
Abstract
Background
Headache is often comorbid with post-traumatic stress disorder yet overlooked in health assessments of refugees.
Objectives
To describe prevalence of severe headache among refugees with post-traumatic stress disorder and compare severity of post-traumatic stress disorder symptoms and treatment outcomes among those with and without severe headache.
Methods
This follow-up study used data from the Danish Database on Refugees with Trauma. Participants were recruited from 2009 to 2015 at a specialized psychiatric clinic. Prevalence of severe headache was computed by age, sex, and history of head injury or torture. Severe headache was defined as maximum headache scores on the Hopkins Symptom Checklist, Symptom Checklist-90 or the Visual Analogue Scale. Groups with and without severe headache were described according to validated questionnaires before and after 12–18 months of multidisciplinary treatment for post-traumatic stress disorder. Regression analyses were used to analyze associations between headache at start of treatment and symptom burden post-treatment, controlled for pre-treatment scores and possible confounders.
Results
Among 403 female and 489 male participants, nearly all (97.5%) complained of headaches. Severe headache prevalence was 31.4% to 50.0% (depending on which questionnaire was used) and was significantly more common among females and those aged 30–49 years. There was no clear relationship between headache and head injury or torture. Participants with severe headache had heavier symptom burdens compared to those without severe headache. Post-treatment, headache prevalence by age and sex did not change significantly. Those without severe headache showed a tendency toward improvement in outcome measures; this was not seen among those with severe headache. Pre-treatment headache scores were correlated with all outcome measures. Regression analyses controlled for pre-treatment scores of the outcome variables showed associations between pre-treatment headache scores (Hopkins Symptom Checklist or Symptom Checklist-90) and post-treatment scores for intrusion, numbing, hyperarousal, anxiety, disability, and quality of life (all p < 0.02).
Conclusion
Headache is a prevalent comorbid condition among refugees with post-traumatic stress disorder. Measures of pre-treatment headache severity appear to predict post-traumatic stress disorder treatment outcomes. Severe headache adversely affects post-traumatic stress disorder prognosis. Assessment and treatment options should be studied further.
Introduction
The United Nations Refugee Agency estimates that there are 26.6 million refugees as of mid-2021 (1). The prevalence of post-traumatic stress disorder (PTSD) among refugees is difficult to study under conditions of ongoing conflict, unstable access to basic needs, and lack of health care services. Refugees could be about ten times more likely to have PTSD than matched general populations in western countries (2). Studies among refugees in various settings report a wide range of PTSD prevalence estimates: from 3% to 86% (2–4).
Headache is a debilitating comorbid condition in many people with PTSD (5–8). Headache disorders by themselves are associated with impaired quality of life (QoL), disability, substantial lost productivity, and high economic costs (9,10). Headache-related disability is greater in the presence of psychiatric comorbidity (11).
Unfortunately, headache is often overlooked in health assessments of refugees possibly because headache is viewed as a relatively minor, non-life-threatening problem. There are therefore very few prevalence studies on headache in refugee populations. A systematic literature search on comorbid chronic pain and PTSD among refugees yielded only 15 studies between 1996 and 2017. Only four estimated headache prevalence; with reports ranging from 50% to 99% (4).
This follow-up study aims to describe the prevalence of severe headache among refugees with PTSD; and to compare severity of PTSD symptoms and treatment outcomes among those with and without severe headache.
We hypothesized a high prevalence of headache in our clinic-based study population. We further hypothesized that those with severe headache would have poorer treatment outcomes compared to those without severe headache.
Methods
Recruitment
The primary data source was the Danish Database on Refugees with Trauma (DART) compiled through integrated clinical research practice at the Competence Centre for Transcultural Psychiatry (CTP), Mental Health Centre Ballerup, a specialized tertiary care clinic in the Capital Region of Denmark (12). Patients referred to CTP are considered particularly complex and require specialized care.
Participants from four recruitment periods were included (2009 to 2011, 2011 to 2012, 2011 to 2015, and 2013 to 2015) (13–17). Inclusion criteria were: aged 18 years or older; referred to CTP for treatment of trauma-related symptoms; recognized as a refugee or family reunified with a refugee; had experienced psychological trauma related to being a refugee (e.g., torture, political persecution, imprisonment, experience of war); and diagnosed with PTSD according to ICD-10 research criteria.
Participants were excluded if they had a psychotic disorder (ICD-10 diagnoses F2x and F30.1–F31.9); abused drugs or alcohol (F1x.24–F1x.26); had been admitted to a psychiatric hospital; or had a physical illness or handicap that would not allow for participation (Figure 1).

Flowchart on participants’ recruitment, inclusion, and withdrawal from the study.
Data collection
Data on headache were gathered uniformly throughout the recruitment periods. Interdisciplinary treatment was carried out using manuals developed specifically for this patient group. Typical treatment duration was 12 to 18 months (12–17).
Baseline clinical and demographic data were gathered by medical doctors (including JC and MLW) and social workers. Information was gathered on age, sex, country of origin, civil status, children (under 18 years), education, work status, and nature of trauma.
Participants filled out self-administered questionnaires on their first and last visits. Questionnaires were available in Danish, English, Arabic, Persian, and Russian. Participants had the option of filling in questionnaires themselves or with the help of a translator.
The following data collection instruments were used:
Harvard Trauma Questionnaire (HTQ)
Sixteen questions on symptoms of PTSD and functional distress were used to quantify trauma-related symptoms (18,19). Responses were coded as (1) not at all, (2) a little, (3) quite a bit, and (4) extremely. Items were analyzed according to four symptom domains adapted from previous studies (20,21):
Intrusion (intrusive thoughts, flashbacks, disturbing dreams, physical or psychological reactions to reminders of trauma) items 1, 2, 3, 16. Avoidance (avoiding activities, thoughts and feelings associated with the traumatic event) items 11 and 15. Numbing (diminished interest, lack of vision for the future) items 4, 5, 12, 13, 14. Hyperarousal (anxious arousal – feeling jumpy, feeling on guard) items 6 and 9; and (dysphoric arousal – difficulty concentrating and sleeping, irritability) items 7, 8 and 10.
A mean score (range 1 to 4) was calculated for each domain and for the total score.
Hamilton Depression and Anxiety Questionnaires
Severity of depression was analyzed using the Hamilton Depression scale (HAM-D) with 17 questions rated from 0 to 2 or 0 to 4 (22,23). Summary scores ranged from 0 to 52.
Severity of anxiety was analyzed using the Hamilton Anxiety scale (HAM-A) with 14 questions rated from 0 to 4 (24). Summary scores ranged from 0 to 56.
Sheehan Disability Scale (SDS) and the WHO Well-being Index (WHO-5)
Disability was measured using three items of the SDS indicating the extent to which symptoms disrupted life in three areas: work/school, social life, and family life. Each domain was scored from 0 to 10, with 0 being no disruption, and 10 being extreme disruption (25).
WHO-5 was used as a measure of QoL (26,27). Five questions were scored from 0 to 5 and summed for a total of 0 to 25. A score from 0 to 100 was calculated by multiplying the raw score by four. Higher numbers represented better QoL. A score below 13 was considered poor well-being.
Hopkins Symptom Checklist (HSCL), Symptom Checklist-90 (SCL-90), and Visual Analogue Scale (VAS)
Portions of the HSCL (28) and SCL-90 (29) were used to identify somatic comorbidities with a one-week recall period.
Participants were asked the following questions related to headache:
“How much did headache bother or distress you in the last week, including today?” Responses were coded as (1) not at all, (2) a little, (3) quite a bit, and (4) extremely. “To which degree did headache bother you in the past week, including today?” Responses were coded as (0) not at all, (1) a little, (2) quite a bit, (3) a lot, and (4) extremely.
Participants were also asked to indicate degree of headache pain in the last four weeks using a VAS score from 0 (none) to 10 (very severe).
Physical injury
Data on head trauma were systematically gathered only from participants enrolled from 2013 to 2015. Participants were asked if they experienced any head injury related to their trauma (yes/no), whether head injuries resulted in loss of consciousness (yes/no), whether they experienced torture (yes/no), number of torture episodes (once, two to five times, more than five times), and duration of exposure to torture (ranging from less than a month to more than five years).
Definition of terms
A case of headache was defined as a report of headache in at least one of three questionnaires: HSCL (score of 2, 3, or 4), or SCL-90 (score of 1, 2, 3, or 4), or VAS (>=1).
Participants most affected by headache were those who reported a maximum HSCL score of 4, SCL-90 score of 4, or VAS 8 to 10. These participants are referred to in this study as suffering from “severe headache”.
Participants recruited into the study had symptoms of PTSD or were given a diagnosis of PTSD by a physician based on ICD-10 criteria. Criterion E (symptom debut within six months of the stressful event) was disregarded because of the complex and repeated nature of participants’ traumatic experiences.
Statistical analysis
Description of study participants
Demographic data were summarized as counts and percentages for the following variables: sex, age, region of origin, migrant status (refugee, family reunification or other), civil status, number of children, living arrangement, education in home country, current work in host country, income source, torture, and head injury related to a traumatic event. Chi-square tests were used to examine headache prevalence among those who experienced head injury or torture.
Headache prevalence and severity before and after PTSD treatment
Reports of headache in the HSCL and SCL-90 were summarized as counts and percentages. VAS scores were summarized as means and standard deviations. VAS scores were also dichotomized as <8 or 8–10, then counts and percentages were calculated.
Prevalence of severe headache was calculated by age, sex, history of physical trauma to the head, and history of torture. Chi-square test was used to examine distributions by sex. Fisher’s Exact test was used to compare distributions by age group. McNemar’s test was used to examine proportions with severe headache by sex and age group pre- and post-treatment.
Distribution according to headache severity pre- and post-treatment was analyzed using Wilcoxon Signed Ranks test.
PTSD treatment outcomes for participants with and without severe headache
Participants were divided into two groups: with and without severe headache according to their responses to the HSCL, SCL-90 and VAS. Symptom burden, disability, and QoL (as measured in four HTQ domains, HAM-A, HAM-D, SDS and WHO-5) were summarized as mean scores for each headache group pre- and post-treatment.
These scores were then compared using t-tests. P < 0.05 was considered significant at the outset. However, we considered analyses using the three headache measures (HSCL, SCL-90 and VAS) as a family of tests. We applied a more stringent cut-off point to avoid Type 1 error because of multiple comparisons. A p-value of <0.05/3, i.e., p < 0.017 was therefore considered significant.
Cohen’s d was used as a measure of effect size.
A correlation matrix was constructed to describe bivariate relationships between pre-treatment headache scores and outcome measures. Pearson’s correlation coefficients were computed. Significant correlations at the 0.05, 0.01 and 0.001 levels (2-tailed) were marked on the matrix.
Regression analyses were then performed to explore these relationships further.
In Model 1, independent variables were pre-treatment headache score and pre-treatment score of the outcome variable. This analysis was done for each questionnaire (i.e., scores for HSCL, SCL-90 and VAS). Model 2 included variables in Model 1 plus age and sex as possible confounding variables. Standardized beta coefficients and tests of significance for the headache variables were computed (level of significance, p < 0.017).
Dropout analysis
Dropouts were defined as those who did not have scores for all three questionnaires on headache symptoms (HSCL, SCL-90 and VAS) at end of study. Characteristics of dropouts were summarized by age, sex, several demographic variables, headache severity, PTSD severity (four HTQ domains), anxiety, depression, disability and QoL. Dropouts were then compared with study completers according to these characteristics using chi-square tests (p < 0.05).
SPSS Statistics 25 (IBM) was used for all statistical analyses.
Ethical considerations
Study protocols used during the four data collection periods were approved by relevant scientific ethics committees and registered as clinical trials (NCT00917397, NCT01362543, NCT01569685, NCT01955538). Informed consent was secured from all participants. Study aims and methods of data management were approved by the Data Protection Agency in accordance with the Privacy Act.
Data from the Danish Database on Refugees with Trauma (DART) were anonymized prior to analysis. MLW and JC had access to the database. Statistical analyses were done by MLW without access to participants’ Central Person Registry numbers or other personally identifiable information.
Results
Description of study participants
A total of 965 persons were enrolled. Among them, 73 were excluded and 892 were included (403 females, 489 males) (Figure 1). Demographic characteristics are summarized in Table 1.
Demographic data on 892 participants.
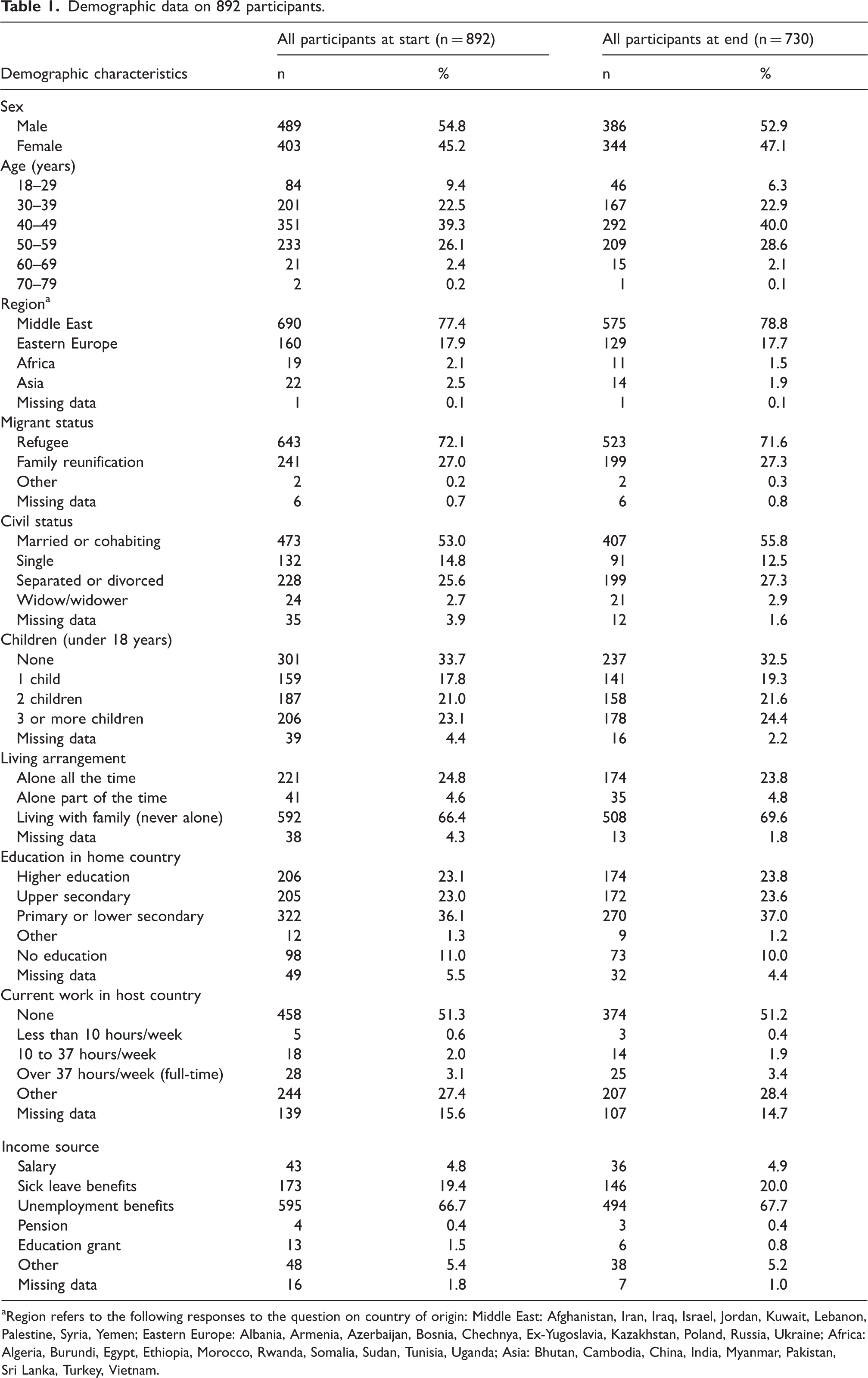
aRegion refers to the following responses to the question on country of origin: Middle East: Afghanistan, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Palestine, Syria, Yemen; Eastern Europe: Albania, Armenia, Azerbaijan, Bosnia, Chechnya, Ex-Yugoslavia, Kazakhstan, Poland, Russia, Ukraine; Africa: Algeria, Burundi, Egypt, Ethiopia, Morocco, Rwanda, Somalia, Sudan, Tunisia, Uganda; Asia: Bhutan, Cambodia, China, India, Myanmar, Pakistan, Sri Lanka, Turkey, Vietnam.
At the start of treatment, 387 participants (43.9%) scored 4 on HSCL and 280 (31.4%) scored 4 on SCL-90 (Table 2). In addition, 430 (50.0%) indicated that their headache was between VAS 8 to 10, with a mean score of 7.0 (SD 2.9).
Participants who reported severe headache based on responses to three questionnaires, by age and sex, before and after treatment for PTSD.

HSCL, Hopkins Symptom Checklist; PTSD, Post-traumatic stress disorder; SCL-90, Symptom Checklist 90; VAS, Visual Analogue Scale. Severe headache refers to maximum scores in the three questionnaires.
P for sex differences were analysed using chi-square test. P for age differences were analysed using Fisher’s Exact test since several cells had expected counts less than 5. P for before and after treatment was analyzed using Mc-Nemar’s test.
*The level of significance is corrected for multiple comparisons, 0.05 divided by 3 tests. P < 0.017 is considered significant.
Table 2 shows that severe headache is significantly more common among females than males (p < 0.001 for all three questionnaires), and most common among 30–49-year-olds compared to other age groups. Age group differences were not consistently statistically significant across the three questionnaires.
Among all 892 participants, 46.2% reported having been tortured. Among 318 participants who were asked systematically about head injury, 41.8% said they experienced head injury related to a traumatic event.
Table 3 summarizes the proportion of participants who reported severe headache according to history of head injury and torture. Prevalence of severe headache was similar for those with or without a history of head injury: (p > 0.017 for all three questionnaires). Prevalence was generally higher among those who experienced head injury with loss of consciousness compared to those who did not lose consciousness, but the differences did not reach statistical significance. Prevalence of severe headache was similar for those who reported torture and those who did not: (p > 0.017 for all three questionnaires). For those who experienced torture, there was no clear trend in headache complaints according to number or duration of torture episodes.
Proportions of participants with severe headachea at start of treatment according to history of head injury and torture.
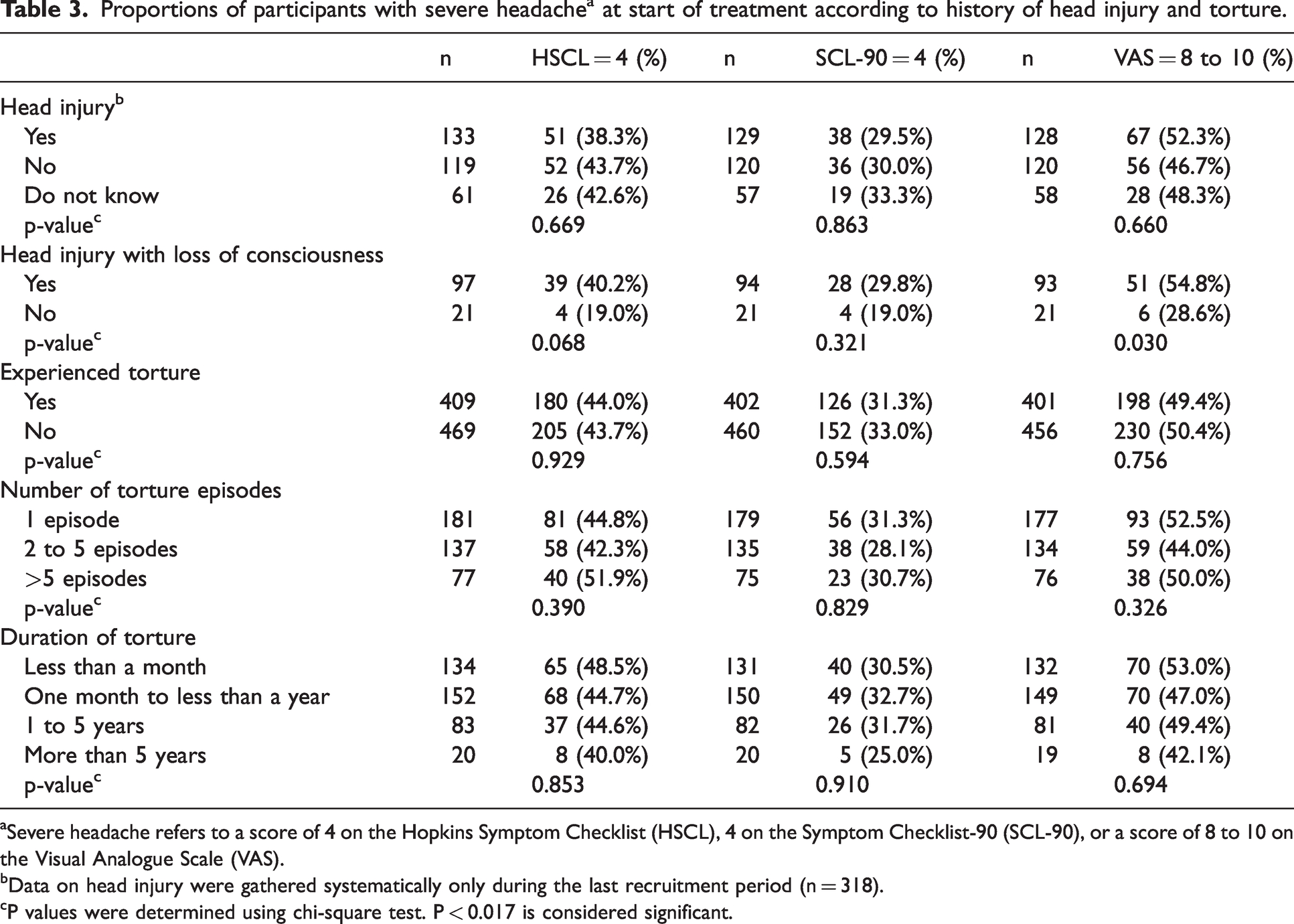
aSevere headache refers to a score of 4 on the Hopkins Symptom Checklist (HSCL), 4 on the Symptom Checklist-90 (SCL-90), or a score of 8 to 10 on the Visual Analogue Scale (VAS).
bData on head injury were gathered systematically only during the last recruitment period (n = 318).
cP values were determined using chi-square test. P < 0.017 is considered significant.
Headache prevalence and severity before and after PTSD treatment
At baseline, headache was reported by 97.5% (870 of 892 participants) in at least one of three symptom questionnaires (HSCL, SCL-90, or VAS). Post-treatment, prevalence was 97.4% (711 of 730 participants).
There was no significant change in prevalence of severe headache after treatment for all age and sex categories (all p > 0.017, Table 2).
Using HSCL, 172 had a better rating post-treatment, 146 had a worse rating, and 402 remained unchanged (p = 0.009). Using SCL-90, 194 had a better rating post-treatment, 188 had a worse rating, and 315 remained unchanged (p = 0.095). Pre-treatment VAS scores for all those with headache (i.e., excluding those who scored 0) were extremely high, with a mean of 7.1 (SD = 2.8). Post-treatment, the mean for all with headache decreased slightly to 6.9 (SD = 2.9); 305 had a better score post-treatment, 339 had a worse score, and 45 remained unchanged (p = 0.084).
PTSD treatment outcomes for participants with and without severe headache
Pre- and post-treatment, participants without severe headache had better scores compared to those with severe headache in all assessments of PTSD, anxiety, depression, disability, and QoL. Pre-treatment, differences between the two headache groups were statistically significant except for numbing (in all three questionnaires) and avoidance (HSCL and VAS) (Table 4a). Post-treatment, the gap in scores of the two groups appeared to widen and all comparisons showed statistically significant differences (Table 4b).
Scores for severity of psychiatric symptoms, disability, and quality of life among participants with and without severe headache at start of treatment.

Scores for severity of psychiatric symptoms, disability, and quality of life among participants with and without severe headache at end of treatment.
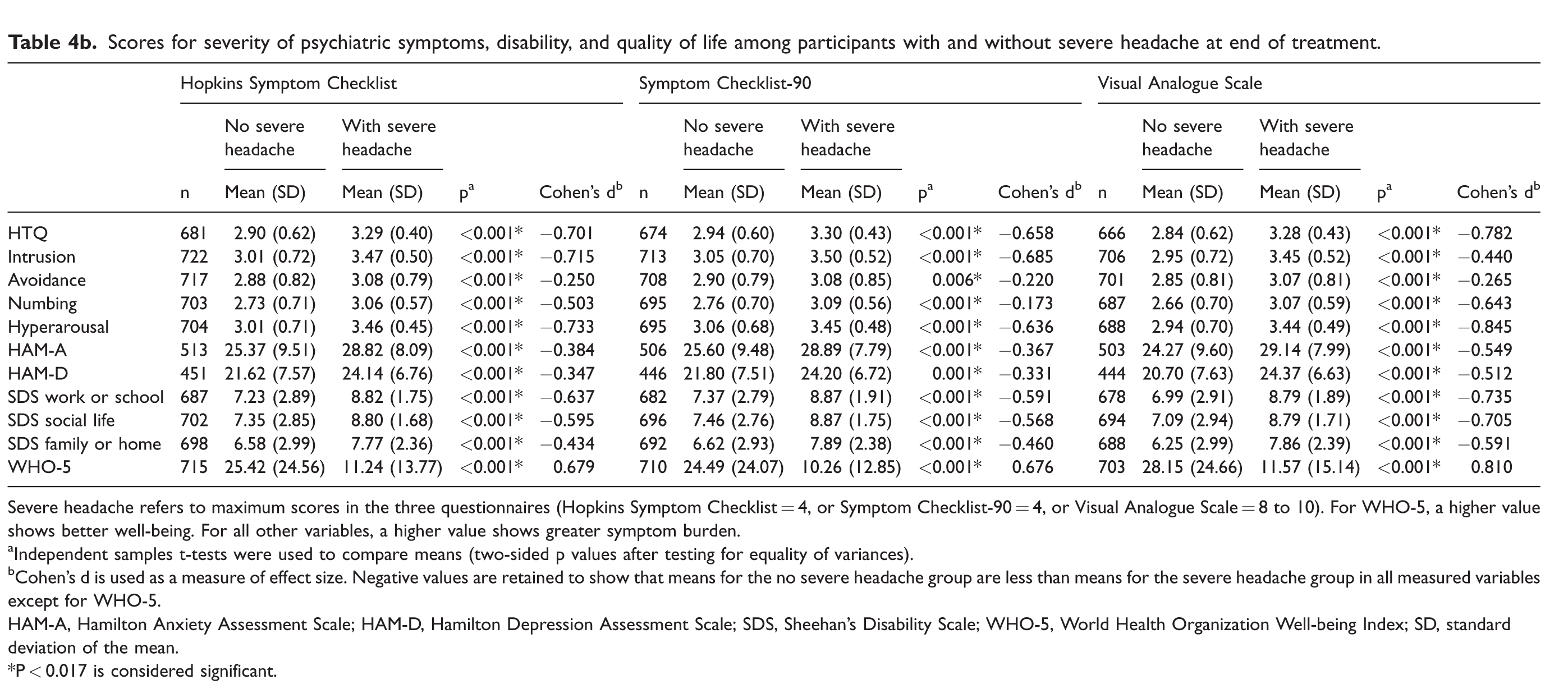
Severe headache refers to maximum scores in the three questionnaires (Hopkins Symptom Checklist = 4, or Symptom Checklist-90 = 4, or Visual Analogue Scale = 8 to 10). For WHO-5, a higher value shows better well-being. For all other variables, a higher value shows greater symptom burden.
aIndependent samples t-tests were used to compare means (two-sided p values after testing for equality of variances).
bCohen’s d is used as a measure of effect size. Negative values are retained to show that means for the no severe headache group are less than means for the severe headache group in all measured variables except for WHO-5.
HAM-A, Hamilton Anxiety Assessment Scale; HAM-D, Hamilton Depression Assessment Scale; SDS, Sheehan’s Disability Scale; WHO-5, World Health Organization Well-being Index; SD, standard deviation of the mean.
*P < 0.017 is considered significant.
Intrusion and hyperarousal showed strong effect sizes pre-treatment (Cohen’s d > 0.500, Table 4a). Post-treatment, in addition to intrusion and hyperarousal, QoL and several disability scores also showed high effect sizes (Cohen’s d > 0.500, Table 4b). The largest differences between group means were seen in hyperarousal and WHO-5 scores post-treatment (Cohen’s d > 0.800 for VAS scores, Table 4b).
Bivariate correlations were computed using pre-treatment headache scores and outcome measures (Table 5). The three questionnaires were strongly correlated with each other (correlation coefficients >0.600). All headache scores were significantly correlated with outcomes, except in the case of HSCL and avoidance. The coefficients were positive, i.e., higher pain scores correlated with higher scores on the outcome measures, indicating worse outcomes. The exceptions were correlations with WHO-5, which showed negative coefficients since high pain scores correlated with lower QoL. The strengths of the relationships were low (correlation coefficients <0.300), but the analyses likely had enough statistical power to identify even these weak effects.
Correlation matrix showing bivariate relationships between headache scores at start of treatment and outcome measures at end of treatment.

All values are Pearson correlation coefficients. The strongest correlations (>0.500) are highlighted.
HAM-A, Hamilton Anxiety Assessment Scale; HAM-D, Hamilton Depression Assessment Scale; HTQ, Harvard Trauma Questionnaire; HSCL, Hopkins Symptom Checklist; SCL-90, Symptom Checklist-90; SDS, Sheehan’s Disability Scale; VAS, Visual analogue scale; WHO-5, World Health Organization Well-being Index.
*Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2-tailed). *** Correlation is significant at the 0.001 level (2-tailed).
Regression analyses were performed using pre-treatment headache score as the independent variable and the various outcome measures as dependent variables (Table 6).
Regression analyses showing relationships between headache (at start of treatment) and treatment outcome.

Coeff B, Standardized beta coefficients for headache as an independent variable; HAM-A, Hamilton Anxiety Assessment Scale; HAM-D, Hamilton Depression Assessment Scale; HSCL, Hopkins Symptom Checklist; HTQ, Harvard Trauma Questionnaire; SCL-90, Symptom Checklist-90; SDS, Sheehan’s Disability Scale; VAS, Visual analogue scale; WHO-5, World Health Organization Well-being Index.
*The level of significance is corrected for multiple comparisons, 0.05 divided by 3 tests. P < 0.017 is considered significant.
Model 1 was adjusted for the baseline score of the outcome variable and showed significant relationships between pre-treatment headache score (HSCL and SCL-90) and post-treatment intrusion, numbing, hyperarousal, anxiety, disability, and QoL. Similar results were seen in Model 2, which was additionally adjusted for age and sex. The relationships between headache scores and HTQ, intrusion and numbing were significant in all three questionnaires after these adjustments.
Results for HSCL and SCL-90 analyses were similar. In analyses using VAS scores, only HTQ, intrusion and numbing, were significant (p < 0.017), although several analyses for disability and QoL had p-values <0.05 (Table 6). Overall, results appeared to indicate that severe headache complaints at start of treatment predicted poor outcomes.
Dropout analysis
There were 162 participants lost to follow up (18.2%) while 730 (344 females and 386 males) completed treatment. Dropouts were disproportionately male (21.1% vs. 14.6% among females, p = 0.013), under 30 years old (45.2% dropout) or over 60 years old (30.4% dropout, p < 0.001). There were also significant differences in schooling and work profiles (p < 0.042); with a higher proportion of dropouts enrolled in education programs (4.6%) compared to completers (0.8%).
The proportion of those with severe headache was similar for dropouts and completers in the three questionnaires (p = 0.056 for HSCL, p = 0.299 for SCL-90, and p = 0.060 for VAS).
Regarding PTSD symptoms, those who dropped out had less severe avoidance scores at baseline (mean 3.04) compared to completers (3.19; p = 0.024). Differences in intrusion scores were marginally significant (p = 0.041). There were no significant differences according to severity of numbing (p = 0.157) and hyperarousal (p = 0.246).
Disability scores were similar for dropouts and completers (p = 0.151 for work/school, p = 0.288 for social life, and p = 0.102 for family life). However, dropouts had significantly better scores on HAM-A (p = 0.010), HAM-D (0.002), and WHO-5 (p = 0.023).
Discussion
Severe headache was highly prevalent in this study population of refugees with PTSD. Severe headache was more common among women and the middle aged. There was no clear relationship with head trauma and torture episodes. The group with severe headache had significantly heavier symptom loads for PTSD, anxiety, and depression; had higher disability scores; and poorer QoL.
Prevalence of severe headache (by age and sex) did not significantly change after treatment for PTSD. Regression analyses using HSCL or SCL-90 (but not VAS) as measures of headache severity showed that pre-treatment headache appears to predict symptoms of intrusion, numbing, hyperarousal, anxiety, disability, and QoL post-treatment.
Severe headache comorbid with PTSD
In the general population, one-year prevalence of any headache is between 24 to 79% (10). The prevalence of tension-type headache (TTH) is 26.1%, and migraine 14.4% (9). Yet in this study population of refugees with PTSD, point prevalence (one- or four-week recall) of any headache was 97.4%, and depending on the questionnaire used, 31.4 to 50.0% reported severe debilitating headaches.
Headache prevalence differs between local and immigrant populations. Onset or worsening of headache often occurs after immigration, which likely reflects the stress of displacement: uncertain access to basic needs, sleep disturbances, comorbid psychiatric illness, lower access to medical care (due to language barriers or socio-cultural factors), and differences in medication use (30). Neglecting headache diagnosis and treatment among migrants and refugees likely contributes to increased burden of headache worldwide.
Estimating prevalence of comorbid PTSD and pain among refugees is difficult because of the fluidity of the population, multiple traumatic experiences, and limited access to regular health care where psychological and physical health can be assessed. A review of 15 studies on PTSD and pain among refugees shows heterogenous research settings, cultural groups, and phases of integration into host countries (4). Published papers are mainly on people with a refugee background resettled in Western countries (31), where 85.7% of those with PTSD report head pain, compared to only 14.3% among those not diagnosed with PTSD.
General health assessments in primary care settings report lower headache prevalence compared to clinic-based studies. A study of newly arrived Syrian refugees in Norway surveyed 827 adults for physical and mental health problems. Headache was the most prevalent illness, reported by 22% (32). Among refugees treated at a psychiatric center in Norway, however, 98% reported chronic pain in at least one location, with the most prevalent location being the head (80%) (31).
Similarly, in Denmark, a study of 160 newly resettled refugees showed that 54% reported headache during their general health assessment (33). Among refugees with PTSD treated at our psychiatric center, prevalence of headache is much higher: 97.4%. Analysis of a subset of participants included in this study (168 women and 150 men), showed that high pain scores along with chronicity of PTSD symptoms predicted poor treatment response (34).
Our findings support research showing associations between chronic pain and PTSD (6,33,35); as well as high prevalence of PTSD among persons with headache in general (5) and migraine in particular (7,8).
There is high comorbidity between traumatic brain injury, headache, and PTSD (36–38). In our study, severe headache was more common among those who experienced head injury with loss of consciousness. A study of asylum seekers in the US showed that almost half (42.5%) reported a history of head injury, which is similar to our finding of 40.2% for HSCL (39).
Our findings on poor outcome of treatment for those with severe headache, align with observations from a recent study of refugees who experienced torture or trauma (40). Improvement in PTSD symptoms was observed after treatment, but not pain severity or pain interference (i.e., how pain affects daily functioning). As expected, higher levels of pain interference predicted poorer outcomes.
The current study shows that severe headache could be an effect modifier, where the effect of treatment for PTSD on an outcome variable (improvement in PTSD symptoms) differs depending on the presence or absence of a third variable (severe headache or more generally, pain).
Severe headache could be a marker for PTSD that is refractory to usual treatment. Severe headache in a person with PTSD could be associated with higher pain intensity in other parts of the body, pain catastrophizing, depression, anxiety, disability, higher pain medication use, and lower self-efficacy, all these leading to low QoL (35,40,41).
There are several explanatory theories on the link between chronic pain and PTSD (42), all pointing to shared pathophysiological mechanisms of these two conditions, and maladaptive changes or abnormalities in the somatosensory and cerebral systems (36,43,44).
Pain may trigger memories of trauma. Sensory reexperiencing symptoms of PTSD could include pain (36). Stressful life events (e.g., job loss, divorce, major illness) not necessarily related to previous trauma could lead to pain and PTSD-like symptoms in someone with an existing vulnerability (45).
Implications for diagnosis and treatment
Assessment of pain in patients diagnosed with PTSD is important in treatment and prognostication. Pain self-report questionnaires (e.g., Brief Pain Inventory, the Pain Catastrophizing Scale, or the Short Form McGill Pain Questionnaire) could be used to gather more information (35,45). Characterizing headache pain as being caused by tension, migraine, medication overuse, or physical trauma, could be the starting point for education and appropriate treatment.
The group without severe headache – representing the majority of participants who completed treatment – showed improvement. This is a positive finding for this group of refugees with PTSD, whose symptoms required specialized treatment.
Among people with chronic pain, avoidance contributes to maintenance of PTSD; and among those with PTSD, avoidance contributes to maintenance or aggravation of chronic pain (31). Reduction in avoidance behavior after treatment is maybe the first sign of improvement. Available data do not allow for much optimism, however. A 10-year study of 139 tortured refugees resettled in Denmark reported a 47.5% prevalence of head pain at baseline, and 58.3% at follow-up (46), representing a clear challenge to treatment programs.
There are very few studies on effective treatments for comorbid chronic pain and PTSD. Cognitive behavioral therapy (CBT), Acceptance and Commitment Therapy (ACT), Narrative Exposure Therapy (NET) with biofeedback, Cognitive Processing Therapy (CPT), prolonged exposure, manualized trauma psychotherapy, Traditional Chinese Medicine (TCM) and Emotional Freedom Techniques have been evaluated with positive outcomes for both pain severity and PTSD symptoms (4,35), although these methods do not focus specifically on headache pain.
Since research points to a common underlying mechanism that explains comorbid pain and PTSD, an integrated treatment approach for both conditions might be more effective (36,47). Headache treatment will likely support improvement of PTSD symptoms. Non-pharmacological treatment of TTH – such as stress management and relaxation techniques – can also alleviate symptoms of PTSD. Preventive medications for TTH recommended by the Danish Headache Society include amitriptyline, mirtazapine, and venlafaxine (48), which are, perhaps not coincidentally, among the medications used for treatment of PTSD symptoms at our psychiatric center.
Improved treatment of headache comorbidity could improve PTSD outcomes. Treatment of migraine reduces symptoms of depression and anxiety and improves associated sleep problems and fatigue (49). Treatment of debilitating medication overuse headache (MOH) reduces anxiety, depression, and disability (50). Treatment of chronic post-traumatic headache shows some degree of psychological improvement and slightly better QoL compared to a control group, even if there is no significant improvement in headache and pain parameters (51).
Strengths and limitations
This study is the largest so far conducted on headache in a clinic-based population of migrants and refugees diagnosed with PTSD. Data were gathered consistently across several recruitment periods. Study participants were previously examined by health professionals in primary or secondary care before being referred to specialist care at a tertiary center with a working diagnosis of PTSD. Symptoms of PTSD were then assessed uniformly by medical doctors.
The questionnaires on PTSD, anxiety, depression, pain, and QoL are all previously validated and widely used (18,19,22–29) These have also been validated for refugee populations (52).
A limitation is that headache was not characterized according to location, duration, precipitating/relieving factors, and associated symptoms. Specific headache diagnoses could not be made, although these were most likely TTH, migraine, post-traumatic headache, or MOH (53). The case definition for severe headache does not conform to current diagnostic criteria (53).
Bivariate analyses show that HSCL, SCL-90 and VAS are strongly correlated. However, during preliminary analyses, we found differences in the numbers of participants who reported high scores for headache in these three questionnaires. This made it difficult to choose just one instrument to describe the group most affected by headache, assuming the three instruments are equally valid. Ideally, a validated headache diagnostic questionnaire should be used, and the participants asked to fill in a headache diary.
A sum score for all three questionnaires was considered, but without validation, cut-off scores for what constituted severe headache would have been arbitrary. Analyzing all three questionnaires increased the number of statistical analyses performed, which increased the risk of Type 1 error. We attempted to decrease the error risk by using a lower p-value to indicate statistical significance.
Regression analyses using VAS scores showed fewer significant associations, possibly because of a ceiling effect, where a high percentage of participants scored near the maximum and therefore linear models are not appropriate. Severity of headache was based on one-week recall for HSCL and SCL-90; and four weeks for VAS. This might also account for the differences in the results.
Information on prescription pain medications was gathered systematically only for the last 318 participants, and only at baseline. The most common pain medications prescribed were paracetamol (111 participants), tramadol (39 participants) and triptans (20 participants). They were not systematically asked about use of over-the-counter pain relievers nor misuse of opiates, the latter being more prevalent among patients with PTSD (35,54). In a recent Norwegian study of newly arrived refugees, 21% of those who reported headaches used painkillers every day (32). It was not possible to diagnose MOH which was likely prevalent in this study population.
Participants represent the most severe cases of PTSD requiring referral to a highly specialized center. Their responses to the questionnaires were mostly in the severe end of the scales. Our findings are not generalizable to all groups of migrants and refugees.
Data were anonymized after inclusion. It was not possible to rule out repeated inclusion of the same patient during different recruitment periods. If this occurred, this would have accounted for a very small number of participants. Demand for services is high, and those who had already been through a full treatment program were not prioritized for repeat inclusion.
Finally, a sensitivity analysis of the effect of dropout was not done. We suspect that those who dropped out chose to prioritize work or school and were probably more able to function in these settings because of lower avoidance (and possibly intrusion) scores. This group had a lighter symptom burden for anxiety and depression. They reported better well-being even though their disability scores were similar to those who completed treatment.
The proportion of those with severe headache was similar for dropouts and completers in the three questionnaires. It is therefore less likely that results were biased by missing headache data. However, it is possible that we underestimated the degree of improvement for those without severe headache.
Several questionnaires were not completely filled in by participants, and some did not attend a separate session for HAM-A and HAM-D interviews conducted by blinded interviewers. This aspect of data collection could be improved. We chose to present the results as recorded, rather than impute missing data.
Conclusion
Headache is a highly prevalent comorbid condition in this group of migrants and refugees referred to a specialized center for treatment of symptoms of PTSD. Those with severe headache presented with higher symptom burden, more disability, and lower QoL; and showed little improvement post-treatment likely because of mutual maintenance of PTSD and headache disorders. Measures of pre-treatment headache severity appear to predict PTSD treatment outcomes. Assessment and treatment options for these debilitating comorbid conditions should be studied further.
Clinical implications
This study on refugees with PTSD shows that assessment of headache is important in treatment and prognostication. Severe headache adversely affects PTSD prognosis. Improved treatment of headache comorbidity might improve PTSD outcomes. Since research points to a common underlying mechanism that explains comorbid pain and PTSD, an integrated treatment approach for both conditions might be more effective.
Footnotes
Acknowledgements
The authors thank the clinical and research staff and secretaries at the Competence Centre for Transcultural Psychiatry, Erik Lykke Mortensen for invaluable advice on statistical analysis, and most of all, our patients through the years who contributed their time and engagement, knowing that their efforts would help improve the treatment of psychiatric illness among migrants and refugees.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection for the Danish Database on Refugees with Trauma (DART) has been ongoing since 2009. Funds were received from TrygFonden under grant numbers 7-10-1002 and 102265 URL: ![]() . The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.