
Abstract
Background
Persistent headache/facial/neck pain attributed to past cervicocephalic arterial dissection is under-documented in literature. Our main goal was to evaluate clinical characteristics and contributors to this persistence.
Methods
A retrospective cohort study which included patients with a radiologically confirmed cervicocephalic arterial dissection (2015–2020) in a Portuguese tertiary hospital. Headache persistence was identified through clinical records. A questionnaire aimed to characterize headache in three moments: previous, persistent, and headache at the time of the interview (on average 2.5 years post-event).
Results
Ninety-two patients were identified; 24 (26.1%) had headache persistence ≥3 months, and 20 (22.2%) on average after 2.5 years post-event. There were no differences regarding demographics and vascular risk factors among patients with (n = 22) and without (n = 68) headache persistence. The first group had higher previous headache history (68.2% vs 4.4%, p < 0.001), delay in diagnosis (3.6 vs 1.9 days, p < 0.001), and headache/cervicalgia as the first symptom (81.8% vs 41.2%, p < 0.001). At the time of the interview, 20% still reported daily headache. A logistic regression model depicted headache history (OR = 59.8, p < 0.001), acute headache/cervicalgia (odds ratio, OR = 25.4, p = 0.005), posterior circulation dissection (OR = 7.6, p < 0.001), and less than 4 points by National Institutes of Health Stroke Scale score (OR = 5.0, p = 0.025) as contributors to headache persistence.
Conclusion
Headache persistence post-cervicocephalic arterial dissection is common, and frequently affects patients daily. As it potentially affects functional outcomes and quality of life, the contributors identified in this study may help clinicians manage patients after the acute event.
Introduction
Cervicocephalic artery dissection (CCAD) encompasses a tear in the intimal layer of a cervical or cephalic artery, resulting in the formation of a “double lumen” (1). Blood fills the recently created false lumen forming an intramural hematoma (1). CCAD is considered a frequent cause of ischemic stroke in young and middle-aged adults (2,3), representing up to 25% of all ischemic infarcts in individuals under 45 years (4). In European population-based studies, the incidence of CCAD is estimated at 2.6–3/100,000/year and appears to decrease with age (3). Nevertheless, little-to-no scientific evidence is available concerning the ideal therapeutic strategy, its duration, and overall prognosis (5).
Headache is the most frequent inaugural symptom of CCAD, present in up to 86% of patients (6). Headache or facial or neck pain attributed to cervical carotid or vertebral arterial dissection has been described in part II (6.5.1) of the International Classification of Headache Disorders – 3rd edition (ICHD-III) (7). It can be classified as acute (resolving within one to three months) or persistent pain (persisting for more than three months after the dissection has stabilized) (7). There are some specific acute headache-related features, such as the acute onset, the continuous duration, and its persistence over time, that seem to be more prevalent in headaches attributed to vascular disorders, as is the case with CCAD (7).
Although headache persistence after CCAD (HPCCAD) has been vastly under-documented as a long-term consequence of this event, it can be a major contributor to a decline in the overall quality of life (6,8–10). In the literature, about a quarter of patients with CCAD had a persistent headache at six months post-event (8); another study reported 19% of HPCCAD at 36 months post-event (9). Very few studies have investigated its characteristics and possible risk factors that contribute to this persistency in the post-CCAD context. Some authors pointed out that a previous history of migraine, as well as anxiety or depression, could be possible contributors (7). Consequently, we aim to evaluate clinical characteristics and identify possible contributors to HPCCAD.
Methods
Design and participants
A retrospective cohort study was performed, identifying 92 adult patients with imaging features and clinical characteristics of CCAD, diagnosed from January 2015 to June 2020, selected from the carotid and transcranial Doppler ultrasonography database from Centro Hospitalar Universitário de São João, a tertiary referral hospital in Portugal (Figure 1). The dissection was confirmed radiologically by the presence of an intramural hematoma, dissecting aneurysm, long tapering stenosis, intimal flap, double lumen, or an occlusion more than two centimeters above the carotid bifurcation with a dissecting aneurysm and/or long tapering stenosis after recanalization, as in accordance with the recent European Stroke Organization 2021 guidelines (11). All cases with a dubious diagnosis, or which had not been confirmed by Computed Tomography Angiography (CTA) and/or Magnetic Resonance Angiography (MRA) were excluded (seven of 99 patients, Figure 1). Electronic files were reviewed independently by two study investigators, identifying patients who, according to medical records, met the diagnostic ICHD-3 criteria for persistent headache attributed to CCAD (n = 24), including initially fulfilling the requirements for acute headache or facial or neck pain attributed to cervical carotid or vertebral artery dissection (7). If patients had a pre-existing headache but the headache at dissection onset had changed in characteristics (frequency, intensity, and/or localization), we considered it attributable to the event.

Flow chart showing patient selection.
Variables analyzed
Twenty-two of 24 patients accepted and were able to answer a structured telephone questionnaire, performed in a single moment, consisting of 20 systematized questions, mostly multiple-choice, aimed at characterizing previous, acute, and persistent pain post-event. This survey was based on the questionnaire of Matsumoto et al. (12), which accessed the characteristics of the patient’s pain in three distinct moments: 1) previous and acute (at the time of dissection), 2) persistent headache, and 3) at the moment of the intervention (on average after 2.5 years post-event). It included the following characteristics of the event and headache at the time of dissection: the presence of a previous history of headache (if present: frequency, and type of headache), history of head or neck trauma before the dissection event (minor or major), presence of headache at the time of dissection (and whether it was the first symptom), and characteristics of acute headache (location, laterality, quality, intensity on the numerical pain scale from 0 to 10, time of onset, duration, aggravating factors, relieving factors, whether it was the worst headache ever, and accompanying symptoms). Patients who had a headache before the CCAD event were asked to indicate if the severity or frequency of their headache had changed after the dissection (more severe, unchanged, or better). For persistent headache and headache at the moment of the interview, we evaluate the following characteristics: frequency, location, laterality, quality, intensity, accompanying symptoms, aggravating and relieving factors, analgesics taken for pain (type, frequency of intake, and response to analgesia – partial, good/satisfactory or no response), and if there is a current outpatient follow-up in a headache clinic/consultation.
Data concerning the patients’ sociodemographic characteristics, pathological history, vascular risk factors, and characteristics of the arterial dissection event, as well as an inpatient and consultation approach, were collected from medical records through the hospital electronic process.
Statistical analysis
Data were analyzed with IBM Statistical Package for the Social Sciences (SPSS) version 25. The baseline and clinical characteristics of HPCCAD and no-HPCCAD were compared using the chi-square test or the Fisher exact test for categorical variables, and the t-test (parametric test) or the Mann-Whitney U test (non-parametric) for continuous variables. To compare the characteristics of acute and persistent headache in the same group, we used the paired t-test. Quantitative variables were reported as mean ± SD or median (interquartile range, IQR). Normality was assessed by using skewness and kurtosis measures. Bonferroni correction was applied when necessary. All p-values were 2-tailed, with a p-value <0.05 indicating statistical significance. Multivariate logistic regression analysis was performed to identify independent factors. In this regression, the variables included were based on univariate associations (p < 0.05) and theoretic assumptions, considering the variables: initial National Institutes of Health Stroke Scale (NIHSS), Glasgow coma scale on admission, age at the event, involved circulation, headache/neck pain on admission, the maximum level of care, and headache history. Odds ratio (OR) was used to estimate associated factors.
Results
We identified 92 patients with radiological confirmed CCAD: 24 (26.1%) had persistent headache according to medical records for at least three months (Figure 1). Twenty-two of them (91.7% response rate) accepted to answer a telephonic questionnaire.
In the CCAD cohort, the patient median age at diagnosis was 48 ± 13.7 years, and 58 (64.4%) were male. Particularly, in the HPCCAD group, the median age at the event was 43 ± 1.8 years, and half of the sample was comprised of women. We found no differences concerning gender or age between HPCCAD and no-HPCCAD patients (p = 0.103 and p = 0.592, respectively) (Table 1).
Sociodemographic characteristics of patients with cervicocephalic arterial dissection.

BMI, Body mass index; HPCCAD, headache persistence after cervicocephalic arterial dissection; IQR, Interquartil range; SD, standard deviation.
Bold entries in p-value indicate statistical significance (p < 0.05).
Regarding baseline characteristics, and comparing HPCCAD and no-HPCCAD patients, HPCCAD were more prone to have a previous history of headache (63.6% vs 4.4%, p < 0.001), with a migraine without aura being the most prevalent type of headache in both groups. In the HPCCAD group, three out of 22 patients had a history of chronic headache before the dissection (13.6% vs 0%, respectively). There were no differences between groups regarding other baseline characteristics, namely vascular risk factors, such as hypertension, dyslipidemia, and diabetes. Most HPCCAD patients (54.5%) did not smoke and had never smoked; in this group, 10 (45.5%) had a history of trauma, which showed no statistical difference compared to no-HPCCAD patients (36.8%) (Table 1).
During the acute dissection event, headache/neck pain was the most frequently experienced first symptom (51.5%), particularly prevalent in patients that went on to develop HPCCAD (81.8% vs 41.2% in no-HPCCAD, p = 0.002, Table 2). Fifty-nine patients (65.6%) had symptoms and imaging findings consistent with ischemic stroke at admission, with a median of 3 (IQR 0–11) on the initial NIHSS scale. Although there is a tendency for patients in the HPCCAD group to have a lower NIHSS (1 [0–17] vs 4 [0–24] in the no-HPCCAD group, Table 2), the difference was not statistically significant (p = 0.150). Forty-seven patients in total (52.2%) came to the emergency department on the day of pain onset, whereas 20 (22.2%) came one week or more later. Most were admitted to the stroke unit (57.8%), both in the HPCCAD (45.5%) and no-HPCCAD (61.8%) groups; only two patients (9.1%) were admitted to the intensive care unit in the HPCCAD, and eight (11.8%) in the opposite group. HPCCAD patients had a significant symptom-onset-to-diagnosis delay compared to no-HPCCAD patients (3.6 ± 1.8 days vs 1.9 ± 1.5; p < 0.001) (Table 2).
Clinical and instrumental characteristics of cervicocephalic arterial dissections.
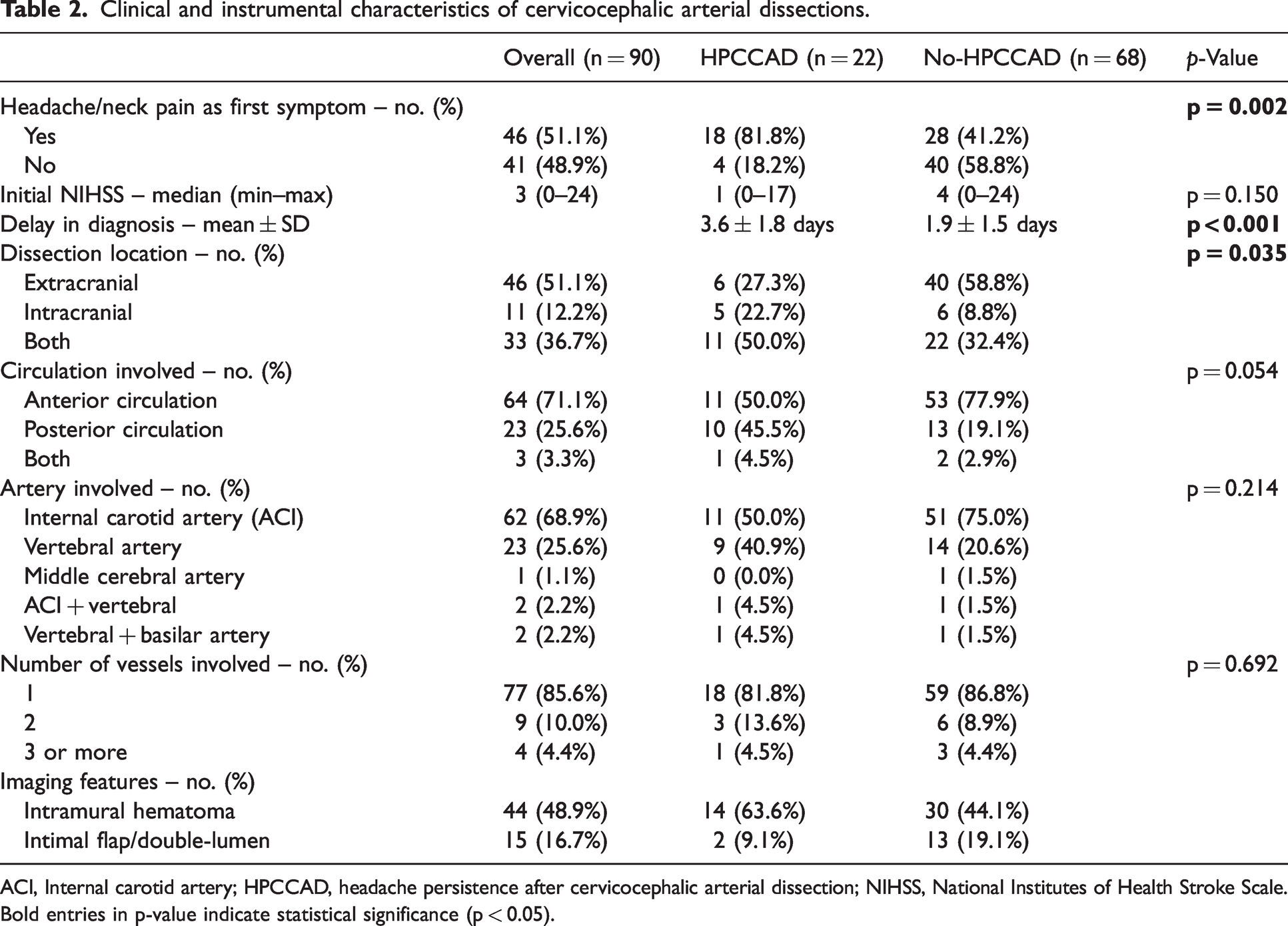
ACI, Internal carotid artery; HPCCAD, headache persistence after cervicocephalic arterial dissection; NIHSS, National Institutes of Health Stroke Scale.
Bold entries in p-value indicate statistical significance (p < 0.05).
CTA was the most frequently performed exam for suspected arterial dissection (n = 55; 61.1%), followed by MRA as means for confirmation (n = 43; 47.8% of cases); Doppler ultrasound was the most used exam for patient follow-up (n = 35; 38.9%). In general, arterial dissection was most frequently extracranial (51.1% in total), affecting predominantly the anterior circulation (71.1%) (Table 2). Intracranial dissections were significantly more common in HPCCAD patients (22.7% vs 8.8% in no-HPCCAD, p = 0.035), and these patients tend to have commonly affected the posterior circulation (45.5% vs 19.1%, p = 0.054). Internal carotid artery involvement was present in 50.0% and 75.0% of patients reporting HPCCAD and no-HPCCAD, and the vertebral artery was affected in 40.9% and 20.6% of patients, respectively. In both groups, the bulk of patients had a single vessel dissection event; the involvement of multiple dissected vessels was seen in a minority of patients (4.5% in the HPCCAD group and 4.4% in no-HPCCAD). Of patients with persistent headache, 14 (63.6%) had an identifiable intramural hematoma (vs 44.1% in the no-HPCCAD); intimal flap/double-lumen of the dissected artery was reported in a minority of cases in both groups (9.1% in HPCCAD and 19.1% in no-HPCCAD) (Table 2).
Of the 22 patients with HPCCAD, 20 (90.1%) reported headache/cervical pain during the dissection event, mostly ipsilateral (70.0%) (Table 3). Nuchal/cervical features were described in nine (45.0%), bifrontal headaches in four (20.0%), and diffuse headache in two (10.0%). Infrequent locations included facial (n = 2, 10.0%) and temporal pain (n = 2, 10.0%). Pain description was predominantly fading/stabbing (n = 6, 30.0%), throbbing (n = 4, 20.0%) or as tightness/pressure (n = 4, 20.0%); nine patients (45.0%) characterized their headache as sudden. Concerning pain intensity, 10 patients (50.0%) characterized it as severe and five (25.0%) as moderate; one patient reported a thunderclap headache. More than half (55.0%) described it as being the worst headache they had ever felt. Most patients (n = 18, 90.0%) had accompanying neurological symptoms at the onset of dissection, such as dysarthria, paresis, and hypoesthesia (n = 7, 35.0%), isolated paresis and/or hypoesthesia (n = 6, 30.0%), autonomic dysfunction (n = 2, 10.0%), nausea and/or vomiting (n = 2, 10.0%) and lower cranial nerve involvement (n = 1, 5.0%) (Table 3).
Characteristics of acute and persistent headache attributed to past cervicocephalic arterial dissection.

Persistent headache was characterized retrospectively by telephonic questionnaires, with a time span of one to five years following the event (Table 3). We contrasted the characteristics of headache at the time of the dissection and the persistent headache reported in clinical records: 15 patients (68.2%) described the persistent pain as similar to the one preceding the event, with no change in the pattern of prior headaches, only with change in frequency. The remaining patients rated the HPCCAD as greater in intensity and longer-lasting (at least 72 hours) than previous ones (Table 3). After an average of 2.5 years after the event, 20 (22.2%) patients reported persistent headache, four of which (20.0%) have daily persistent headaches, and nine (45.0%) referred symptomatology less than once a week (Table 3 and Figure 2). Nuchal/cervical (n = 7; 35.0%) and holocranial (n = 6; 30.0%) were the most prevalent pain locations. Concerning quality, 10 (50.0%) patients had a throbbing sensation, and most (n = 14; 70.0%) classified the events as moderate in severity (4–7 on the numerical pain scale from 0–10). Emotions were reported as an exacerbating factor of headache by half, with six patients (30.0%) not able to identify any aggravating factors. Concerning elements of relief, rest and analgesics seemed to improve the symptoms in most of the patients (n = 11; 55.0%), while lying-down position was sufficient for five (25.0%). Forty-five percent did not report accompanying symptoms; for those who had them, photophobia was the most prevalent (20.0%). About 70% (n = 14) of patients reported taking simple analgesic medication, with eight (57.1%) saying the analgesic response was partial, and six- (42.9%) reporting satisfactory response to medication.

Characteristics of persistent headache attributed to previous dissection.
In the logistic regression model, previous headache history (OR = 59.8, p < 0.001), headache/neck pain on admission (OR = 25.4, p = 0.005), posterior dissection involvement (OR = 7.6, p < 0.001), and less than 4 points by NIHSS score (OR = 5.0, p = 0.025), were identified as contributors to HPCCAD (Table 4).
Multivariate logistic regression analysis.
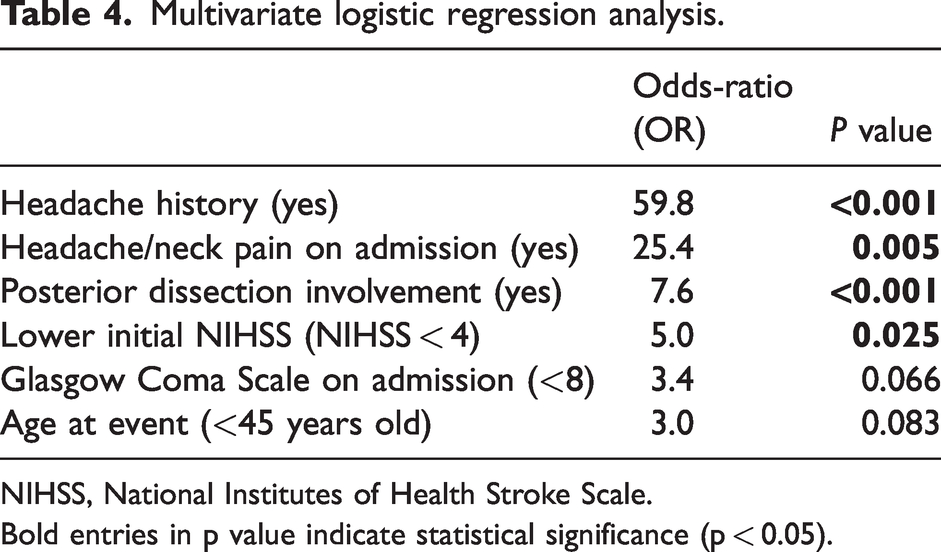
NIHSS, National Institutes of Health Stroke Scale.
Bold entries in p value indicate statistical significance (p < 0.05).
Discussion
Our research provides new and important information about persistent headache or facial/neck pain attributed to past cervicocephalic arterial dissection. In this study, about a quarter of patients with CCAD had persistent headache or facial or neck pain attributed to past cervical carotid or vertebral artery dissection for at least three months after the event. Twenty-two percent reported its persistence 2.5 years later (on average), and of these patients, a fifth had daily headaches. Previous history of headache is the factor that confers the greatest risk for headache persistence, followed by having headache/neck pain as the presenting symptom, a posterior circulation dissection involvement, and a lower initial NIHSS.
Acute headache or facial/neck pain in a CCAD can be a warning sign of subsequent stroke; thus, an early diagnosis has the potential to be lifesaving (5). Most patients with CCAD were between the third and fifth decade of life, and often with no identified vascular risk factors (5,6). Headache/cervical pain was the first manifestation of the dissection in more than half of the cases, especially in our HPCCAD group, in which 82% had a headache as the first symptom, commonly in association with other symptomatology. Onset of headache around the time of the dissection is well described in the literature (5,6). Kim et al. (5) suggested that acute occipital-nuchal severe pain was suggestive of CCAD, which translated into our work, where almost half of the patients presented with nuchal/cervical features during the episode, frequently describing the pain as severe. Indeed, a recent systematic review about headache in CCAD showed that, in most cases, the pain was classified as severe (55%), with an acute/subacute onset, and generally ipsilateral (although it can also present as contralateral or diffuse) (6). Additionally, it was mainly reported as throbbing (35%), followed by constrictive, and prolonged (mean of four days) (6). This headache is reported to be different from any previously experienced pain and often requires analgesics (6); interestingly, in our study, 55% of patients reported it as the worst headache they ever had. Nevertheless, it has no constant specific pattern, which can be quite misleading, mimicking other primary headaches (7).
The HPCCAD is less documented in the literature, and few authors have studied its frequency (8,9); nevertheless, our work is in concordance with the findings of other studies in this field (8,9,13–15). Schytz et al. (8) showed that six months after dissection, five of 19 patients (26.3%) reported persistent headache attributable to the event. At 36 months of follow-up, Leys et al. (9) found out that 21 of 110 patients (19.1%) with stroke after artery dissection had a residual headache or cervical pain. Also, Hansen et al., in a prospective cohort study with 275 patients with stroke of any etiology, showed that at three and six months, 23% and 23.4% of patients had a persistent headache post-stroke, respectively, and at three years 11.7% reported maintenance of this headache (13,14). On the other hand, Lebedeva et al. (15), in a recent prospective study, found lower percentages for acute and persistent headaches after stroke: at three months, 61 of 529 (11.5%) patients had a headache after stroke, and 55 (10.4%) had a persistent headache attributable to ischemic stroke. One possible justification could be the fact that these authors consider that a headache at stroke onset with different characteristics from a pre-existing headache can fit into an attributed-to-stroke headache, whereas if the characteristics are unchanged, they were not attributed to stroke. Therefore, these authors minimize the misclassification bias between pre-existing and new headaches (15). Indeed, our data showed that the majority of patients with HPCCAD have a prior history of headache (63.6% vs 4.4% in the no-HPCCAD group), mostly a migraine without aura. Our logistic regression model also points out that having a history of headache results in a 60-fold increase in having HPCCAD. In the literature, some studies proposed that the history of migraine is a risk factor for spontaneous CCAD (16–22), more evident for migraine without aura (19). Nevertheless, no author to date has studied the influence of migraine history on HPCCAD. Tentschert et al. (17) showed that 23% of patients with a persistent headache for three years after a stroke had previous history of headache, and our study showed a percentage almost three times higher (63.6%). On the contrary, Lebedeva et al. (15) did not find a high prevalence of previous headache among patients with persistent headache after stroke, once more possibly explained by fine distinction between current and previous headaches.
In our study, 31.8% of patients characterized persistent headache as being more intense and prolonged (at least 72 hours) than previous ones. The pathophysiology behind the development of a persistent post-stroke/dissection headache or worsening of pre-existing headache is unknown (16). Central sensitization of nociceptive pathways may contribute to its persistence (15,16); comorbid depression, fatigue, and sleep changes may also exacerbate or perpetuate the previous headache (16,23).
Regarding the characteristics found for HPCCAD in our study, first, these persistent headaches were more frequently throbbing (50.0%) than the acute/at time of dissection headache (20.0%), as reported in other studies (16). These patients seem to display mostly migraine features, but also tension-type headaches, and a fifth of the sample reported daily HPCCAD. The fact that they have characteristics similar to primary headaches, especially in patients with a previous history of headache, may lead to an initial underestimation by patients and clinicians, contributing to the persistence of this symptom (15). Indeed, in our study, HPCCAD patients had a delay in diagnosis, with a symptom-diagnosis time twice as long as the control group, which may also have contributed to a delay in treatment and persistence of headache. Other studies also point out that medication overuse headache is frequent in patients with a persistent headache, which can contribute to the worsening and chronicity of this headache (15). Lebedeva et al. showed that, although almost half of their patients had a migraine-like persistent headache after stroke, triptans were ineffective in these group, which may point to a different pathophysiology for the headache subtypes (15).
Second, HPCCAD patients more often had significant involvement of the intracranial circulation and tended to involve the posterior circulation; both features were almost 2.5 times more than in the no-HPPCAD group. These findings may explain why nuchal and/or neck pain was the most common site of pain in HPCCAD. Other studies reported a higher prevalence of headache in vertebrobasilar dissections, which may be explained either by the local pressure exerted by the blood clot or by the release of pro-inflammatory neurotransmitters from nerve terminals near the injured vessel, which can also contribute in itself to the persistence of headache (6,18).
In addition to the headache history, initial headache/neck pain, and posterior circulation dissection involvement, our logistic regression model also identified a lower initial NIHSS (less than 4) resulting in a five times higher risk of HPCCAD. This finding is in agreement with an other study (15). One of the reasons we highlight is that patients with lower NIHSS, often with a predominance of headache and/or concomitant mild neurological signs/symptoms, may underestimate their symptoms, resulting in an increase in the time to diagnosis, possibly contributing to the persistence of this condition. Other authors considered that a possible explanation could be the fact that the brain regions involved in the neural networks responsible for pain processing are preserved, and/or due to the good arterial elasticity of the cerebral arteries without severe atherosclerosis in patients with less severe events (15).
We did not find any studies in the literature that were dedicated to the study of risk factors for headache persistence after CCAD. Having a CCAD as an etiology of stroke is proposed as being a risk factor for persistent post-stroke headache in the study of Lai et al. (16). These authors also reported female sex, being younger, headache at stroke onset, pre-existing headache disorder, and comorbid fatigue or depression as risk factors for headache persistence post-stroke. Although the difference was not significant, as was the case in the cohort presented by Lai et al., our HPCCAD group showed a higher percentage of women and patients tended to be younger, suggesting that this may be the population most prone to headache persistence.
Finally, this study had the benefit of having access to a large database from the ultrasound exams performed (used both for screening and monitoring), including patients not only hospitalized in the neurology ward but also in other inpatient services and intermediate/intensive care units. With this said, we present some of its limitations. One major limitation is the small sample size, since CCAD does not have a high incidence which makes it difficult to generalize the results. Indeed, in our study, we considered patients who met the ICHD-3 criteria for “acute headache or facial or neck pain attributed to cervical carotid or vertebral artery dissection” and, later, according to medical records, those who met the ICHD-3 criteria for “persistent headache or facial or neck pain attributed to cervical carotid or vertebral artery dissection”. It is true that 15 patients (68.2%) described the persistent pain as similar to the one preceding the event, with no change in the pattern of prior headaches; however, the characteristics of the headache and its relationship with the dissection event (close temporal relation to other local signs of the cervical artery dissection, intensity, characteristics and lateralization) point to its possible association with the event. Nevertheless, we assume that it is unclear if these patients with acute dissection-headache had persistence of this symptom for 2.5 years, or if the acute headache resolved and another headache disorder developed in the meantime, or the alternative explanation of persistence of headache in a patient with a history of previous headache. One of the ways to overcome this misclassification bias would be to carry out a prospective study, with more information about each headache subtype, as performed in the study by Lebedeva et al. (15). We also recognize that our study may have a recall bias, since the information collected was acquired via telephonic questionnaires years after the event and, because of that, patients could not precisely remember every aspect regarding the dissection and the persistence of headache after it. Also, because of the retrospective nature of the data, and since it was partially based on electronic records, a precise description of the headaches after the acute dissection event was, sometimes, difficult to obtain. The existence or not of headache in these patients, may be underdiagnosed, as we relied on medical records from vascular neurology and general neurology outpatient consultations that can inadvertently omit information on headache.
Conclusion
In our study, a quarter of patients with a history of dissection had HPCCAD, with features of both migraine and tension-type headache, and commonly reported pulsatile characteristics. Daily headaches were reported by a considerable number of patients, that encompassed years after the initial event. Previous headache history, headache/neck pain on admission, posterior circulation dissection, and less severe disease were implied as having significant prevalence among patients with persistent headache after arterial dissection. As headache persistence potentially affects rehabilitation potential, functional outcomes, and quality of life, further research, especially in the form of a prospective study, is needed to fill the lack of information gap regarding its risk factors, and to make it easier and more reliable to characterize this type of headache.
Article highlights
Headache persistence post-CCAD is common, and frequently affects patients daily. Patients with headache persistence after CCAD seem to have more frequently a previous headache history (more often migraine), headache/neck pain at admission, greater involvement of the posterior circulation, and a less severe disease. Headache persistence post-CCAD potentially affects rehabilitation potential, functional outcomes, and quality of life. This study helps to identify risk factors of headache persistency after arterial dissection, which may contribute to helping clinicians manage these patients after the event, and so increase their quality of life.
Footnotes
Author statement
Bárbara Pinto Martins, Neurology resident at Centro Hospitalar Universitário São João, on behalf of the authors, takes full responsibility for the data presented in this study and conclusions. All authors have read and agree with the submitted version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics statement
All participants included in the study gave their informed consent. The study was approved by the hospital ethics committee. All data generated or analyzed during this study are included in this published article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.