
Abstract
Background
Cytokines are important endogenous substances that are involved in immune and inflammatory responses. Neurogenic inflammation has been proposed to play a role in migraine involving altered cytokine levels. Therefore, we aimed to provide a systematic review on the current knowledge on cytokine levels in migraine patients during and outside attacks.
Methods
Databases of PubMed and Embase were systematically searched for studies investigating cytokine levels in migraine patients during and outside attacks.
Results
Screening yielded identification of 45 articles investigating 18 cytokines in total. We found that the interictal level of the anti-inflammatory cytokine, interleukin 10, was decreased, while the level of transforming growth factor beta 1 was increased in migraine patients compared to controls. Levels of pro-inflammatory cytokines, tumor necrosis factor α and interleukin 6, were increased outside attacks compared to controls. Ictal levels of cytokines were unchanged or varying compared to the interictal state in migraine patients. Three studies reported dynamic cytokines levels during the course of an attack.
Conclusion
The findings of the current review underline a possible involvement of cytokines in the proposed inflammatory mechanisms of migraine. However, future studies are needed to expand our knowledge of the exact role of cytokines in the migraine pathophysiology with focus on cytokines TNF-α, IL-1ß, IL-6 and IL-10 while applying refined methodology.
Introduction
Neurogenic inflammation has been suggested as an important mechanism involved in the migraine attack pathophysiology (1–3). Clinically, non-steroidal anti-inflammatory drugs may indeed effectively abort migraine attacks (4). While the exact mechanisms of the neurogenic inflammation in migraine are unclear, an important role of cytokines has been implicated (1).
Cytokines hold pro- or anti-inflammatory properties and are involved in modulating mobilization of immune cells (5–7) as well as activation of the pain pathways through trigeminal sensitization (3). Previous studies in migraine patients have shown that pro-inflammatory cytokines, such as interleukin (IL) 1ß and tumor necrosis factor α (TNF-α), may increase during or outside the attack state in migraine (8,9). Preclinical studies have also shown that pro-inflammatory cytokines, including IL-1β and IL-6, may activate and sensitize both meningeal and muscle nociceptors (10–12). These findings suggest that cytokines may play a role in stimulating meningeal nociceptors and thereby contribute to migraine pain. Changes in anti-inflammatory cytokine levels have been suggested as a reaction to the increased pro-inflammatory cytokines levels, re-establishing the balance during a migraine attack (13,14).
The question is to what extent the pro- and anti-inflammatory cytokines are involved in the migraine pathophysiology. To elucidate this, we found it timely to conduct a systematic review to identify studies that investigated the cytokine levels in migraine patients during and outside attacks.
Methods
Data source
This review is conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines (15). Articles on cytokines and their roles in primary headache were obtained through a search on PubMed and Embase on August 18th 2021. The following search string was used, “(“headache”[MeSH Terms] OR “headache”[All Fields] OR “headaches”[All Fields] OR “headaches”[All Fields]) AND (“cytokin”[All Fields] OR “cytokine s” [All Fields] OR “cytokines”[MeSH Terms] OR “cytokines”[All Fields] OR “cytokine”[All Fields] OR “cytokinic”[All Fields] OR “cytokins”[All Fields])” with the filter “English”.
Selection criteria
The inclusion criteria were clinical studies with migraine patients, diagnosed according to the International Classification of Headache Disorders (ICHD) (16–18), where the cytokine levels were investigated in the ictal or interictal state. The exclusion criteria were articles in a non-English language, other headache types, pre-clinical studies, reviews, case reports, conference abstracts and studies that focused on genetics.
Study inclusion and data extraction
Two investigators (JT and ME-J) independently screened all articles by title and abstract, and relevant articles were selected for full-text screening to determine eligibility. We also screened the reference lists of included studies to identify additional eligible studies. In case of disagreements, these were solved via consultation with one of two independent senior investigators (HWS and SY).
Two investigators extracted data independently (JT and SY). Following data were extracted: number of participants, type of migraine, female to male ratio, mean age of patients, monthly attack frequency, source of samples and whether samples were collected in the ictal or interictal state in migraine patients. The main objectives were data extraction on cytokines levels where interictal levels in migraine patients were compared to healthy controls, while ictal and interictal levels were compared within patients.
Cytokines
Cytokines are sub-divided into pro- and anti-inflammatory cytokines based on how they predominantly influence the interaction and communication between cells (19). Overview of the unique function of each cytokine is reported in Table 1.
Characteristics of anti- and pro-inflammatory cytokines.
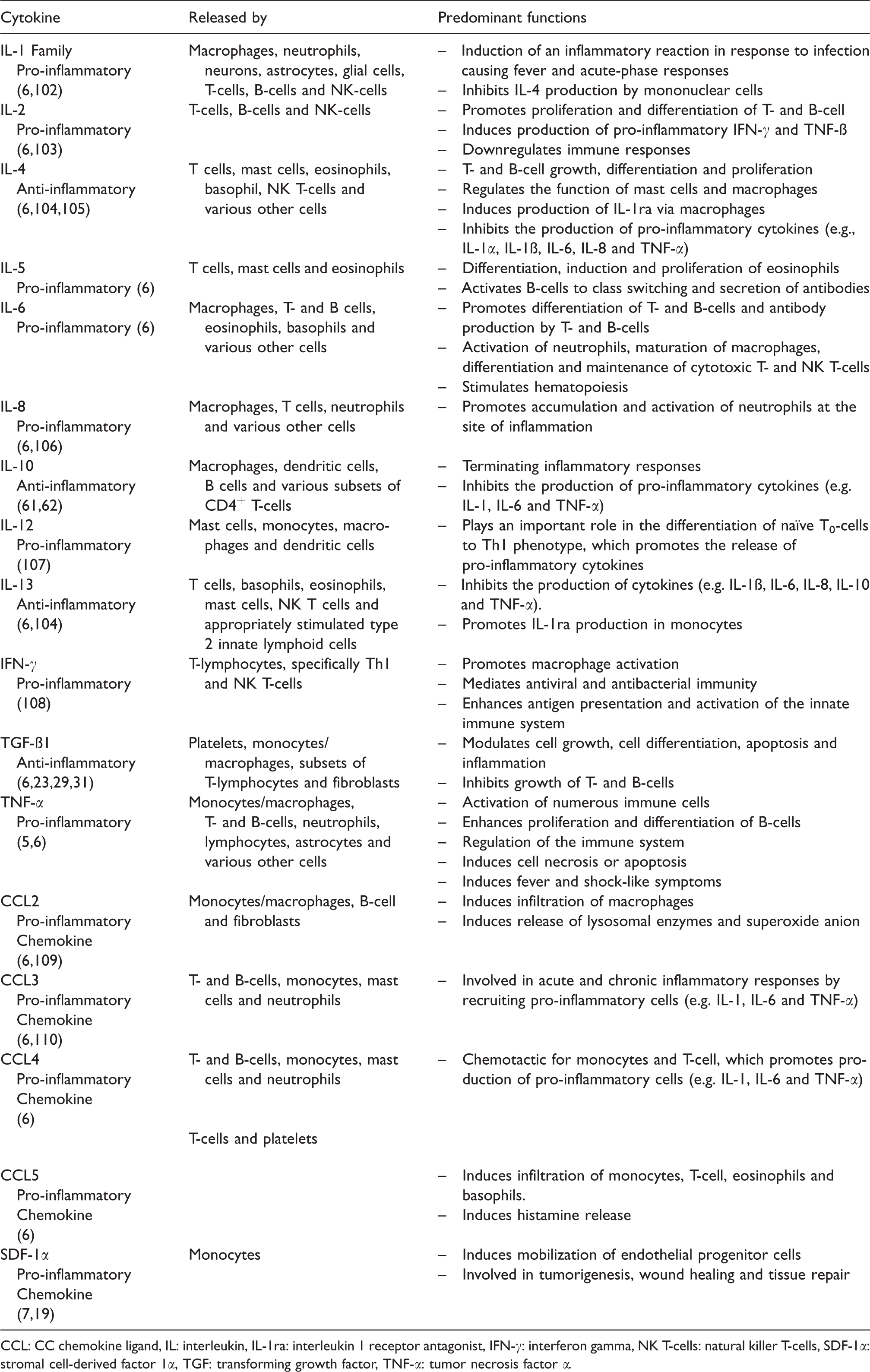
CCL: CC chemokine ligand, IL: interleukin, IL-1ra: interleukin 1 receptor antagonist, IFN-γ: interferon gamma, NK T-cells: natural killer T-cells, SDF-1α: stromal cell-derived factor 1α, TGF: transforming growth factor, TNF-α: tumor necrosis factor α.
Results
Literature search returned 2789 unique articles (Figure 1). Title and abstract screening yielded 50 articles for full-text screening, which resulted in the identification of 41 eligible articles. Four articles were found through reference screening of the 41 articles. In total, 45 articles were included in the systematic review. Hereof, 27 studies compared interictal cytokines levels between patients and healthy controls, while 16 studies compared the ictal and interictal levels within patients. The included studies investigated 18 types of cytokines (Table 2). Hereof, four cytokines have anti-inflammatory properties and 14 have pro-inflammatory properties.

Flow chart of the inclusion process.
Cytokine studies in migraine.

↑: increased, ↓: decreased, = : no significant difference, ßB: ß-blocker, CCL: chemokine ligand, CM: chronic migraine, CSF: cerebrospinal fluid, CTTH: chronic tension type headache, EM: episodic migraine, ETTH: episodic tension type headache, HC: healthy controls, HD: headache day(s), IL: interleukin, MM: menstrual migraine, MA: migraine with aura, MO: migraine without aura, MX: migraine that is not specified as migraine with or without aura, NA: not applicable, NR: not reported, nVNS: non-invasive vagus nerve stimulation, OTA: Onabotulinum Toxin A, PACAP: pituitary adenyl cyclase-activating polypeptide, SAH: subarachnoid hemorrhage, SD: standard deviation, SDF-1α: stromal cell-derived factor 1 α, SNRI: serotonin-norepinephrine reuptake inhibitor, SSRI: selective serotonin reuptake inhibitor, TCA: tricyclic antidepressant, TGF-ß: transforming growth factor beta, TNF-α: tumor necrosis factor α, TNF-ß: tumor necrosis factor beta, TOP: topiramate, TTH: tension-type headache, VM: vestibular migraine.
Study and patient characteristics
Eighteen studies included both migraine patients with and without aura (8,13,20–35), 11 studies included only migraine without aura (n = 11) (9,36–45), while only one study investigated migraine with aura patients (n = 1) (46). Two studies investigated patients with vestibular migraine (47,48). All studies included more females than males, except two studies, which included more males (20,21). Three studies investigated cytokine levels in children (10–18 years of age) (20,21,30). Mean age of patients in the remaining 42 studies ranged from 24 to 55 years of age. Four studies reported inclusion of patients only with episodic migraine (38,45,49,50), while two studies reported inclusion of only chronic migraine patients (51,52). Majority of the studies measured cytokines levels in the blood. Three studies measured cytokine levels in the cerebrospinal fluid (23,25,52), two studies measured levels in blood from the internal jugular vein (9,43), two studies from saliva (22,53) and one study from urine samples (54).
Anti-inflammatory cytokines
The most studied anti-inflammatory cytokines were IL-10 (14 studies) (8,13,21,23–25,28,32,41,42,47,51,55,56) and IL-4 (8 studies) (8,9,13,21,40–42,47). Studies mainly reported decreased interictal levels of IL-10 in migraine patients compared to controls (5 studies) (25,32,47,51,56), while three studies reported unchanged levels (8,13,28) and only one study reported increased levels (24) (Figure 2). There were no consistent reports of altered IL-10 levels during attacks of migraine compared to the interictal state (8,13,28,32) (Figure 3).
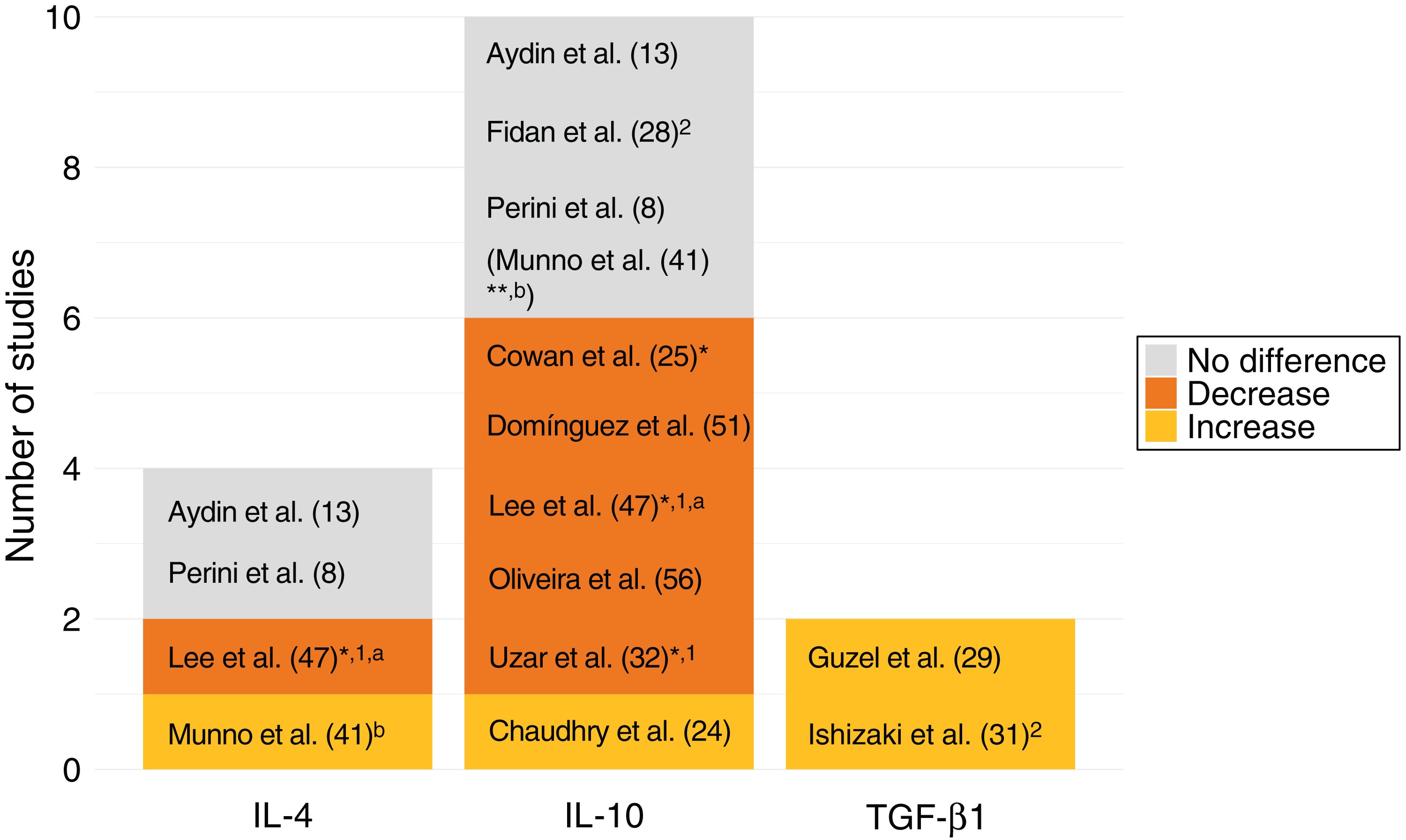
Interictal anti-inflammatory cytokines levels in migraine patients compared to controls.

Ictal anti-inflammatory cytokines levels compared to interictal levels in migraine patients.
Interictal investigations of IL-4 levels in migraine yielded varying outcome (8,13,41,47). Ictal IL-4 levels were decreased compared to the interictal state in three studies of migraine without aura patients (9,39,40). The ictal IL-4 levels were unchanged in two studies with a mixed cohort of patients with and without aura (8,13) and in one study of patients without aura (9).
Two studies investigated transforming growth factor beta 1 (TGF-ß1) and reported increased interictal levels in migraine patients compared to healthy controls, with no difference between patients with and without aura nor correlation to attack frequency (29,31).
Pro-inflammatory cytokines
The most studied pro-inflammatory cytokines were TNF-α (27 studies) (8,9,13,20,23–25,27,28,30,32,33,35–38,45,47–49,51,52,54,56–59), followed by IL-6 (20 studies) (8,9,13,24,25,27,28,30,32,34,35,39,47,48,51,53,54,56,58–60) and IL-1ß (16 studies) (8,9,22–24,28,30,32,33,35,47,48,53,54,56,59). The pro-inflammatory cytokines, IL-2 (5 studies) (8,28,32,44,47) and IL-8 (5 studies) (25,26,43,47,56), were less studied.
Studies investigating TNF-α mostly reported interictally increased levels in a mixed cohort of patients with and without aura compared to controls (13,30,35,56) (Figure 4), while ictal investigation mainly revealed unchanged levels compared to the interictal state (9,13,28,32,33,38,45) (Figure 5). Likewise, majority of studies reported increased IL-6 levels outside attacks in patients with and without aura compared to healthy controls (28,30,32,34,35,43,48,51,58–60). Six studies found unchanged IL-6 levels during attacks compared to outside attacks in mixed cohorts of patients with and without aura (8,9,13,32,34,48), while four studies reported increased ictal levels (28,35,53,59). In contrast, interictal investigations of IL-1ß levels mainly showed unchanged levels in migraine compared to controls (8,22,24,30,48,53,54,56). Three studies showed increased ictal levels of IL-1ß (8,35,59), while five studies showed unchanged ictal levels compared to the interictal state (9,28,32,33,48).
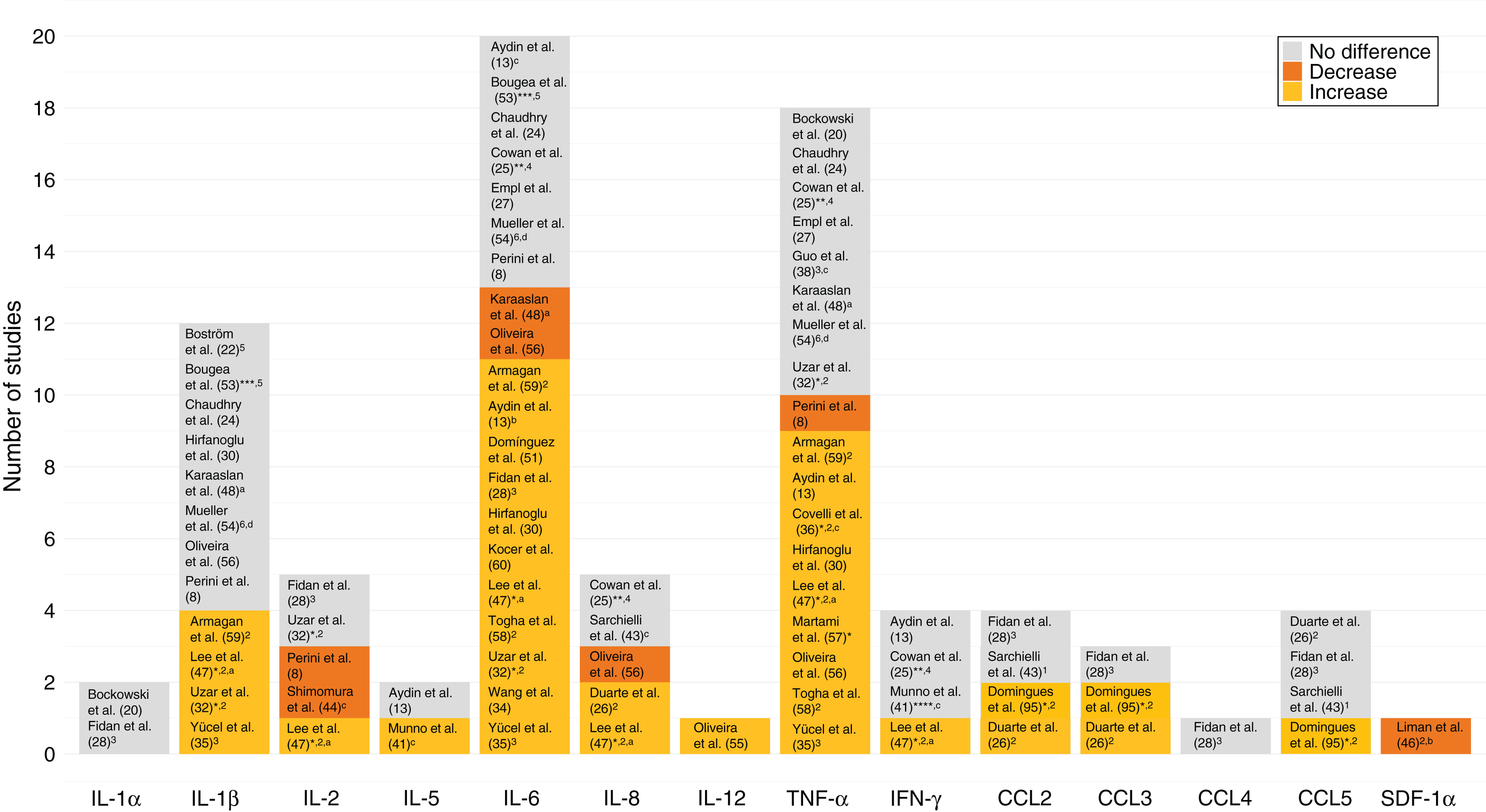
Interictal pro-inflammatory cytokine levels in migraine patients compared to controls.

Ictal pro-inflammatory cytokines levels compared to interictal levels in migraine patients.
Two studies in migraine without aura patients investigated cytokine levels in the internal jugular venous blood within 30 min after onset of attacks (9,43). These studies found increased levels of IL-1ß, IL-6, TNF-α (peak at 2 hours after attack onset) and IL-8 (peak at 4 hours after onset) as well as decreased levels of IL-4, all measured within a range of 1–6 hours after attack onset and compared to the early attack state (<30 min after onset) (9,43). No changes were found in the cytokine levels between the early attack state and within 2 hours after attack termination (9,43).
Only two studies investigated differences in cytokine levels between patients with episodic and chronic migraine (57,58). One of the studies reported increased IL-6 and TNF-α levels in chronic migraine compared to episodic migraine (n = 71), while levels in both groups were higher than in headache-free controls (58). The other study reported no difference in TNF-α levels between patients with episodic and chronic migraine, while levels were increased in both groups compared to controls (n = 43) (57).
Discussion
This systematic review identified altered levels of anti- and pro-inflammatory cytokines in migraine patients during and outside attacks.
Anti-inflammatory cytokines
The most studied anti-inflammatory cytokine was IL-10 followed by IL-4. Studies mainly showed decreased interictal levels of IL-10 in the blood of migraine patients (25,32,47,51,56), while there were no consistent ictal data (8,13,28,32) (Figure 2 and 3). Reports on IL-4 levels during or outside attacks were varying as well. IL-10 is involved in terminating inflammatory responses and downregulating the production of pro-inflammatory cytokines (61,62). Thus, the finding of increased IL-10 levels during attacks was suggested as an anti-nociceptive counterresponse to the release of pro-inflammatory cytokines (8,28). Moreover, decreased interictal IL-10 levels may suggest persistently insufficient regulation of the pro-inflammatory cytokine levels in migraine (32). Both IL-4 and IL-10 are released from Type 2 T helper (Th2) cells (28,42,56). It has been speculated whether imbalance or dysfunction in the cytokine release from Th2 cells plays a role in migraine pathophysiology (28,42,56). Interestingly, TGF-ß1 levels were increased interictally (29,31). TGF-ß1 is believed to act as a pro-inflammatory cytokine as well (63).
Pro-inflammatory cytokines
The most studied pro-inflammatory cytokines were TNF-α and IL-6 followed by IL-1ß. Studies mainly reported increased interictal levels of TNF-α and IL-6, while IL-1ß levels were unchanged (Figure 4). Ictal investigations showed mainly unchanged TNF-α levels, while reports of IL-6 and IL-1ß levels were inconsistent (Figure 5). Overall, the increased levels of pro-inflammatory cytokines outside of attacks may suggest an underlying sustained inflammation in migraine patients (26). In support, one recent study reported persistently increased inflammatory signal within the parameningeal tissue in the occipital region in migraine patients with aura measured by positron emission tomography (64). Similar findings were not detected in healthy controls nor patients with chronic low back pain, indicating that the reported finding was not a general pain feature (64). Increased pro-inflammatory cytokine levels during attacks have been proposed to be due to trigeminovascular activation during the headache phase of migraine (9), which may be stimulated by the release of calcitonin gene-related peptide (CGRP) from the trigeminal afferents (65).
Two studies found increased levels of pro-inflammatory cytokines (i.e. IL-1ß, IL-6, TNF-α and IL-8) and decreased levels of the anti-inflammatory cytokine, IL-4, measured in the internal jugular vein of migraine without aura patients at 1–6 hours after onset, compared to the early attack state. (< 30 min after onset) (9,43). Levels were not investigated in controls to exclude possible inflammatory response due to catheter insertion (9,43,66). Similar findings were reported for the CGRP levels in another study (67). The findings from the two internal jugular vein studies altogether suggest altered levels of cytokines during the course of an attack, possibly reflecting the dynamics of the inflammatory mechanisms (8,9,14,43). In support, one study reported that levels of both IL-10 and TNF-α correlated with time from attack onset (0–24 hours) (8). The levels of IL-10 and TNF-α were higher close to attack onset and decreased with temporal distance from onset (8). Infusion of neuropeptides in patients with migraine typically produces a delayed headache development of migraine attacks (68). Infusion of nitric oxide in rats, yielded delayed inflammatory response with detection of dural IL-1ß at 2 and 6 hours after infusion with a decline at 10 hours after infusion and increased IL-6 in dural macrophages and cerebrospinal fluid at 6 hours after infusion (69). This further supports the notion of altered cytokine levels during migraine attacks (9,43).
Three studies investigated the cytokine levels in the cerebrospinal fluid (23,25,53). The first study only detected IL-10 levels in the cerebrospinal fluid, which were unchanged in the ictal state in migraine patients compared to pain free controls (23). Samples were collected >12 hours after acute headache onset with no comparison to the interictal state in migraine patients (23). The second study investigated the following cytokines: IL-6, IL-8, IL-10, TNF-α and interferon gamma (IFN-γ) in both cerebrospinal fluid and plasma (25). This study found decreased interictal levels of IL-10 in plasma of patients compared to healthy controls, while there was no corresponding change in the cerebrospinal fluid (25). The last study measured ictal levels of TNF-α in cerebrospinal fluid and serum in chronic migraine patients, however there was no comparison to the interictal state or healthy controls (52). Based on these findings, we were unable to assess the correlation between the peripheral and central cytokine levels or whether the cerebrospinal fluid measurements may provide better cytokine profiles in migraine patients compared to peripheral measurements.
Increased pro-inflammatory cytokine levels have been proposed as an underlying mechanism involved in migraine chronification (3). In support, one study reported increased IL-6 and TNF-α levels in chronic migraine patients compared to episodic migraine patients (58). In contrast, three studies found no correlation of attack frequency or disease duration to increased levels of pro-inflammatory cytokines (i.e., IL-1ß, IL-5, IL-6, TNF-α and IFN-γ (41,48,57). The recent positron emission tomography study reported persistently increased inflammatory signal within the parameningeal tissue in the occipital region in a cohort of patients with a median attacks frequency of three attack per month (range: 1–11) (64).
Cytokines and CGRP
Calcitonin gene-related peptide (CGRP) is a potent vasoactive peptide widely distributed in the central and peripheral nervous system (70) and plays an important role in migraine pathophysiology (4,71). The exact role of CGRP in pain transmission is still not clear (72,73). Infusion of CGRP induces prominent vasodilation of cranial arteries and onset of attacks in migraine patients (68,74–78). The CGRP receptors are expressed in vascular smooth muscle cells in the human cranial vasculature (e.g. meningeal vessels), peripheral primary trigeminal afferents and the trigeminal ganglion (79–82), which are not protected by the blood-brain barrier (83). Neurogenic inflammation is believed to involve neuropeptides, such as CGRP, which lead to vasodilation, plasma protein extravasation, mast cell degranulation and release of pro-inflammatory mediators including cytokines (84). Majority of the included studies investigated peripheral levels of cytokines (see Table 2). Peripherally, the cytokines may be involved in sensitization of the meningeal afferents as well as the trigeminal ganglion neurons (83). One preclinical study showed that application of TNF-α to the meninges promoted delayed mechanical sensitization of meningeal nociceptors dependent of cyclooxygenase (COX) and activation of the p38 mitogen-activated protein (MAP) kinase signaling pathway (85). Dural, intraplantar, subcutaneous, intramuscular, intracisternal and intrathecal injection of IL-6 and allodynia, and thus hypersensitivity, was investigated in another preclinical study (86). Dose-dependent facial allodynia only developed after dural and intracisternal application of IL-6, suggesting activation of meningeal afferents and the trigeminal nucleus caudalis, respectively (86). This response was prevented by MAP inhibitor, indicating that dural application of IL-6 produces allodynia via involvement of the MAP kinase pathway (86).
Studies have also shown that CGRP stimulates the secretion of cytokines, such as IL-1ß, IL-6 and TNF-α from trigeminal ganglion neurons, satellite glia cells in trigeminal ganglion and T-cells (87–90). One of these studies observed upregulation of the MAP kinase signaling pathways following stimulation by CGRP, suggesting that prolonged increase in the cytokine levels may be mediated partly by these pathways (90). One study of lymphocyte-enriched mononuclear cells, isolated from healthy volunteers, showed that CGRP stimulated secretion of IL-1ß, IL-6 and TNF-α from the mononuclear cells (91). In this study, high concentrations of CGRP (0.3 µM–1 µM) was used to induce the cytokine response (91). In comparison, the CGRP levels were much lower in migraine patients when measured in the internal and external jugular blood (approximately 30 pM–90 pM) as well as in the peripheral blood (approximately 30 pg/mL–40 pg/mL) (43,67). These findings suggest that lower concentrations of CGRP may stimulate cytokine secretion in migraine patients, in contrast to healthy volunteers, supporting the notion that CGRP-induced upregulation of pro-inflammatory cytokine levels might be a unique feature of migraine.
Cytokines may also induce release of CGRP (92,93). One study in rats showed that TNF-α stimulated release of CGRP from trigeminal ganglion neurons involving activation of the MAP kinase pathways (92,93). Likewise, another study showed IL-1ß induced dose-dependent synthesis of COX-2 and prostaglandin 2, which yielded delayed release of CGRP from the rat trigeminal ganglia neurons (94). Moreover, this study reported that COX-2 selective and non-selective COX-inhibitors blocked the IL-1ß-induced CGRP release (93).
The bidirectional relationship between CGRP and inflammatory cytokines attest to a positive, inflammatory, neuron-glia loop, which promotes peripheral sensitization in the trigeminovascular system. Cytokine levels may increase up to 24 hours after stimulation by CGRP in trigeminal ganglion neurons (90,94) and satellite glial cells (89), supporting the notion of persistent activation and sensitization stimulated by cytokines. Thus, the cytokines are involved in the cascade of migraine attack initiation as well as sustaining attack activity.
Limitations
The present systematic review revealed the limitations of studies investigating interictal and ictal levels of cytokines in migraine. Consequently, caution is needed in the interpretation of the results. Major limitations involve the heterogeneous study populations and the methodological differences between studies. The studies mainly included migraine patients with or without aura, while few studies included patients with chronic migraine (51,58,60) or menstrual migraine (54). Most studies did not separate migraine patients with aura from those without aura. Controls were defined as either healthy controls, headache/pain free controls (23,40,48) or patients with tension type headache (20,21,36,37,95). Comparison to healthy controls is also important to exclude methodological bias, such as potential procedure-induced local inflammatory responses (66).
Not all studies specified whether migraine patients with known history of other major inflammatory disease were excluded (22–24,28,29,33,36,37,39,40,46,47,55,56). Patients with additional major inflammatory disease might have a different cytokine profile than pure migraine patients.
Many studies did not report the time of the data collection, especially relative to the time of migraine onset in patients. This is important as cytokine levels might alter during the course of an attack.
The sensitivity of the enzyme-linked immunosorbent assay (ELISA) methods, in terms of cytokine detection threshold, varied between studies (21,35,45). Few studies reported undetectable cytokine levels due to low ELISA sensitivity (21,23,33,41,42,55).
Most studies collected blood samples from peripheral veins, while two studies measured the cytokine levels from the internal jugular vein (9,43) and three studies from the cerebrospinal fluid (23,25,52). Unfortunately, we are unable to provide firm conclusion on potential associations between peripheral and central levels of cytokines based on the limited available data on central measurement. Potential limitations include temporal sampling issues and clear separation of ictal and interictal data (23,25,52). Measurement from the internal jugular vein mostly reflects the circulation of the brain parenchyma and is only responsible for <3% of the extracerebral circulation (96). Thus, the internal jugular vein may be more relevant for data collection of brain cytokine levels. Likewise, measurement from the cerebrospinal fluid may provide a profile of cytokine levels within the central components of the trigeminovascular system. However, obtaining samples from the cerebrospinal fluid or internal jugular vein are invasive and infeasible procedures. Consequently, other more feasible methods (e.g. neuroimaging) are needed to assess more central levels of cytokines.
Future perspectives and directions
Future research investigating cytokine levels in migraine should take into consideration the limitations presented in this review. It is necessary to standardize the methodology. This may be achieved by using the same sample source and an optimized method to measure cytokines (e.g., ELISA or radioimmunoassay), which allows detection of low cytokine levels. The study populations should be well-characterized (e.g. phenotype, attack frequency and time from migraine onset) and with separation of migraine patients with aura from patients without aura due to pathophysiological differences (29). It has been proposed that peripheral sensitization by cytokines might be important in migraine chronification (3). Therefore, separation of episodic and chronic migraine may provide information on the impact of attack frequency on cytokine levels (58).
Most studies measured cytokine levels during the ictal or interictal phase. Few studies investigated the levels during the course of an attack while implying possible alterations during the headache phase of migraine (8,9). Longitudinal investigation of the cytokine levels during an attack would be of interest to further elucidate the aspect of potential dynamic ictal cytokine levels. Based on current knowledge, the cytokines IL-1ß, IL-6, IL-10 and TNF-α are of specific interest and should be further investigated.
Investigation of cytokine profiles in the cerebrospinal fluid in future studies is interesting as this may provide relevant information of central processing in the trigeminovascular system. Central investigations would also allow assessment of the potential correlation or differences in the peripheral and central cytokine levels and further elucidate the migraine mechanisms.
Effects of anti-migraine medications (e.g., CGRP antibodies) on the cytokine levels, could be interesting to study in future migraine research. Results from these studies may elucidate the positive feedback-loop between CGRP and cytokines, and thereby the inflammatory aspect of the migraine pathophysiology. Correspondingly, investigations of migraine treatment targeting the cytokines should be explored in future research as well. Interestingly, headache has been reported as a common side effect of treatment with TNF-α and IL-6 inhibitor and monoclonal antibodies (97–100).
It is possible that other peptides than CGRP, such as pituitary adenylate cyclase-activating polypeptide and vasoactive intestinal peptide, stimulate increased level of pro-inflammatory cytokines in migraine (68,101). Moreover, preclinical studies suggest that cytokines are involved in the modulation and activation of e.g., the MAP kinase and COX pathways (85,92,93). These pathways may cover possible mechanisms involved in the sustained inflammatory response and sensitization in migraine patients as mediated by cytokines. Future research is needed to further elucidate the specific role of cytokines in migraine attack pathophysiology.
Conclusion
This review identified that both anti- and pro-inflammatory cytokines were altered in migraine patients outside attacks. Ictal investigations reported unchanged or varying levels of cytokines. These findings suggest persistently altered inflammatory regulation as a potential underlying mechanism of migraine. Future studies with refined methodology are needed to further investigate and expand our knowledge of the role of cytokines in migraine attack pathophysiology.
Clinical implications
Levels of anti- and pro-inflammatory cytokines (TNF-α, IL-6 and IL-10) are altered in migraine patients in the interictal state, suggesting persistently altered inflammatory regulation. Compared to previous studies, we found that interictal IL-10 levels were decreased and IL-1ß levels were unchanged in migraine patients compared to healthy controls. Ictal TNF-α levels were unchanged compared to interictal data in migraine patients, while findings were inconclusive on ictal IL-1ß, IL-6, IL-10 and IL-4 levels. Future migraine studies may focus on investigating TNF-α, IL-1ß, IL-6 and IL-10 levels, based on current knowledge, using refined methodology.
Footnotes
Authors’ contributions
SY and HWS initiated and supervised the study. JT and HMA contributed to the study design. JT and ME carried out the search and screening. JT and SY carried out the data extraction. All authors contributed to interpreting the results. JT wrote the first draft of the manuscript while ME, HMA, HWS and SY contributed significantly with wording and approving the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.