
Abstract
Aim
To identify factors that may be predictors of the outcome of a detoxification treatment in medication-overuse headache.
Methods
Consecutive patients entering a detoxification program in six centres in Europe and Latin America were evaluated and followed up for 6 months. We evaluated anxious and depressive symptomatology (though patients with severe psychiatric comorbidity were excluded), quality of life, headache-related disability, headache characteristics, and prophylaxis upon discharge.
Results
Of the 492 patients who completed the six-month follow up, 407 ceased overuse following the detoxification (non overusers), another 23 ceased overuse following detoxification but relapsed during the follow-up. In the 407 non-overusers, headache acquired an episodic pattern in 287 subjects (responders). At the multivariate analyses, lower depression scores (odds ratio = 0.891; p = 0.001) predicted ceasing overuse. The primary headache diagnosis – migraine with respect to tension-type headache (odds ratio = 0.224; p = 0.001) or migraine plus tension-type headache (odds ratio = 0.467; p = 0.002) – and the preventive treatment with flunarizine (compared to no such treatment) (odds ratio = 0.891; p = 0.001) predicted being a responder. A longer duration of chronic headache (odds ratio = 1.053; p = 0.032) predicted relapse into overuse. Quality of life and disability were not associated with any of the outcomes.
Conclusions
Though exploratory in nature, these findings point to specific factors that are associated with a positive outcome of medication-overuse headache management, while identifying others that may be associated with a negative outcome. Evaluation of the presence/absence of these factors may help to optimize the management of this challenging groups of chronic headache sufferers.
Introduction
Discontinuation from the overused drug is the first step in the management of medication-overuse headache (MOH), being effective in reverting the headache pattern from chronic to episodic in the majority of patients (1). However, in a minority of MOH patients, drug withdrawal is unsuccessful either because they fail to actually interrupt drug overuse or because overuse discontinuation is not associated with an improvement of headache (2–4). Thus, the identification of the factors associated to a positive or negative outcome of a withdrawal treatment in subjects with MOH seems critical. Psychiatric comorbidities, such as anxiety and depression, are often associated with frequent headache and medication overuse (5,6). The same is also true for poor quality of life (QoL) and high headache-related disability (7–9). In this frame, it is interesting to understand whether some of these factors actually have an impact on the response to the detoxification treatment. Several authors (10–23) have explored the association that exists between such factors and the effects of the treatment, mostly recruiting MOH patients in specialized headache clinics. However, it must be noted that the results of these studies are hardly comparable because they differ in terms of sample size, selected outcomes and duration of follow-ups. In general, detoxification interventions are able to produce benefits on patients’ affective state (10–13), QoL (11–14), and disability levels (10,12–13,15). When investigating those variables associated with the outcome of withdrawal therapy, an observational prospective study conducted on a small MOH population showed that poor QoL and high scores of depression and anxiety at baseline correlated with frequent headaches 6 months after withdrawal (11). Raggi (16) found in an observational longitudinal study that baseline self-reported depression, but not QoL or headache-related disability, was associated with relapse into MOH and need for another treatment at 1 year. Caproni (17), in a post-hoc analysis from the SAMOHA study, showed that quality of life – but not headache-related disability – before treatment (detoxification plus sodium valproate) was associated with poor response at 3 months. Bøe (18) confirmed this finding in a 1-year follow-up. Authors in this prospective study also included the Hospital Anxiety and Depression Scale (HADS) (19) for assessing depressive symptomatology, but in this case failed to find any association between affective state and detoxification outcome. Another prospective cohort study (20) found that headache-related disability (the authors did not evaluate patients’ affective state or QoL) was an independent predictor of treatment efficacy at 1-year follow-up. Finally, in a recent retrospective study, higher depression scores and disability levels as well as lower QoL were associated with frequent relapses; that is, need for two or more structured withdrawals within three years (21). At variance, there is also evidence of a lack of association between these variables and the outcome of treatment. A couple of Italian retrospective (22) and prospective (12) studies failed to find any relation between baseline affective state and headache disability and risk of relapse into overuse at 1-year follow-up. Similarly, a small longitudinal Chinese study (23) showed a lack of association between patients’ psychological state two months after detoxification and the outcome itself 7.5 months later.
Taken together, all these findings are interesting as they show the importance of considering psychiatric comorbidities, QoL and migraine disability together with clinical variables with respect to the outcome of the detoxification. However, the heterogeneity and limitations described above do not allow definite conclusions. The COMOESTAS project is a multicentric multinational prospective study that provides a large and well characterized population of MOH subjects who underwent detoxification and were followed up for 6 months (24–27). In a previous analysis of the COMOESTAS population, we observed that detoxification had a general positive impact on anxious and depressive symptomatology (26). A subsequent post-hoc analysis showed that the observed improvement was driven by the success of treatment (27); that is, it was more evident in those subjects who became overuse-free, but it was also dependent on the affective state, being the best outcome after detoxification observed in the subjects with lower depressive symptomatology. These observations suggested the importance of exploring the association between psychological variables and the outcome of detoxification, considering also a possible mutual interplay with clinical and therapeutic factors. Hence, in the present study, for the first time, we report a post-hoc analysis of the COMOESTAS database aimed at evaluating in more depth the association existing among symptoms of anxiety and depression, QoL, headache-related disability, headache characteristics, preventive treatments, and detoxification outcome.
Methods
Participants and study design
Design and results of the COMOESTAS project have been described elsewhere (24–27). It was a study aimed at comparing the outcomes six months after detoxification between MOH patients monitored with an electronic (IEPR) or a paper diary (25). Patients with MOH according to the ICHD-3 beta criteria (28) were recruited consecutively from August 2008 to February 2009 in six headache centers: Four in Europe (Italy, Denmark, Germany, and Spain) and two in Latin America (Argentina and Chile). Patients affected by severe psychiatric comorbidities; that is, those who scored ≥15 on the HADS scale (29) or who required psychiatric evaluation and treatment in the physician’s opinion, were excluded. This exclusion criterion was adopted in the COMOESTAS project to limit the possibility of including subjects suffering from headache associated with psychiatric comorbidities, and to improve the homogeneity of the population under investigation. All patients underwent drug withdrawal followed by optional prophylactic treatment, according to a consensus protocol published elsewhere (24) and were followed up for 6 months.
Procedures
The procedures adopted have been explained in detail elsewhere (23–27). Briefly, at visit 0, patients were informed individually about the role of acute drugs in causing medication-overuse headache, the treatment program and the need to keep a headache diary. One month later, at visit 1 (Day 0), the headache diary was checked, patients were included in the study and underwent detoxification either as inpatients or as outpatients. Detoxification lasted 7 days and consisted of the abrupt discontinuation of overused acute medications, which were substituted by rescue medications. As of Day 8, the patients were allowed only two days/week with symptomatic medications different from the overused ones. Prophylactic treatment was optional; when prescribed, it was started on Day 1. At visit 2 (two months after day 0) patients returned to the headache center for a follow-up visit. Visit 3 (6 months after day 0) completed the study.
Given the size of this study, depressive and anxious symptomatology, QoL and headache-related disability were evaluated by means of self-reported questionnaires, adopted as the best trade-off between data quality and resource usage. More specifically, we used HADS (19) for scoring the levels of depressive and anxious symptomatology, WHOQoL (30) for assessing QoL, and Migraine Disability Assessment (MIDAS) (31) for measuring headache-related disability. The study was approved by the local Ethics Committees from all centers except Denmark, where approval was not necessary because the study did not foresee any new pharmacological treatment. Participants gave informed consent before taking part.
Data management
We collected clinical data by means of a dedicated web-based platform (the COMOESTAS platform). All centres were required to perform data entry in real time. Data input was continuously monitored by the coordinating centre (the Mondino Institute).
Endpoints and statistical analysis
For data analysis, we adopted the following possible outcomes (24–25):
1. Non-overusers: Subjects who were overuse-free at both 2 months and 6 months 2. Responders: A subset of non-overusers who had less than 15 headache days/month during the entire 6-month observation period 2a. 50% responders: A subset of responders with a 50% reduction in headache attacks during the entire 6-month observation period 2b. Optimal responders: A subset of responders with a 75% reduction in headache attacks during the entire 6-month observation period 3. Relapsers: Subjects who were overuse-free at 2 months but relapsed back into overuse at any month between 3 months and 6 months.
Descriptive characteristics and predictors of being a non-overuser.
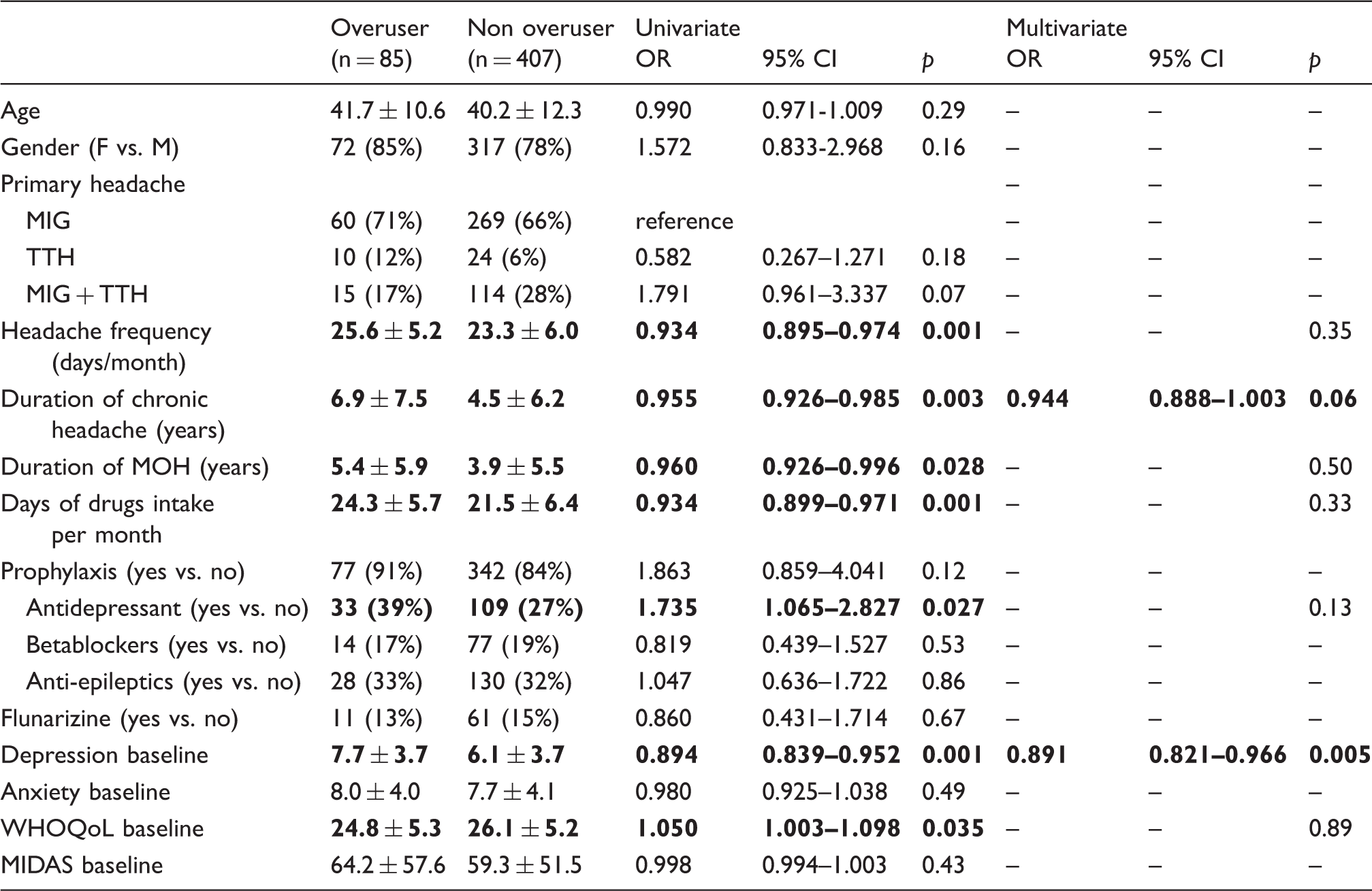
MIG: Migraine; TTH: tension-type headache. Significant odds ratio (OR) in bold.
Results
Patient population
Of the 663 patients with MOH included in the study, 492 (74%) completed the study. Our analysis was restricted to the population formed by this latter group. As represented in Figure 1, a total of 407 (83%) subjects were non-overusers, that is, they persistently discontinued overused medications for the entire six-month observation period; 23 (5%) subjects relapsed into drug overuse during the 6-month follow-up and 62 (13%) failed to discontinue overused medications. Among the 407 non-overusers, 287 (71%) were responders; that is, overuse-free and with less than 15 headache days/month, whereas 120 (30%) were still experiencing a chronic headache pattern (partial responders). Two hundred and ninety non-overusers (71%) were qualified as 50% responders. Among these latter, 132 patients (55%) reached at least a 75% reduction of headache days with respect to baseline.
1. Factors associated with the outcome ‘being a non-overuser’
Study diagram according to the exploratory outcomes considered. These are indicated in shaded boxes on the left side of the diagram.

Characteristics of overusers and non-overusers and the results of the univariate analysis are reported in Table 1. In the multivariate analysis, the only factor associated with this outcome was having lower HADS depression scores (OR 0.891; p = 0.005). This logistic regression model was statistically significant (p < 0.001) and it explained 10.5% (Nagelkerke R2) of the variance of ceasing overuse six months from detoxification and correctly classified 83.3% of cases.
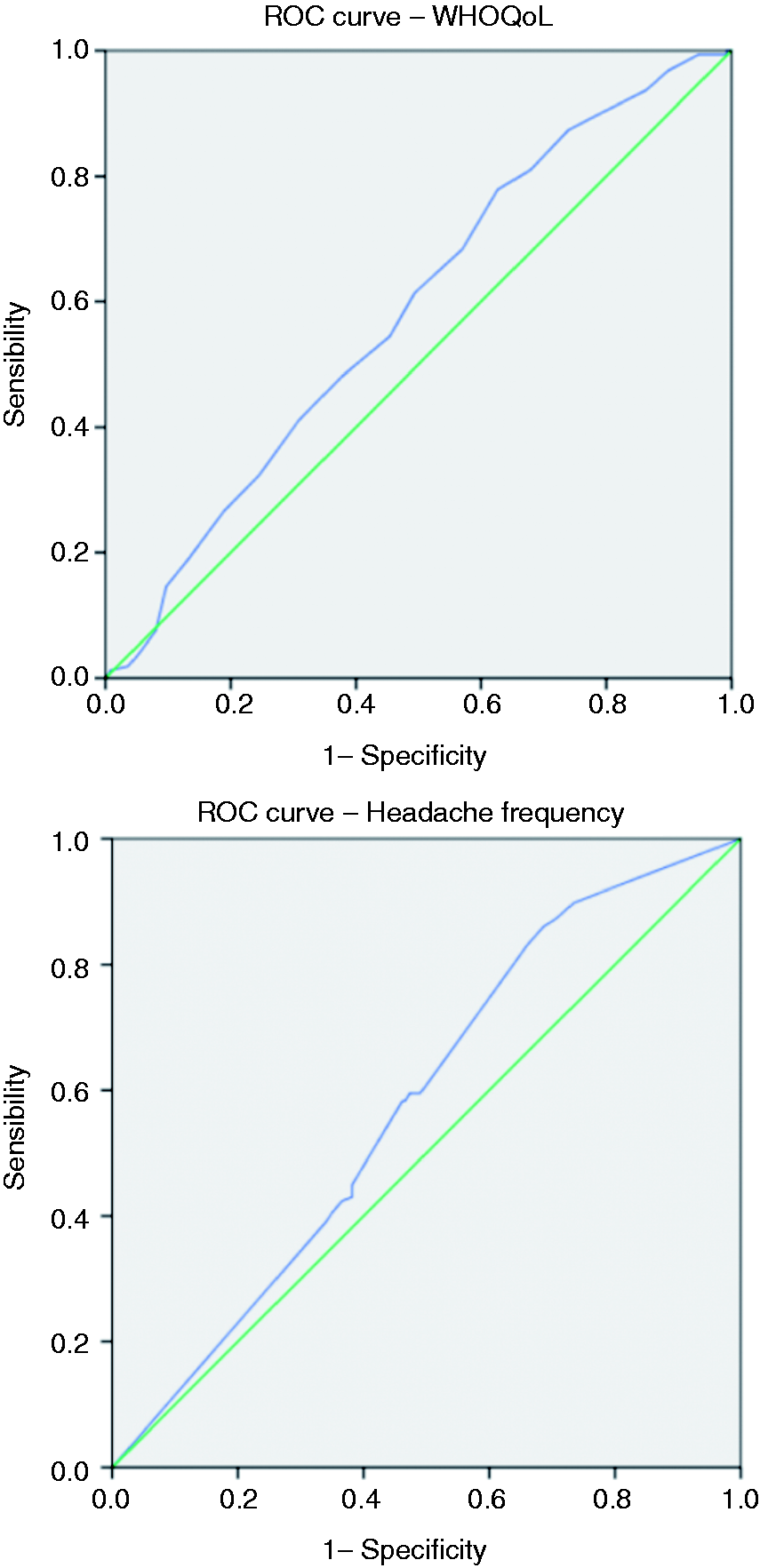
The ROC curve and the AUC were measured for depressive symptomatology and duration of chronic headache (Figure 2). For the HADS depression score, the optimal cut-off point was achieved at 8 (7.5+) with an AUC of 0.625 (0.559–0.690, p < 0.001). This model has a fair sensitivity (65.6%), but a low specificity (39.3%). For the duration of chronic headache, the optimal cut-off point was achieved at 7.5 years with an AUC of 0.604 (0.540–0.666, p = 0.003), which would classify correctly 83.5% of non-overusers (sensitivity) and 60.7% of overusers (specificity).
Receiver Operating Characteristics (ROC) curve analysis of HADS depression scores and chronic headache duration used to identify patients ceasing overuse.
Insert Figure 2
2. Factors associated with the outcome ‘being a responder’
Descriptive characteristics and predictors of being a responder (≤15 days/month headache attacks).

MIG: Migraine; TTH: tension-type headache. Significant OR in bold.
Here, we did not measure the ROC curve or the AUC given the lack of differences in the continuous variables.
2a. Factors associated with the outcome ‘being a 50% responder’
Descriptive characteristics and predictors of being a responder with at least a 50% reduction in headache frequency.

MIG: Migraine; TTH: tension-type headache. Significant OR in bold.
The ROC curve and the AUC were measured for days of drugs intake, which were not significant (p = 0.062).
2b. Factors associated with the outcome ‘being an optimal responder’
Descriptive characteristics and predictors of being an optimal responder (≥75% headache frequency).

MIG: Migraine; TTH: tension-type headache. Significant OR in bold.
The ROC curve and the AUC were measured for WHOQoL scores and headache frequency (Figure 3). For WHOQoL, the optimal cut-off point was achieved at 23.5 with a very low AUC of 0.585 (0.359-0.470, p = 0.004) and low sensitivity (37.3%) and specificity (22.2%). For headache frequency, the optimal cut-off point was achieved at 23.5 with an AUC of 0.580 (0.524–0.635, p = 0.007), which would classify correctly 54.2% of optimal responders and 42.4% of non-optimal responders.
3. Factors associated with the treatment outcome ‘being a relapser’
Receiver Operating Characteristics curve analysis of WHOQoL scores and headache frequency used to identify optimal responders.
Descriptive characteristics and predictors of being a relapser.

MIG: Migraine; TTH: tension-type headache. Significant OR in bold
The ROC curve and the AUC were measured for HADS depression scores, WHOQoL scores and duration of chronic headache (Figure 4). For HADS depression scores, the optimal cut-off point was achieved at 11 (10.5+) with an AUC of 0.654 (0.534–0.774, p = 0.013), which would correctly classify 86.5% of relapsers and 56.5% of non-relapsers. For WHOQoL, the optimal cut-off point was achieved at 27.5 with an AUC of 0.656 (0.556–0.755, p = 0.012), which would correctly classify 82.6% of relapsers and 58.2% of non-relapsers. For the duration of chronic headache, the optimal cut-off point was achieved at 7.5 years of duration with an AUC of 0.641 (0.525–0.758, p = 0.023), which would correctly classify 83.5% of relapsers and 56.5% of non-relapsers.
Receiver Operating Characteristics curve analysis of HADS depression scores, WHOQoL scores and chronic headache duration used to identify relapsers.
Discussion
This study provides the analysis of the associations of a multitude of variables with the outcome of careful management of MOH (24–27) conducted in a multicentric, multinational population. The effect of these variables was evaluated against different pre-specified levels of outcomes; that is, having simply ceased abuse (non-overusers), having also achieved an episodic pattern of headache (responders), and having relapsed into overuse (relapsers). Furthermore, response was further subdivided into ≥50% reduction in the number of headache days and ≥75% reduction in the number of headache days. This distinction is useful in order to understand the added value of each predictor with respect to a negative, a regular or an optimal outcome.
The first finding that emerges from the study is that the variables considered, whether clinical, therapeutic or psychological, were differently associated with the various outcomes.
Anxious and depressive symptoms
For psychological variables, higher depressive symptomatology and lower QoL were associated in the univariate model with overuse, both in the case of its persistence and of its relapse. Comorbidity, in particular depression, is indeed generally known to play a role in perpetuating medication overuse (32) and other studies have shown its role in predicting relapse after detoxification (16–21). Interestingly, the ROC curves showed two different cut-offs for the HADS depression subscale according to these outcomes, with a higher threshold (11 vs. 8) for relapsers than overusers. It is noteworthy that a score >8 on the HADS depression subscale is usually considered the optimal threshold for possible mood disorders, while a score >11 suggests the probable presence of mood disorders (33). Taken together, these findings suggest that relapsers are characterized by a more “probable” depressive symptomatology, and likely by a more complicated (34) psychological pattern. As recently highlighted (21), frequent relapsers are indeed those patients with worse clinical and psychosocial situations.
We did not find any association between anxiety and the considered outcomes. In general, patients with both positive and negative outcomes were equally characterized by a sufficiently marked anxious symptomatology. Hence, it could be that the presence of anxious features represents a risk factor for the evolution of headache – and more specifically of migraine, since the large majority of our population suffered from migraine as primary headache – into MOH (5) than for its prognosis after detoxification.
Migraine-related disability
Furthermore, in line with some studies (12,16–17,21–22), though at variance with another (20), headache disability, as assessed via the MIDAS, was not strongly associated with any considered outcome. This finding may be a consequence of the high MIDAS scores reported in our population before detoxification, but it is nonetheless interesting because the lack of differences between those having a positive or a negative outcome of treatment suggests that even particularly compromised patients may benefit from withdrawal.
Clinical variables
Clinical variables were involved, in different ways, in most of the outcomes. The type of primary headache and its complexity is undoubtedly associated with treatment outcome. Migraine was indeed associated with the outcome ‘responder’; that is, an episodic pattern of headache. Another clinical factor that emerged from the statistical analysis, as associated in the multivariate models with the outcome of ceasing overuse or relapse into overuse, was duration of chronicity. According to ROC analyses, the cut-off for chronic headache duration is 7.5 years. All together, these findings suggest the importance of treating these patients as early as possible in order to overcome medication overuse more easily. They also recommend additional attention when treating subjects with medication overuse who suffer from other types of primary headache in addition to migraine.
Treatments
For a prophylaxis regimen, the intake of preventive drugs was associated by itself with the reduction of headache attacks, highlighting to clinicians the importance of prescribing therapies at discharge in order to control headache (35–38) and therefore improve patients’ daily life activities (39). When looking at the specific classes of prophylactic drugs, some interesting peculiarities should be noted. Flunarizine prescription was associated with the ‘responder’ outcome, also with optimal responders. This datum per se does not imply stronger effectiveness of the drug, as it may simply reflect the fact that depression is one of flunarizine’s side effects (40) and therefore physicians may have preferentially prescribed it to subjects with lower levels/absent depression; that is, those who are more likely to have a positive outcome. On the other hand, antidepressant prescription was instead associated with a negative outcome: Persistence of overuse or its relapse. This finding probably reflects the correct clinical attitude of prescribing this class of drugs to patients who were already more “psychologically” complex and in need of such a specific treatment. That is in agreement with data obtained from a different cohort of MOH subjects in whom we demonstrated that responders feature specific personality profiles compared to overusers and relapsers (41), so as to suggest that psychological factors influence the outcome of disease. However, it must be noted that not all patients received a preventive treatment at discharge. Hence, future studies are needed in order to further explore this aspect, by evaluating differences in detoxification effectiveness among patients receiving or not receiving preventive therapies.
Strengths and limitations
The strength of this study resides in the very large population of MOH subjects, all of whom were very well characterized in terms of clinical data recording and outcome. The population is also quite homogeneous since the patients were enrolled in headache centers, they did not suffer from severe psychiatric disorders, and were naive to detoxification procedures.
Some limitations need to be mentioned: The use of the HADS for assessing anxious and depressive symptomatology does not represent the diagnostic gold standard. We are aware that this self-report questionnaire is a screening instrument; however, its adoption seemed the best option to obtain consistent and comparable data from such a large and geographically spread population. Furthermore, our population may not be entirely representative of the MOH population since we enrolled subjects seeking help in headache centers, who might therefore express a more severe clinical picture. On the other hand, the exclusion of subjects with severe psychiatric comorbidities and previous detoxifications prevented the evaluation of the full spectrum of psychological predictors. However, it is generally accepted that “selected” clinic patients represent a convenience sample for studying an aspect before confirming such findings in the general population. Future studies are needed to also replicate these findings in a population-based group of MOH patients and in a sample of patients featuring all the possible degrees of psychiatric comorbidity, though in the latter case extreme care will be needed to exclude headache associated with psychiatric disorders.
Conclusions
This study shows that clinical, psychological, and treatment variables have different impacts on different outcome measures in a large clinical sample of MOH patients. Though exploratory in nature, our findings suggest some final considerations. First, it is important to appropriately address the issue of medication overuse in chronic headache as early as possible, in order to favour the optimal outcome. Second, MOH subjects should undergo a thorough psychological assessment, in particular those with a longer duration of chronic headache and high depression scores, because they represent a sub-group of particularly challenging patients. Finally, from a purely methodological point of view, our findings underscore the importance of adopting well defined, clinically meaningful outcomes across studies in order to make them comparable and more useful.
Clinical implications
Higher depression scores at HADS are associated with a negative outcome for detoxification in MOH. A longer duration of the chronic pattern of headache (>7.5 years) is associated with relapse into overuse after detoxification. A complete profiling of patients is important for carefully planning the management and follow-up of MOH subjects.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the COMOESTAS Project – EC contract number 215366 (COMOESTAS) FP7 – Thematic priority ICT and by a grant from the Italian Ministry of Health to the National Neurological Institute C. Mondino, 2013–2015.