
Abstract
Chronic daily headache (CDH) remains a relatively unexplored entity in India. Misconceptions are common, unnecessary investigations often done and inappropriate therapy prescribed. Analgesic overuse is seldom recognized. The present report appears to be the first of its kind from India. CDH has been defined as headaches occurring more than 15 days per month for more than 3 months (secondary causes excluded). Over 2 years (1998-1999) 849 cases (49.6% of all primary headaches) were seen. More than 1 year's follow-up data were available in 205 subjects (M 34; F 171). The distribution of these was as follows: (i), chronic tension-type headache (CTH), 33 (16.1%); (ii), chronic/transformed migraine (TM), 169 (82.4%); (iii), new persistent CDH, 3 (1.5%). There were 169 cases of TM (M:F 1:4.7; age 26-58 years). History of past episodic migraine was present in all. Transformation had been gradual (89.4%) or acute (10.6%). Possible factors in transformation included psychological stress (44.4%), analgesic overuse (28.4%), ergot overuse (4.1%). HRT seemed to be implicated in three female subjects. Analgesic overuse was limited between intake of 600 and 2400 mg of aspirin equivalent per day (mean 735 mg). Ergot overuse varied between 1 and 3 mg/day of ergotamine for ≥ 3 days/week. With medical therapy approximately 70% TM and 40% CTH patients noted significant improvement. About 80% of these relapsed on therapy withdrawal. CDH in India is not uncommon. Analgesic/ergot overuse needs to be recognized early. The average dose of analgesic implicated in CDH seems much less compared with that reported in the West.
Introduction
Headaches occurring daily or on a near daily basis are common in clinical practice. Although not included in the International Headache Society Classification (1988), the concept of chronic daily headaches (CDH) is now widely accepted. CDH forms a major bulk of all primary headaches in both population-based as well as clinic-based studies from different parts of the world (1–6). CDH remains a relatively unexplored entity in India. Misconceptions are common, unnecessary investigations often done and inappropriate therapy prescribed. Analgesic overuse is seldom recognized. The present report appears to be the first of its kind from India dealing with the clinical aspects of CDH in this country in a hospital-based study.
Materials and methods
CDH has been defined as headaches occurring for more than 15 days per month (duration> 4 h/day) for more than 3 months (secondary causes excluded). Over 2 years (1998–1999) 849 cases (49.6% of all primary headaches) were seen in a general neurology out-patient clinic (chronic cluster headaches excluded). More than 1 year's follow-up data were available in 205 subjects (male 34, female 171). An analysis of these cases is presented.
All patients had full neurological examination, routine haematological studies, chest skiagraphy and brain imaging studies done to exclude secondary intracranial or extracranial pathologies. Assessments by ophthalmologists and otorhinolaryngologists were made when indicated. Psychiatric co-morbidity was assessed using the DSMIV criteria. In a few selected patients CSF study with manometry was done to exclude chronic meningitis and unusual cases of idiopathic intracranial hypertension without papilloedema. Diagnosis of type of headache had been made using the International Headache Society (IHS) (1988) criteria (7), although the time frame for chronic headache had been modified (from 6 months to 3 months). This is discussed below.
Identification of stressors, psychiatric diagnosis and transformation factors were all based on detailed structured interview of patients, assessing especially the temporal course of the events when headache became daily.
A modified (from IHS recommendation (7) and Solomon (8)) definition of analgesic overuse had been used in view of our past experience (to be discussed). Analgesic overuse was considered when daily intake was ≥ 600 mg of aspirin or equivalent for ≥ 5 days/week or where daily intake of ergotamine was ≥ 1 mg for> 3 days per week.
Diagnosis and classification of the CDH cases were made in a modified form as proposed by Silberstein et al. (9). The terms chronic migraine (CM) and transformed migraine (TM) as proposed by Mathew (10) have been used interchangeably. Chronic post head trauma and cervicogenic headaches (as included in Mathew's (10) classification of CDH) were excluded, as strictly speaking these do not merit classification as primary headaches. Furthermore, a few cases presenting with features of chronic tension-type headaches but having past history suggestive of episodic migrainous headaches were classified as chronic migraine (CM/TM) as recommended by Silberstein et al. (9).
Headache severity was assessed using a five-point scale. Therapy results were assessed using the same five-point scale and by perusal of headache diaries. Formal psychiatric referral was not made for any patient in the series.
Observations
Of the 205 cases studied, there were 34 males and 171 females. The subtype distribution of the cases is shown in Table 1. Transformed migraine (TM) constituted the largest group (82.4%). There was no case of hemicrania continua in the present series.
Chronic daily headache (CDH) (total patients screened 849, patients followed up 205)

The significant number of patients lost to follow-up at 1 year in the present study needs comment. This had not been unusual with chronic headache patients in India as experienced by the author in his 15 years of practice. Several factors may be contributory. Some people probably accept their headache as part of their life and not a serious malady (after investigations have been negative), some almost certainly change doctor/clinic for the sake of getting better treatment, and many have recourse to alternative forms of therapy which are cheaper and easily available.
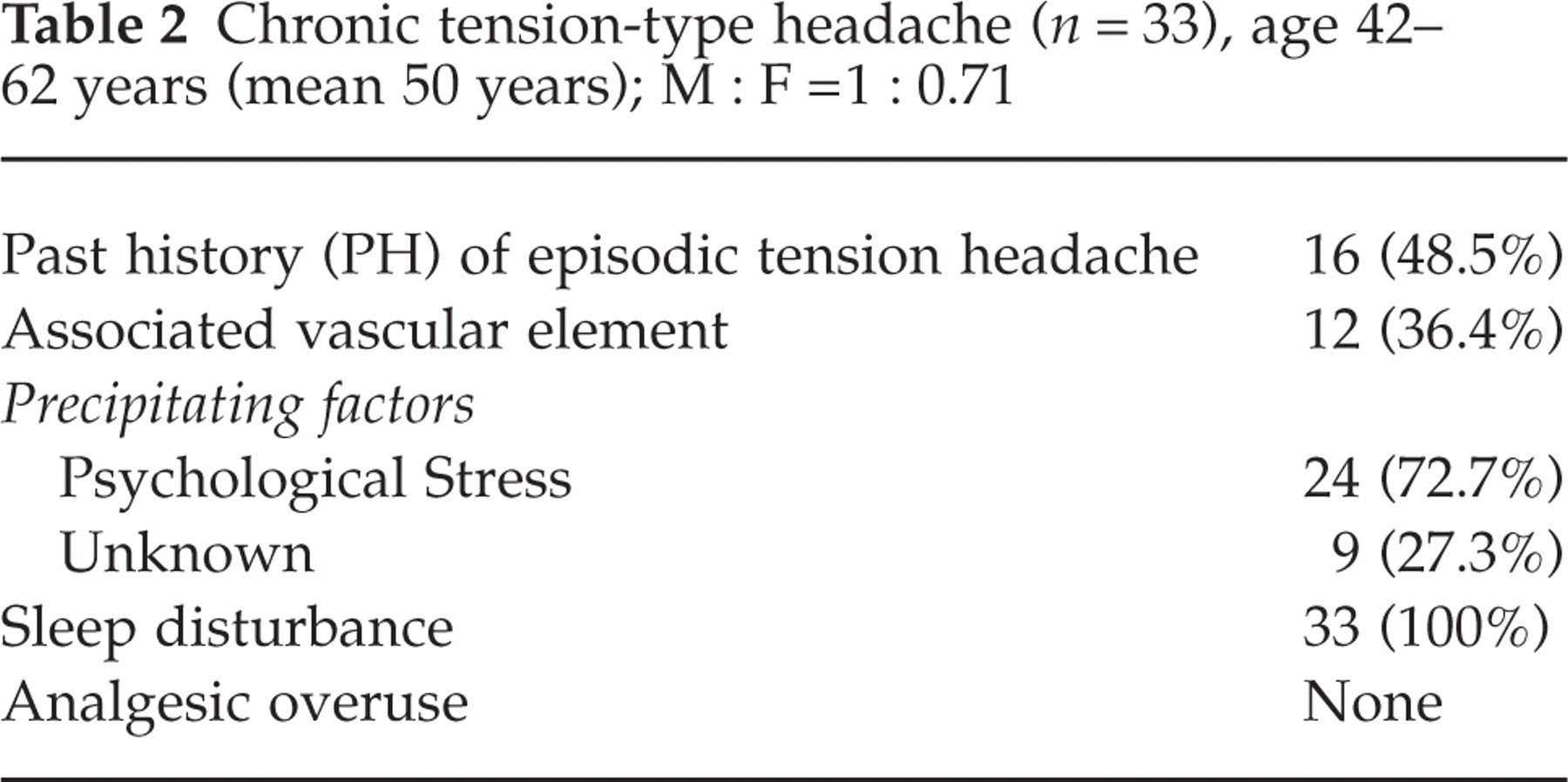
The profile of the chronic tension-type headache (CTH) patients is shown in Table 2. These constituted 16.1% of the subjects with male : female ratio of 1 : 0.71 and a mean age of 50 years. About half (48.5%) had past history of episodic tension-type headache. In this group, such episodic headaches gradually increased in frequency over time, culminating in a daily or near daily almost continuous head pain. In the rest, continuous dull headache started gradually and increased in severity over time. Differentiation of the latter group from new persistent daily headache (NPDH, see below) had been difficult. NPDH was not considered here as the duration of the headache had been longer, and while NPDH patients could almost pinpoint the day of starting of headache, these subjects could not do so. All patients were suffering from daily or near daily, almost continuous dull pressing holocranial pain unaltered by physical activity. Such pain had been present for 4–22 months at presentation. However, about one-third (36.4%) experienced occasional throbbing pain, sometimes with nausea. Such throbbing pain spells did not occur very frequently, and not on a daily basis. In the majority (72.7%), the precipitating factor for daily headache had been psychological stress. Mostly this related to financial inadequacy and stress at work place in men. In no patient in this group could analgesic overuse be implicated. Varying degrees of sleep disturbance were present in all.
Chronic tension-type headache (n = 33), age 42–62 years (mean 50 years); M : F = 1 : 0.71
The clinical profile of patients diagnosed to have CM/TM is summarized in Table 3. TM constituted the largest number (169) of CDH cases encountered. The diagnosis of CM/TM had been made based on recommendations of Silberstein (9) and Mathew (10). The age range varied from 26 to 58 years (mean 39 years) and women vastly outnumbered men (M : F = 1 : 4.7). History of episodic migraine without aura (IHS 1988) was present in all for varying periods (3 to> 20 years). CDH was present for 3–9 months at presentation.
Transformed migraine (n = 169), age 26–58 years (mean 39 years); M : F 1 : 4.7
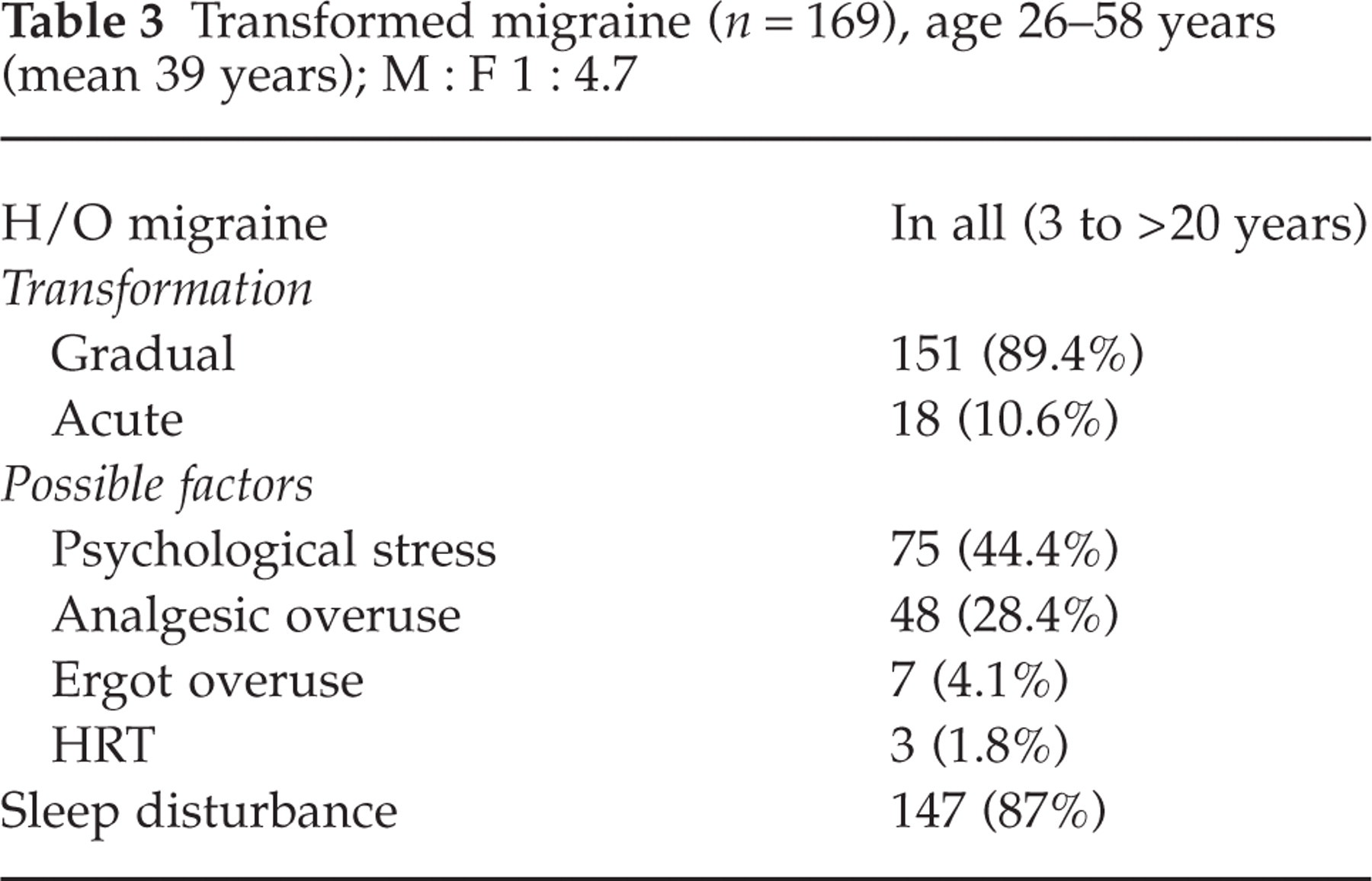
In 89.4% of cases the transformation from episodic to daily headache had been gradual (weeks to months), whereas in a small minority (10.6%) this had been rather acute (over days). The commonest precipitating factor had been psychological stress. In the acute transformation group this included family bereavement, separation, and loss of jobs. In the gradually transformed cases, financial instability, household disharmony, anxieties relating to children and stress at work place were evident. Analgesic overuse was noted in about one-third (28.4%) and ergot overuse in 4.1%. The analgesics implicated were always over-the-counter medicines containing various combinations of aspirin and paracetamol. Ergot use had always been on medical prescription and surprisingly in excessive dosage or on a near-daily basis (as advised by the physicians). However, analgesic or ergot overuse had seldom been the sole factor for transformation. Most patients with drug overuse had significant psychological stress accounting for the initial increased frequency of their migraine. This prompted excess use of analgesics, culminating in a daily or near-daily headache. In three women, in their late forties, daily headache started 8–10 weeks after being put on hormone replacement therapy (HRT) at menopause. In nearly half of subjects (81/169), no clear precipitating factor for transformation could be found.
All patients complained of a near-daily headache of dull type with more than one spell of throbbing headache superimposing in a day. The exacerbations were very often accompanied by nausea and at times vomiting. None ever had any visual or other focal neurological symptoms. Factors implicated in exacerbations included: exposure to sun, fasting, physical activity, increased psychological stress, menstruation, being in a crowded place, noise, and lack of sleep. More than one factor seemed to be implicated in all cases. Varying degrees of sleep disturbance were present in almost 87% of subjects. However, it was unusual for subjects to be woken up from sleep by severe headache (about 10%).
Analgesic overuse could be documented only in TM patients in the present series out of all CDH cases. The intake varied from 600 to 2400 mg/day of aspirin equivalent with a mean of 735 mg/day. The ergot overuse found in 4.1% of TM subjects varied from 1 to 3 mg/day, more than 3 days/week.
Only three patients in the present series were diagnosed to have new persistent chronic daily headache (NPCDH). None of them ever had any significant headaches in the past and presented with near daily headache spells for 3–4 months at presentation without any obvious precipitating cause (e.g. psychological stress, trauma, etc.). All three patients could specify the time of onset of the headache phase but could not relate it to any specified event. Detailed neurological evaluation (including radiology and CSF studies) failed to elicit any secondary pathology. The headaches were of vascular (throbbing) nature for the most part, but a background dull headache remained throughout. Analgesic overuse was not documented. All mentioned feeling anxious but not depressed, but denied that psychological factors were a cause of their symptoms. Sleep disturbances were not noted in any of the three subjects.
Psychiatric co-morbidity
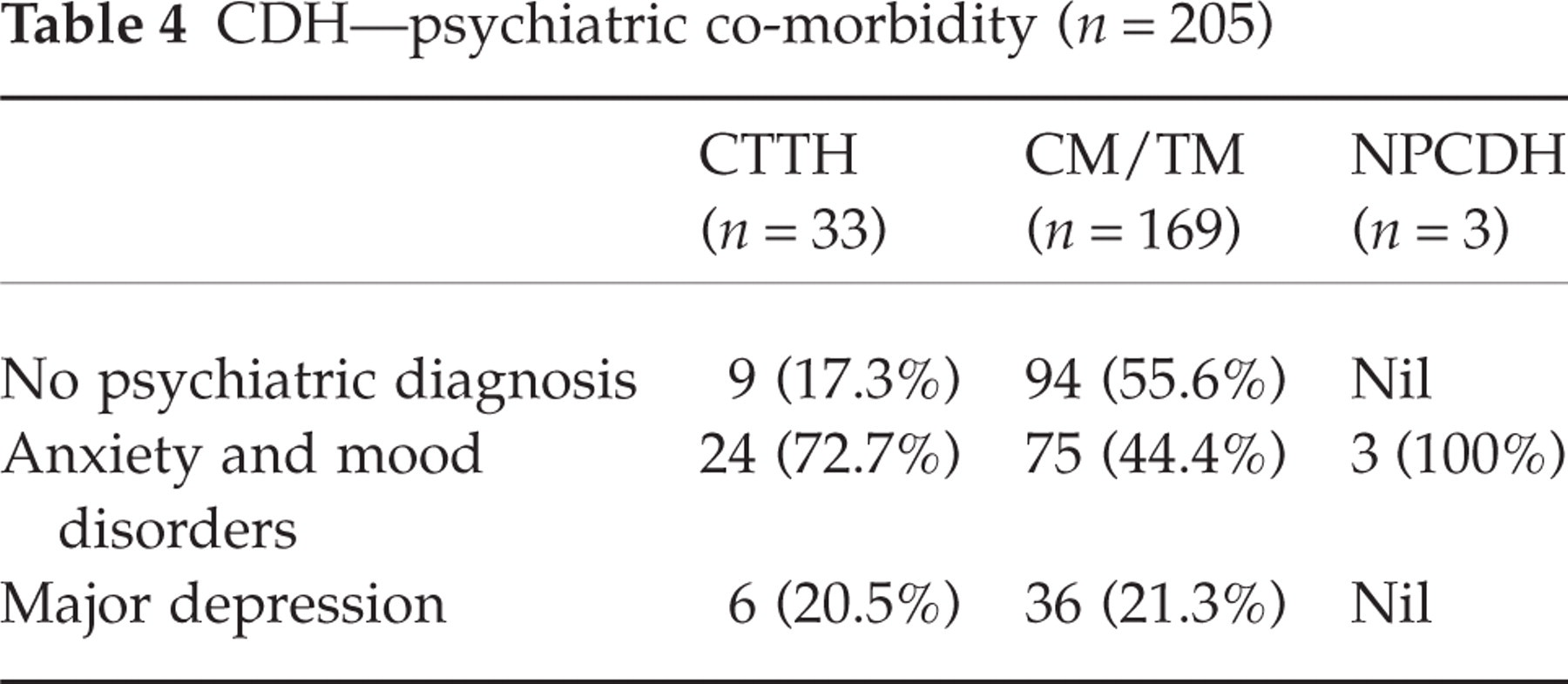
DSMIV criteria (11) were used to diagnose psychiatric conditions in 205 subjects in the present series. One hundred and three cases (nearly 50%) had no psychiatric diagnosis. Most of these subjects suffered from transformed migraine. One hundred and two patients had anxiety and mood disorders, and 42 (20.5%) suffered from major depression. Somatoform disorders were not present in any subject. The results are summarized in Table 4.
CDH—psychiatric co-morbidity (n = 205)
Results
All patients in this series were followed up for more than 1 year (range 14–19 months). CM/TM patients were treated with amitryptiline (50–75 mg daily) combined with one of the migraine prophylactic agents like propranolol, flunerazine, pizotifen or sodium valproate. In the three women with HRT-induced transformation, the HRT was withdrawn and only flunerazine was continued. In patients with analgesic or ergot overuse, these were withdrawn abruptly. They were also put on amitryptiline and a migraine prophylactic agent. None developed any very significant rebound headache needing either parenteral therapy or hospitalization. The CTH patients were put on a combination of chlordiazepoxide (30 mg daily mostly) along with amitryptiline (50–75 mg daily). Formal psychiatric help was not sought in any patient during the period of study.
At 3 months, 116 patients with TM (68.6%) and 14 patients with CTH (42.4%) noted more than 50% reduction in severity of headache on a five-point scale. Therapy was continued for 4–6 months. When reviewed after 3 months of therapy withdrawal, most of the patients (175/205) had increased headache by at least one point. The vast majority of the subjects studied (except 18 patients) needed some form of medical treatment to keep their headaches under control. However, all patients continued to lead a normal working life at home or outside. Surprisingly, none of the subjects with analgesic overuse went back to them, at least during the period of regular follow-up.
Discussion
It is apparent from the present study that CDH is common in Indian patients attending a general neurology clinic. Slightly less than half of all primary headache subjects had CDH. It appears the incidence could be higher in dedicated headache clinics. Unfortunately, such cases are often misdiagnosed as having only migraine, anxiety disorders, depression and even having ocular or sinus diseases. Re-orientation of physicians regarding the recognition of this common malady is essential.
There has been no consensus on the definition of CDH, especially in relation to the ‘cut-off’ time needed for the diagnosis. The IHS (1988) (7) recommended a minimum duration of 6 months for diagnosis of chronic tension-type headache, but only 2 months for the diagnosis of chronic post-traumatic headache. Some authors have considered a period of continuing headache for at least 1 year to merit diagnosis of CDH (12). The time frame appears arbitrary. Previous and ongoing experience of the present author suggest no significant difference between the clinical profile of the patients who presented at> 3 months’ or> 6 months’ history of daily or near-daily headache. This fact combined with the high clinic default rate of Indian patients with chronic headache (only 205 of 849 patients could be followed for more than 1 year) prompted the author to consider the ‘cut-off’ point at 3 months for diagnosis of CDH for the purpose of the present study. In a given population, with high clinic default rate, this ‘cut-off’ point seems justified, especially when there is no consensus on such an issue, particularly in relation to chronic migraine. It may be of interest that the clinical profile remains much the same when patients with chronic headache present with less than 3 months’ history of daily or near-daily headaches. Such cases, of course, are not included in the present study but the observation needs consideration in formulating a consensus definition of CDH in the future.
Overall, the clinical profile of all classes of CDH patients studied does not differ very significantly from previous reports, especially from western countries (1–3). Chronic/transformed migraine remains the most commonly encountered form, with increased prevalence among women. Factors contributing to transformation have been similar to those observed in previous studies (10). However, in nearly half of subjects no clear precipitating factor could be found. This figure is higher than what had been noted earlier (22% reported by Manzoni et al. (13)). Of interest was the transformation induced by being on HRT in three women, all of whom improved after discontinuation of the drug. The relative paucity of CTH cases in the present series compared with CM/TM cases probably represents a true lower incidence of the former in our population with CDH, as this difference was observed even in the entire sample of patients screened (n = 849; CTH 139, CM/TM 699) and not just in the sample followed up (n = 205). The difference thus appears unlikely to be related to any greater percentage of patients with CTTH who were not followed up.
Analgesic overuse in the Indian context needs special mention. This problem is very seldom recognized by physicians and their patients in this country. It is not unusual to come across regular prescription of an analgesic or even ergotamine in a BID or TID dosage for a migraine sufferer being continued for weeks at a time. In the present series, analgesic overuse was recognized as a transformation factor in over 25%, about 20% of cases of TM, and ergot in about 4%. These figures are undoubtedly less than those quoted from the west (14, 15), but no doubt they are significant. Interestingly, no case of analgesic overuse was encountered in the chronic tension-type headache group. nor in any patient with NPCDH. The mean dose of analgesic used appeared much less (735 mg/day) compared with a recent finding in a study from Boston (1860 mg/day) (16). This observation had been made by the author much earlier, and hence in the conduct of the present study the recommended definition of analgesic overuse has been altered to highlight the Indian scenario. None of the subjects developed any serious rebound headache when these were abruptly withdrawn. This would obviously raise the question about the true role of these agents in the genesis of CDH in Indian patients in the present study. However, the data from this study and past experience of the author that analgesic withdrawal almost invariably helps to reduce the intensity of the headache, would indicate a definite causal role of analgesic overuse in the genesis of CDH in Indian subjects. However, the findings may suggest a racial/genetic difference in opioid pathway response to analgesic consumption.
The psychiatric co-morbidity studied in the series revealed nearly similar results to those reported by Verri et al. (17). Some emphasis has been placed in this study on the role of psychological stress in transformation from episodic headache to chronic headache. This observation, however, does not undermine the reports of structural (biochemical) brain changes in chronic headache subjects and does not indicate that CDH is a purely psychogenic disorder. Alteration in neurotransmitter function (qualitative and quantitative) induced by psychological stress with alteration in central sensitization may appear to be an attractive, but unproved, hypothesis.
A careful perusal of the clinical profile of the various subtypes of CDH discussed in the study would reveal overlapping of vascular and non-vascular components of headache in varying proportions in several subjects. The IHS classification (1988) (7) clearly defines individual headache types, but appears inadequate when different headache types overlap to constitute a ‘syndrome’ like CDH. This aspect needs careful consideration in formulating future classification systems.
The differentiation of the various subtypes of CDH proposed and commented upon in the present study also appears to some extent to be arbitrary. Transformed migraine remains a distinct entity with diagnosis of preceding episodic migraine attacks as defined in the IHS classification. However, the distinction between chronic tension-type headache patients with superimposed intermittent throbbing quality of headache and those labelled with migraine/CTH complex evolved from episodic tension-type headache (described by Mathew (10)) may not always be very clear. In practice, the distinction really boils down to one of only intensity and frequency of the vascular component of the headache.
Follow-up data in the present series was limited principally because of high clinic default rate. This is probably related to the inherent tendency of Indian subjects with chronic headaches to change doctors and hospitals frequently (especially when they are in a large metropolis like Calcutta), and the easy and cheaper availability of alternative forms of therapy. However, the limited data point to the intractability of CDH to medical therapy, and this concurs with the observations of other workers (18, 19). It appears that with onset of CDH, the pain-perceiving neurotransmitter pathways and circuits are so much altered that it becomes difficult to reset them to the pre-CDH state.