
Abstract
Objective
We aimed to determine the association between iron deficiency anemia and chronic daily headache.
Methods
This case-control study was conducted in a tertiary care center in Dehradun, India. One hundred patients with chronic daily headache were randomly selected for the study with an equal number of controls. Subsets of chronic daily headache were diagnosed as per the 3rd edition of the International Classification of Headache Disorders. The study participants were assessed for iron deficiency anemia.
Results
The mean age of the patients was 51.1 ± 22.1 years. Male: female ratio was 1:1.08. Chronic migraine was present in 62 (62%), tension-type headache in 23 (23%), and new daily persistent headache in 15 (15%) patients. The majority (96%) of patients had chronic daily headache of mild to moderate severity. Chronic daily headache was of long duration in all patients. Sixty-four (64%) patients had anemia of which 51 (51%) patients had iron deficiency anemia. Iron deficiency anemia showed a significant association with chronic daily headache (p < 0.001), but not with its type, subtype, and duration. Severe iron deficiency anemia had a significant association with the severity of chronic daily headache (p = 0.021). Serum iron, ferritin, total iron-binding capacity, and transferrin saturation also had a significant association with chronic daily headache (p < 0.05 for each), but not with its type, subtype, duration, and severity. Logistic regression analysis showed that iron deficiency anemia, total iron-binding capacity, and transferrin saturation had an independent association with chronic daily headache (p < 0.05 for each).
Conclusions
Iron deficiency anemia had an independent association with chronic daily headache. Severe iron deficiency anemia was related to the severity of chronic daily headache.
Keywords
Introduction
Headache is often considered a minor illness affecting almost 95% of the population sooner or later in their lifetime, at times it can even prove to be a very upsetting and debilitating both mentally and physically (1). It is believed that at least 4% of the general population chronically suffers from this condition (2).
It has been observed that out of all the patients presenting with headache in the neurology clinic, around 40% satisfy the criteria for chronic daily headache (CDH) diagnosis and 80% of patients with CDH are female (3).
The persistent nature of CDH not only affects quality of life and work performance of an individual but also burdens them with the additional cost of related health care. Even after the diagnosis of CDH is established, the disease does not respond very well to the conventionally accepted approach for treating episodic headaches (4).
CDH can be of both primary and secondary origin. Although secondary CDH is not very commonly encountered, it must be excluded first before establishing the diagnosis. Seventy-eight percent of the patients presenting in clinics with primary CDH are diagnosed with chronic migraine while 15% fall into the tension-type headache (TTH) category (5).
Often CDH is associated with various etiologies, and anemia is one of them. Anemia is one of the major health concerns in developing countries, with females in the reproductive age group representing the most vulnerable section of society (6). Country-wide surveys demonstrate that the majority of the female population in India suffers from anemia (55%). The most common cause attributed to this is the deficiency of the micronutrient iron, with data as high as 2 billion globally (7). Various factors like economic status, the standard of living, and the degree of awareness regarding healthy dietary practices have contributed to the high incidence of this micronutrient deficiency (8). Low-income levels and poor dietary habits owing to a lack of information make it even more common in developing nations (9). Also, dependent age groups, like infants, older people and menstruating adolescent girls, are at a higher risk of developing iron deficiency anemia (IDA) (10).
Iron deficiency disturbs many processes at the cellular level, such as oxygen storage and delivery, energy production, myelination, synthesis of genetic material, immune system activation, transport of electrons, and neurotransmitter metabolism (11). Iron not only affects the dopamine levels in the central nervous system but also affects the metabolism of several other neurotransmitters like serotonin and norepinephrine. Both dopamine and serotonin have been seen as the causative agent for chronic headaches among patients. Serotonin is the key neurotransmitter in the pathophysiology of migraine attacks. During migraine exacerbation, it has been seen that the levels of serotonin increase in the peripheral nervous system, and at the same time its levels rise in the central nervous system (12). Iron deficiency leads to several biochemical, physiological as well as morphological changes even before the conventional signs of anemia become apparent due to a fall in hemoglobin levels (13). Deficiency of this micronutrient presents less commonly as reduced academic and work achievement and altered bowel function (10).
Iron also plays an important role in the morphological development of the brain. The deficiency of this micronutrient alters neuronal development in early infancy and may also lead to a reduction in the neuronal activity of the brain. This alteration in brain physiology is attributed not only to defective myelination but also to reduced dopamine metabolism in the brain. However, neuronal changes that happen in the adolescent and older age groups are seen to be easily reversed once the supplementation is initiated. Thus it becomes imperative to diagnose this condition as early as possible (13).
It has been also shown that there is a connection between migraine and IDA (12). The presence of migraine has been correlated with any pre-existing mental health condition like anxiety and depression in patients suffering from a deficiency of this micronutrient. Disorders like attention deficit, hyperactivity problems, anxiety, and disrupted social behavior are frequently seen in patients with iron deficiency, and hence, it must be considered as the differential diagnosis of such patients (11).
However, no study has been conducted so far to examine the link between IDA and CDH in the Indian population. This study was conducted to determine the association of IDA with CDH and its type, subtype, severity, and duration.
Material and methods
This study was conducted in the Department of General Medicine, Himalayan Institute of Medical Sciences (HIMS), Dehradun, India from April 2020 to December 2021. Patients attending the Himalayan Hospital, Dehradun, with a diagnosis of CDH were included in the study after written informed consent was obtained from the patients and ethical clearance from the institutional ethics committee. An equal number of age- and sex-matched controls without CDH were included in the study.
Study design
In this case-control study, a sample size of 95 cases with CDH and 95 age- and sex-matched controls was estimated for detecting a significant association between IDA and CDH at a power of 80% and a 5% level of significance, assuming the frequency of CDH as 16% in the patients with IDA and 4% in the patients without IDA, based on the results of a small pilot study conducted by us in the hospital. The sample size was increased to 100 in each group to adjust for the possibility of dropouts.
Inclusion Criteria
Patients above the age of 18 years with CDH, primary in nature
Of 3089 patients with chronic daily headache attending the medicine/neurology outpatient department (OPD), 93 patients had CDH secondary in nature and did not meet the eligibility criteria. Of 2996 patients who satisfied the eligibility criteria, 37 patients refused to participate in the study during the random selection of the cases using a random number table. In event of a patient refusing to participate in the study, the slot was filled by the patient as per the next number in the random number sequence. In all, 100 patients were selected for the study.
CDH was defined as a headache occurring on 15 or more days in a month for at least three months (1). It was divided into primary and secondary which was further subdivided into headaches of short or long duration (2). Headache of short duration was defined as lasting less than four hours, whereas a headache of long duration was defined as lasting more than or equal to four hours (14,15).
The short-duration headaches included various trigeminal autonomic cephalalgias (TAC) comprising cluster headache (CH), paroxysmal hemicrania (PH), and others like hypnic headaches and primary stabbing headaches. Headaches of long duration included chronic migraine (CM), chronic tension-type headaches (CTTH), hemicrania continua (HC), and new daily persistent headaches (NDPH) (16). The criteria used for CDH subtypes were as per the 3rd edition of the International Classification of Headache Disorders (ICHD-3) (17).
Patients with secondary CDHs, such as post-traumatic headaches and headaches due to temporal arteritis, idiopathic intracranial hypertension, or spontaneous intracranial hypotension, were excluded from the study.
The severity of headache was assessed by an 11-point numeric rating scale (NRS) ranging from 0 to 10, with 0 denoting “no headache at all” and 10 denoting “the worst possible headache.” NRS scores of 1 to 3, 4 to 6, and 7 to 10 were considered mild, moderate, and severe headaches, respectively (18).
Study protocol
Patients presenting with headache were subjected to a detailed history, clinical examination, and evaluation for structural abnormalities or other causative lesions. Those diagnosed as having CDH primary in nature were randomly selected for the study to avoid any bias. The patients having anemia were further evaluated for IDA.
The following investigations were done: complete hemogram, erythrocyte sedimentation rate, fasting blood sugar, liver function tests, kidney function tests, computed tomography (CT) scan/magnetic resonance imaging (MRI) of the brain, and x-ray cervical spine (wherever required).
Those with anemia were assessed for general blood picture, reticulocyte count, serum lactate dehydrogenase (LDH), serum iron, ferritin, total iron-binding capacity (TIBC), stool examination (routine and for occult blood), hemoglobin electrophoresis, bone marrow examination, serum vitamin B12, serum folate, and any other investigation, if required.
Anemia was defined as a low level of hemoglobin in the blood, as evidenced by a fewer number of functioning red blood cells, and was classified into mild anemia (11–12.9 gm/dl), moderate anemia (8–10.9 gm/dl), and severe anemia (<8 gm/dl) as per WHO criteria (19).
IDA was defined as hemoglobin <13 g/dl in males and <12 g/dl in females and TIBC > 360 mcg/dl, percent transferrin saturation <10, and serum iron <30 mcg/dl (20).
Data management and statistical analysis
Statistical analysis was performed using SPSS software version 22. The normality of the data was tested by the Kolmogorov-Smirnov test. Unpaired Student’s t-test was used for the comparison of various parameters pertaining to normally distributed continuous data. Non-normally distributed data were compared by the Mann Whitney U test.
Odds ratios (ORs) were estimated to determine the effect. The Chi-square test was used for the comparison of qualitative data and for measuring the association between different variables. Multivariate analysis was performed to determine the independent association between variables using logistic regression. A p-value of less than 0.05 was considered statistically significant.
Results
The demographic characteristics of patients are shown in Table 1. The mean age of the patients was 51.1 ± 22.1 years. Female preponderance was seen in patients with CDH.
Demographic characteristics of cases and controls.
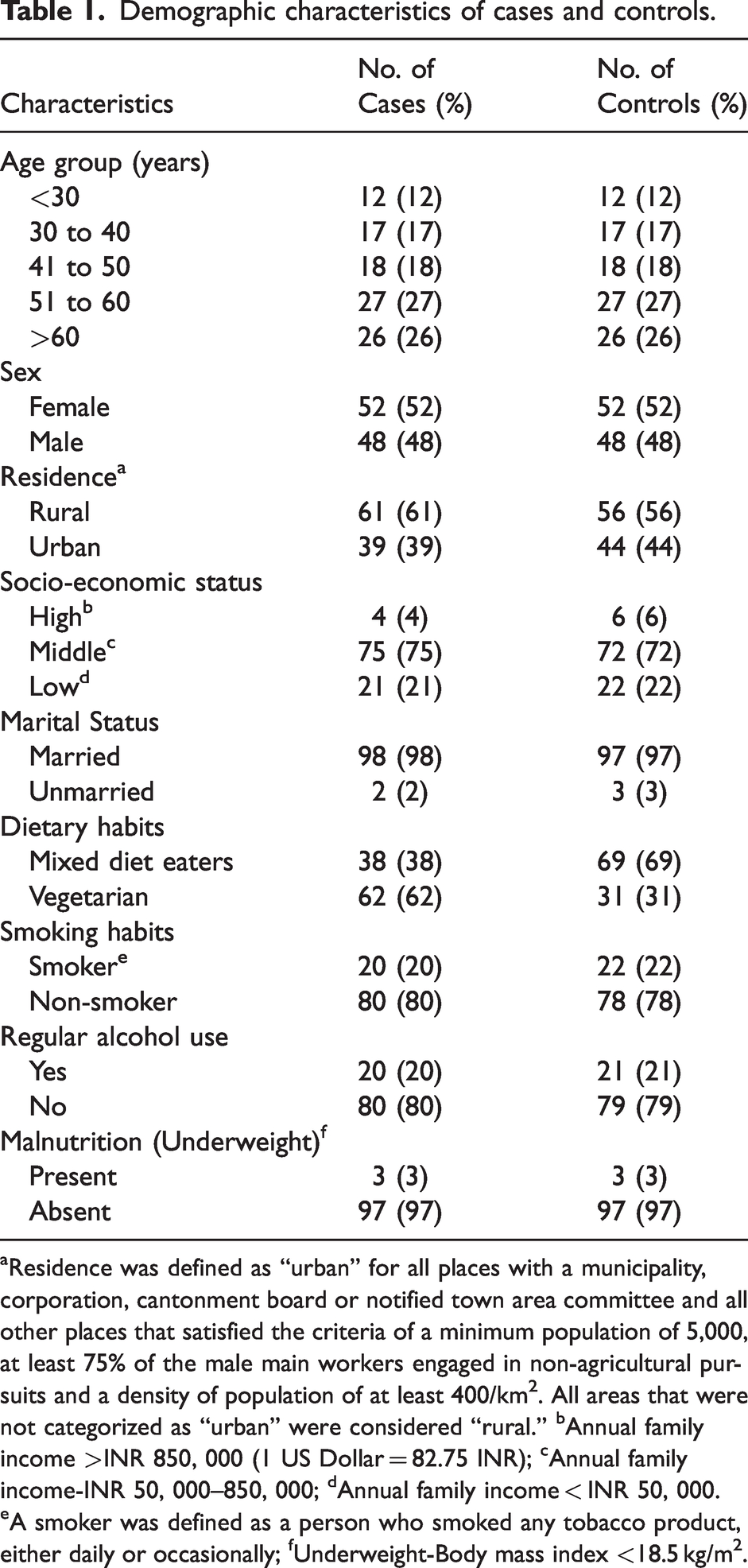
aResidence was defined as “urban” for all places with a municipality, corporation, cantonment board or notified town area committee and all other places that satisfied the criteria of a minimum population of 5,000, at least 75% of the male main workers engaged in non-agricultural pursuits and a density of population of at least 400/km2. All areas that were not categorized as “urban” were considered “rural.” bAnnual family income >INR 850, 000 (1 US Dollar = 82.75 INR); cAnnual family income-INR 50, 000–850, 000; dAnnual family income < INR 50, 000. eA smoker was defined as a person who smoked any tobacco product, either daily or occasionally; fUnderweight-Body mass index <18.5 kg/m2.
In the majority of patients, the severity of the headache was mild to moderate. In all patients, the headache was of a long-duration type. Chronic migraine was the commonest subtype of CDH (Table 2). Most patients with chronic migraine were above 30 years of age (52/62 cases, 83.9%).
Clinical profile of cases.
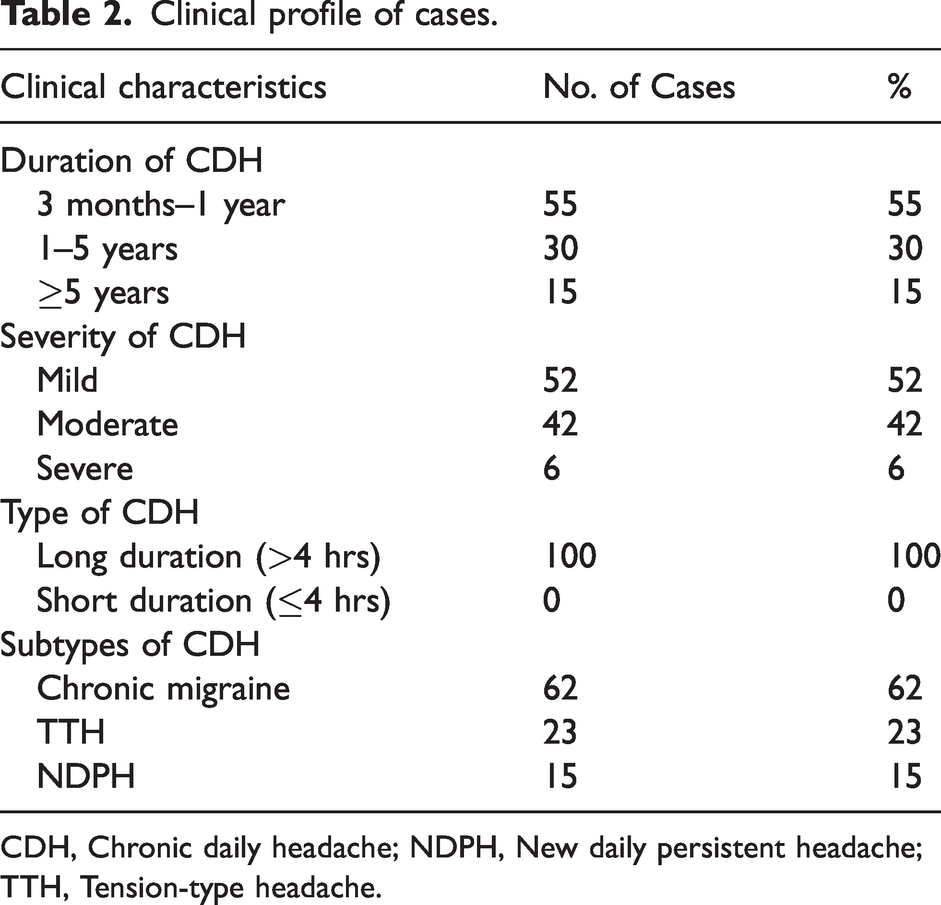
CDH, Chronic daily headache; NDPH, New daily persistent headache; TTH, Tension-type headache.
Mean hemoglobin (p < 0.001), red blood cell (RBC) count (p = 0.006), packed cell volume (PCV) (p < 0.001), serum albumin (p = 0.046), and iron (p = 0.001) were significantly lower while red cell distribution width (RDW) (p < 0.001) and TIBC (p < 0.001) were higher among cases than in controls. No significant differences were seen between cases and controls regarding other laboratory parameters (Table 3).
Laboratory investigations of cases and controls.
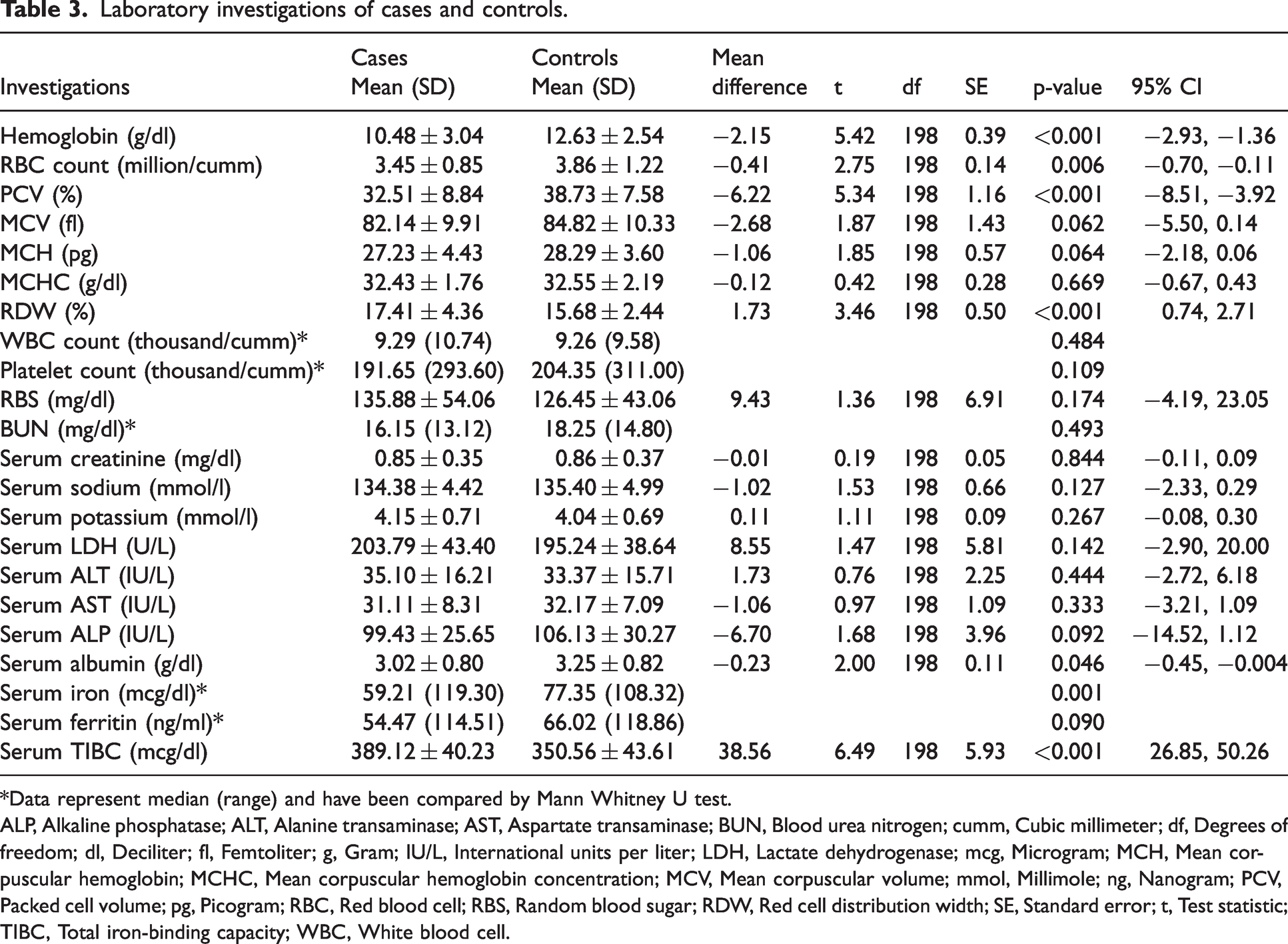
*Data represent median (range) and have been compared by Mann Whitney U test.
ALP, Alkaline phosphatase; ALT, Alanine transaminase; AST, Aspartate transaminase; BUN, Blood urea nitrogen; cumm, Cubic millimeter; df, Degrees of freedom; dl, Deciliter; fl, Femtoliter; g, Gram; IU/L, International units per liter; LDH, Lactate dehydrogenase; mcg, Microgram; MCH, Mean corpuscular hemoglobin; MCHC, Mean corpuscular hemoglobin concentration; MCV, Mean corpuscular volume; mmol, Millimole; ng, Nanogram; PCV, Packed cell volume; pg, Picogram; RBC, Red blood cell; RBS, Random blood sugar; RDW, Red cell distribution width; SE, Standard error; t, Test statistic; TIBC, Total iron-binding capacity; WBC, White blood cell.
Anemia was present in 64 (64%) of patients with CDH. Anemia was severe in 25% (16/64), moderate in 53.1% (34/64), and mild in 21.8% (14/64) patients with CDH and anemia. Anemia was present in a significantly higher number of patients with CDH than in controls (64 cases versus 39 controls; p < 0.001). Among controls with anemia, the highest percentage was found in the mild anemia category (19/39 controls, 48.71%). Moderate anemia was present in 38.46% (15/39) and severe in 12.82% (5/39) controls. The difference between numbers of cases and controls with severe anemia was not significant (p = 0.216). Anemia showed a significant association with CDH (p < 0.001) and its duration (p = 0.016), but not with type, subtype, and severity of CDH.
IDA was present in 51 (51%) of the patients. IDA was most commonly seen in patients of middle age (28/51 cases, 54.9%). A significant association was seen between IDA and CDH (OR = 2.96, p < 0.001). No significant association was found between IDA and type, subtype, and duration of CDH. The severity of IDA did not show a significant association with CDH and its type, subtype, and duration. Severe IDA had a significant association with the severity of CDH (OR = 9.44, p = 0.021).
A significant association was seen between serum iron and CDH (OR = 2.96, p < 0.001). Serum iron did not show a significant association with type, subtype, severity, and duration of CDH. A significant association was seen between serum TIBC and CDH (OR = 3.08, p < 0.001). No significant association was found between serum TIBC and type, subtype, severity, and duration of CDH. Serum ferritin had a significant association with CDH (OR = 1.99, p = 0.042), but not with its type, subtype, severity, and duration. The transferrin saturation showed a significant association with CDH (OR = 2.92, p < 0.001), but not with its type, subtype, severity, and duration (Table 4).
Association between iron deficiency anemia and chronic daily headache-related variables.

CDH, Chronic daily headache; CI, Confidence interval; NDPH, New daily persistent headache; OR, Odds ratio; TTH, Tension-type headache.
Out of the analyses regarding the association between various variables, multiple variables like IDA, serum iron, ferritin, TIBC, and transferrin saturation having significant association with CDH on univariate analysis, were examined for independent association with CDH by logistic regression analysis which showed that IDA (p < 0.001), TIBC (p = 0.001) and transferrin saturation (p < 0.001) had an independent association with CDH while serum iron (p = 0.182) and ferritin (p = 0.122) were not independently associated with CDH (Table 5). Logistic regression analysis was not done for determining the independent predictors of the type, subtype, severity, and duration of CDH as none of the IDA-related variables showed significant association with type, subtype, and duration of CDH while only one variable was found to have a significant association with the severity of headache.
Showing independent predictors of chronic daily headache by logistic regression analysis.

B, Coefficient for the constant; CI, Confidence interval; df, Degrees of freedom; IDA, Iron deficiency anemia; OR, Odds ratio; SE, Standard error; TIBC, Total iron binding capacity; Wald, Wald chi-square value.
Discussion
IDA is not only the most common cause of anemia in the world but is also regarded as the most prevalent form of malnutrition. Globally, 50% of anemia is attributed to iron deficiency. It develops in two million individuals every year, causing death in 700,000 annually (21).
We observed that most of the CDH cases were middle-aged with a mean age of 51.1 years. Migraine was most frequent in subjects older than 30 years of age (83.9%). However, in general, the frequency of migraine was found to decrease with age in another study (11).
Female preponderance (52%) was seen in cases as well as controls having IDA. IDA was most commonly seen in patients of middle age. This may be due to the lifestyle of these patients as they get less time to have a proper diet due to the engagement of most of them in their jobs.
Most (61%) of our patients belonged to rural areas and middle (75%) and low (21%) socio-economic status. This suggests that IDA is more prevalent in rural areas where there is less availability of healthcare facilities in comparison to urban areas. Moreover, low and middle socio-economic status in most of our cases could have affected their knowledge and awareness regarding IDA due to low levels of education, leading to increased prevalence of IDA among this segment of the population. The threat potential builds even more as most of the population in the study resided in villages. This is in accordance with an NHS survey in India showing the prevalence of anemia more in the rural population (22). Moreover, the prevalence of IDA is almost similar in different states of India, as per the district levels household survey (DLHS) (23).
In our study, the majority of the cases were vegetarian (62%). In a study conducted in Saudi Arabia, the most well-known significant variables of anemia were insufficient vitamin C intake, low utilization of red meat, and family history of IDA (24), though, in other studies, the most well-known critical elements discovered were irregular breakfast, rare utilization of vegetables/natural products, meat, fish, chicken, tea-drinking, low household income, smoking, bleeding disorder, and gender (21,25,26). These studies proposed that IDA can be forestalled by giving legitimate information on a healthy diet, improved way of life, and the harmful impact anemia can have on a person. However, in our study, confounding factors of malnourishment and dietary habits were not present as a cause of IDA.
The majority (62%) of the patients suffering from CDH were diagnosed with chronic migraine, while the remaining patients were diagnosed as having TTH (23%) and NDPH (15%). Similar observations were made by Pascual et al. that about 60% of CDH patients suffer from chronic migraine, 20% from TTH, and 20% meet NDPH criteria (27).
In our study, hemoglobin, hematocrit, RBC count, and serum iron were lower whereas RDW and TIBC were higher in the patients as compared to controls. These differences were due to a higher prevalence of IDA among patients.
Several studies have been conducted in the past which attempted to understand the mechanism behind the connection of headache with anemia (28,29). One possible mechanism is the altered dopaminergic function caused by IDA. Change in dopaminergic function is considered one of the migraine triggers. Jellen et al. found that iron deficiency induces changes in genes that affect dopamine functioning (28). Another study by Akerman et al. (29) also found an association between dopamine and headache.
Although the relationship between anemia and headache is accepted in neurology practice, studies examining iron deficiency or metabolism in patients with CDH are in limited number. Although these studies looked at the role of iron deficiency in patients with headache, they could not establish a definite relationship between the two (30,31). Anemia observed in 64% of patients with CDH was moderate in more than half (53.1%) of patients while anemia seen in 39% of controls was mostly of the mild form (48.71%). No significant difference was present between the numbers of cases and controls having severe anemia. However, the association of CDH with anemia was found to be statistically significant (p < 0.001). On the contrary, in another study, Aamodt et al. did not find any correlation between anemia and headache patients and noted a decrease in the prevalence of headache with a decrease in hemoglobin levels (30).
In our study, there was a significant association between CDH and IDA (p < 0.001). However, case-control studies do not confirm temporality. Therefore, the association between iron deficiency anemia and CDH may be bidirectional, but the odds weigh in favor of iron deficiency anemia as a risk factor for CDH because iron deficiency anemia patients have a high frequency of headache like migraine (11).
Among CDH subtypes, chronic migraine was the major subtype. All the patients in the study had a long duration of headache with a total absence of patients with a short duration of headache. Patients with moderate severity of IDA constituted the majority of patients with CDH. Our results are in accordance with several other studies which suggested a relationship between IDA and migraine (11,12,31–33). The presence of a significant association between severe IDA and the severity of CDH implies that patients with severe IDA are more prone to develop severe CDH.
In a study conducted by Gür-Özmen and Karahan-Özcan (31), a relationship was observed between IDA and migraine which was more significant among women and girls. This is because the relative prevalence of IDA in women and girls suffering from migraine was higher in comparison to men and boys. Additionally, a significant relationship was found between migraine and hemoglobin levels (12).
In another study by Pamuk et al. IDA patients had high levels of migraines, depression, and stress, which is indicative of the underlying relationship between IDA and these states, including disorders of the central nervous system (11). A similar study conducted by Tayyebi et al. in Iran found a significant relationship between IDA and migraine (12).
We also examined the relationship of CDH with serum iron, ferritin, and TIBC. Serum ferritin is an important biomarker of body iron storage and a reliable indicator of body iron metabolism (34). We found a significant association between low serum ferritin and CDH while this was absent for type, subtype, and severity of CDH. However, a study conducted by Aamodt et al. showed no association between serum ferritin levels and headache prevalence (30). We observed low serum iron in 51% of patients with CDH. Serum iron, TIBC, and transferrin saturation showed a significant association with CDH, but no significant association with type, subtype, and severity of CDH.
However, in another study, Demirel et al. found that the patients in the migraine group correlated with elevated levels of ferritin, and decreased levels of TIBC while in TTH patients, the increased frequency of headache was found to be correlated with decreased levels of Hb, hematocrit, ferritin, and increased level of TIBC (35).
IDA, TIBC, and transferrin saturation also showed an independent association with CDH which, however, could not be confirmed due to the lack of such studies in the literature. We also observed that serum iron and ferritin were not independent predictors of CDH.
Thus IDA appears to have a relationship with the CDH in the Indian population.
Strengths of the study
This is the first such study on the Indian population. The study suggests a relationship between IDA and CDH though not necessarily a causal one.
Our findings are important from a public health perspective since IDA is rampant all over the globe, particularly in developing countries (36) with a prevalence rate of 57% in women and 25% in men of 15–49 years of age in India (22), 21.2% in Liberia, 18.7% in Philippines, and 17.3% in Mozambique (37). An increased risk of CDH can add to the cost of health care besides overburdening the health resources in such countries.
Limitations of the study
Our study was not a community-based study. The study findings may be slightly biased as they are based on the data from a single referral center. The positive results of many single-center trials are often not corroborated in multicenter settings (38). Moreover, as the study was conducted in a referral center, the prevalence of IDA in patients with CDH may be slightly higher than in the community. However, this disadvantage was counterbalanced to some extent by the random selection of the subjects with CDH. There is a possibility that there may be residual bias due to differences in the middle-income group that can confound the results since 3/4 of cases and controls are in this category. However, differences in the middle-income group are not likely to create a significant bias as the majority of cases and controls are from the same category.
The number of cases may be inadequate to generalize the findings even though cases were taken as per the estimated sample size. One cannot ascertain the causal association between IDA and CDH based only on this study result as the results of case-control studies may differ from those of cohort studies. A study with a larger sample size and/or a multi-centered study is required for the generalization of the findings which is beyond the scope of the present work.
Conclusions
IDA had an independent association with CDH. No significant association was present between IDA and the type, subtype, and duration of CDH. Severe IDA had a significant association with the severity of CDH but not with its type, subtype, and duration.
TIBC and transferrin saturation had an independent association with CDH while serum iron and ferritin did not. Serum iron, ferritin, TIBC, and transferrin saturation were not associated with the type, subtype, duration, and severity of CDH.
Thus all patients with CDH should be screened for IDA as it can be easily corrected and may have a role in the causation of CDH.
Article highlights
Iron deficiency anemia is strongly associated with chronic daily headache. Severe iron deficiency anemia may increase the risk of chronic daily headache of severe nature.
Footnotes
Acknowledgments
We thank Abhinav Bahuguna, Department of Biostatistics, Swami Rama Himalayan University, Dehradun, India for his help in the statistical work. We are thankful to Madhurima Kaushik for carefully going through the manuscript.
Data availability statement
Data available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of Swami Rama Himalayan University, Dehradun, India (SRHU/HIMS/ETHICS/2021/117 dated 19.11.2019). The study was performed in line with the principles of the Declaration of Helsinki and its later amendments.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received an intramural grant from Swami Rama Himalayan University, Dehradun, Uttarakhand, India (No. SRHU/Reg/Int/2020-80 (18) dated 22.2.2020).