
Abstract
Objective
Telemedicine is defined as video-based consultations with synchronous video and sound. This systematic review investigated the use of telemedicine for headache patients. The primary outcomes of interest were treatment efficacy, feasibility, safety, convenience, compliance, and patient satisfaction.
Methods
A systematic literature search was performed using PubMed and Embase. Thirteen articles met the eligibility criteria and were included in the review. A systematic review protocol was registered on the International Prospective Register of Systematic Reviews, registration number CRD42021265875.
Results
There were no significant differences in treatment efficacy, patient satisfaction, compliance or safety using telemedicine when compared to traditional consultations. Telemedicine was found to be convenient due to being less time-consuming and expensive, especially for patients with limited access to health care. Despite the frequent occurrence of technical errors, telemedicine was found to be feasible.
Conclusion
Telemedicine consultations are similar in quality to traditional in-office headache consultations and can be a more convenient solution for eligible headache patients.
Introduction
Telemedicine has emerged as a common way to provide health consultation services and is now an essential part of digital technologies in the health care sector (1 –3). The use of telemedicine for several neurological subspecialties has previously been investigated (4 –6) and is especially well established for stroke (7,8). The use of telemedicine in headache treatment has been investigated but initially primarily in case studies (9). The use of telemedicine increased during the COVID-19 pandemic and is likely to continue as an integral part of health care, even when pandemic-related restrictions have been suspended (10 –15). There is a mismatch between the high need for optimal headache care and the availability of neurologists (16,17), telemedicine could be an ideal tool to remedy some of the organizational challenges in nonacute headache care and thereby contribute to better patient care (18,19). In this review, we explored current data on telemedicine for headache patients with regard to treatment efficacy, feasibility, safety, convenience, compliance, and patient satisfaction.
Methods
This systematic review was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A systematic review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO), registration number CRD42021265875. Telemedicine was defined as video-based consultations with synchronous video and sound without the patient being physically present. Traditional consultations were defined as in-office consultations where the patient was physically present.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: English peer-reviewed studies in which at least part of the population consisted of headache patients and with separate outcome data on headache patients. There were no specific criteria chosen for the setting and no delimitations in demographic factors such as sex, ethnicity, or age were outlined.
Initially, the search was limited to studies comparing the intervention with a control group participating in traditional consultations. However, this resulted in the inclusion of seven studies, of which six were based on the same trial. Therefore, we also included cohorts without control groups.
Information sources and search strategy
The literature search was conducted using PubMed and Embase. PubMed was searched from 1946 to 13 December 2021, while Embase was searched from 1974 to 13 December 2021.
The search was conducted using a variety of MeSH terms and keywords that were identified through a comprehensive background search. A systematic approach was followed when converting the PubMed search strand to Embase. Complete search strands for both databases are presented in Supplemental Material 1 (PubMed) and Supplemental Material 2 (Embase). All studies were screened by title and abstract in accordance with the eligibility criteria. Articles meeting the eligibility criteria based on title and abstract had their full text assessed. Articles for which it was not possible to determine whether they met the inclusion criteria based on title and abstract had their full text assessed. Articles were assessed according to the same eligibility criteria at the full-text stage as when screened by title and abstract. Articles that met the inclusion criteria when the full text was assessed were included in the review. The reference lists of relevant studies were searched manually to identify additional eligible studies.
Data collection process and data items
The search process and the data extraction were conducted independently by two authors (TCC and NKG). In three cases where authors TCC and NKG disagreed on the inclusion of studies, a supervisor (HWS) was consulted. One of these articles was included in the review, while two were excluded. Data were sought for the following variables in the included studies: title, author(s), year of publication, study design, study period, inclusion criteria, exclusion criteria, country, and total number of subjects with headache included in a study. Moreover, data on headache type, sex, age, health professionals conducting the teleconsultations, setting, and the journal in which the article was published were extracted. Finally, data on telemedicine modality, types of comparison, selected outcomes, and all results assessing variables regarding the use of telemedicine were extracted.
Results
The searches yielded 2047 hits on PubMed and Embase in total. Screening by title and abstract left 92 articles for full-text assessment. All 92 articles were retrieved successfully and screened for eligibility criteria in accordance with PRISMA guidelines. The search resulted in a total of 13 articles being included in the review. Reference lists of the 13 included articles were manually searched to identify additional eligible studies. However, no studies were identified during this process. Figure 1 summarizes the identification of studies in a PRISMA flow diagram.
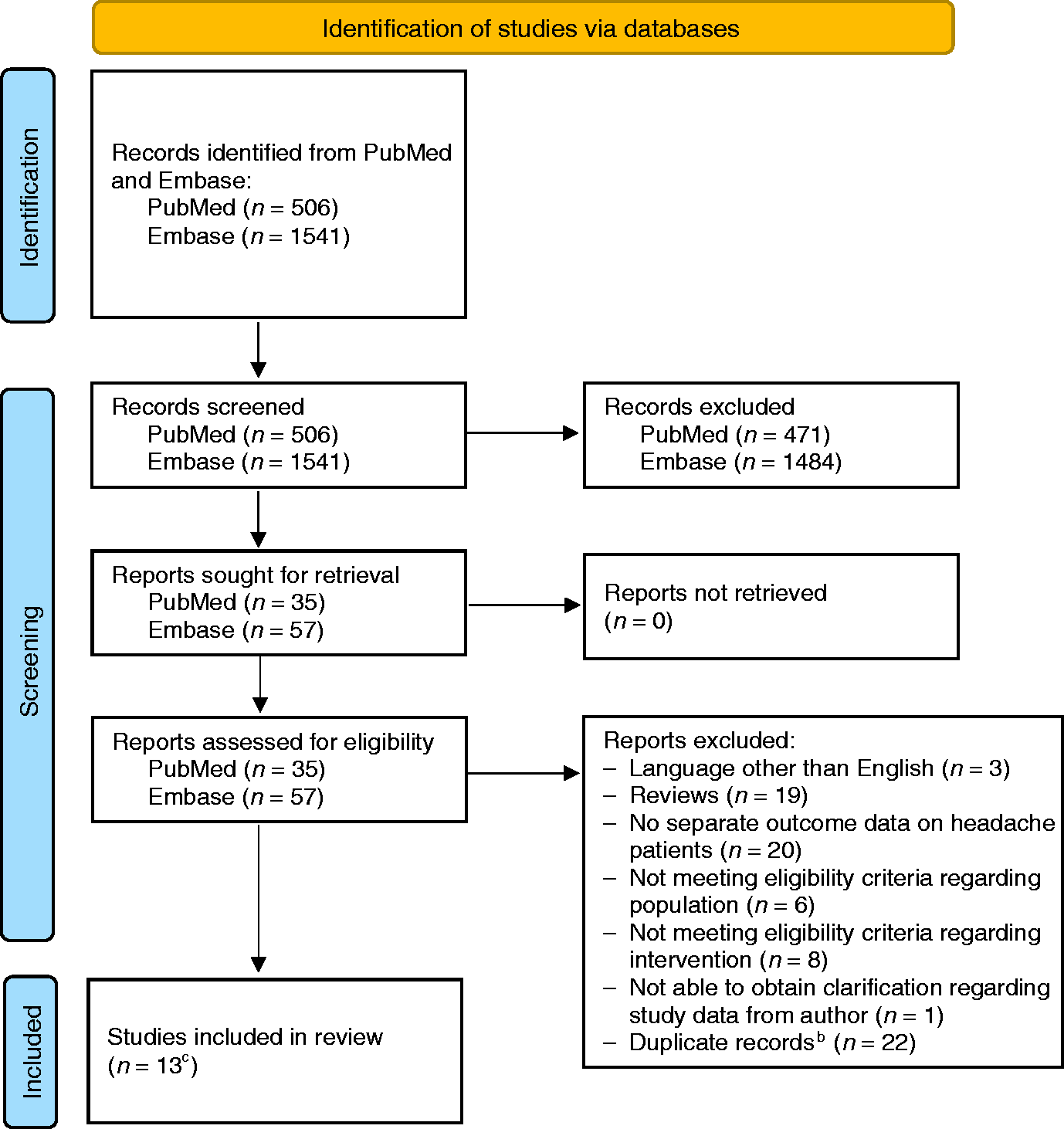
PRISMA flow diagram.a
Study populations and designs
The study populations investigated were heterogeneous. Seven studies (20 –26) included patients diagnosed in accordance with the ICHD-2, while one study (27) included patients diagnosed in accordance with the ICHD-3. Two studies presented specific headache diagnoses for each included patient but did not state whether patients were diagnosed in accordance with the ICHD (28,29). Finally, three studies (30 –32) did not specify the type of headache. One population consisted solely of children (28), while one consisted of both children and adolescents (30).
Only one study (32) investigated the use of telemedicine on hospitalized patients in acute care, while the remaining studies (20 –31) investigated the use of telemedicine in outpatient settings. The initial consultation was via telemedicine in six studies (20 –24,26), while telemedicine was used for follow-up consultations in five studies (25,28 –31). In one study (27), it was not stated whether telemedicine was used for initial consultations or for follow-up.
Seven studies (20 –26) included a control group that had traditional consultations, while one study compared migraine patients to a “non-migraine” group (27). The remaining studies did not include a comparison group (28 –32). Seven studies (20 –26), of which six were based on the same trial, were open-label randomized controlled trials (RCTs). Of the additional studies, one collected data retrospectively (27), and the remaining studies had a prospective design (26,28 –32).
The total number of headache patients in the included studies varied between eight and 402, and the mean age was between 12.4 and 45 years. Finally, the percentage of female headache patients varied between 70.6 and 97.5%. Table 1 presents the study characteristics for all studies included in this review.
Study characteristics of included studies.

aArticles based on the same clinical trial.
bData for the total number for headache patients are not available.
cData only available for headache patients receiving telemedicine.
dData on headache patients are not available.
Abbreviations: MOH: medication overuse headache; TBI: traumatic brain injury; TTH: tension-type headache.
Information and communication technologies
Patients who had telemedicine consultations had to attend the hospital in the six studies based on the same trial (20 –24,26). In one study (32), set in an acute care setting, patients were hospitalized and had telemedicine consultations while in the hospital as well. A “hub-and-spoke” model was used in one study (28), while the additional studies conducted teleconsultations with patients located remotely (24,25,27 –31). In one study (29), teleconsultations were performed by a physician and nurse specializing in headache care, while teleconsultations were conducted by a nurse practitioner alone in another study (28). In additional studies, teleconsultations were carried out by physicians (20 –27,30 –32).
Outcomes
Nine studies (20 –26,28,29) reported on treatment efficacy and headache status using a broad variety of parameters. This included headache days per month, medication use, Migraine Disability Assessment (MIDAS), Headache Impact Test (HIT-6), Visual Analogue Scale (VAS), subjective changes in headache status and remission rate of chronic headache. Feasibility was assessed in eight studies using duration of consultations, number of completed visits, no-show rate, and other factors (24 –26,28 –32). Seven studies (22,23,26 –30) presented data on patient satisfaction, while four studies (24,25,29,30) investigated convenience using telemedicine. Convenience was addressed by investigating travel time, time missed from work, cost of teleconsultations, and other factors. In addition, data on compliance were presented in two studies (21,23), and data on safety were included in one study (21).
Treatment efficacy and headache status
Overall, no differences in treatment efficacy, headache status or remission rate of chronic headache were found in patients who had follow-up teleconsultations in an outpatient setting when compared to patients who had traditional consultations (20 –26,29). One study without a control group found an improvement in headache symptoms similar to outcomes obtained in traditional outpatient visits (28).
One study found an overall higher VAS score in the rural population, which only applied to women when assessed by sex (24). The same study also found that rural patients waited longer to see a neurologist than urban patients (24). “Urban” patients lived in the city where the hospital was located, while “rural” patients lived outside the city where the hospital was located (24). This study used telemedicine for initial outpatient consultations.
Feasibility
Teleconsultations were found to be shorter than traditional visits in outpatient settings (24 –26). This was the case for both initial consultations and follow-up consultations. At the same time, patient perception about the length of visits was similar when comparing the telemedicine group and the traditional group (25). Similar results were reported in an acute setting, where hospitalized patients with headache had relatively short consultations compared to other neurological patients (32).
Friedman et al. (25) found that the number of follow-up consultations completed as scheduled did not differ significantly between the telemedicine group and the traditional group. One study stated that outpatient follow-up teleconsultations had a lower no-show rate and lower late arrival frequency than traditional consultations (30). However, no specific data were presented on this matter.
Rosellini et al. (31) found it possible to obtain a satisfactory neurological examination without the help of a caregiver for all headache patients in outpatient, follow-up teleconsultations. This was not the case for any other group of neurological patients included in the study. However, demands for a satisfactory neurological examination were not specified, and very few headache patients in the study had telemedicine consultations.
One study (29) found that physicians had a low perceived complexity of clinical decisions and that only a small number of patients required in-person re-evaluation (29). The study investigated follow-up teleconsultations in an outpatient setting. Another study (26) looked at a subgroup of patients who had remission from chronic headache 12 months after they took part in either a teleconsultation or a traditional consultation. This study found that patients who took part in traditional consultations more often consulted a general practitioner for headache during a one-year follow-up period (26).
Caponnetto et al. (29) found that headache patients had good computer literacy and that physicians found it easy to interact with patients during teleconsultations (29). Technical failures were, to a certain degree, a challenge in all studies regarding video quality, sound quality, and problems with internet connection.
Patient satisfaction
Studies in outpatient settings using telemedicine for initial consultations and follow-up consultations had similar results. No differences were found in patient satisfaction when comparing telemedicine consultations to traditional consultations (22,23,26). Studies without a comparison group similarly found that patients were highly satisfied with telemedicine consultations (27 –30). In studies with populations consisting of children and adolescents, both patients and their parents expressed a high degree of satisfaction (28,30).
Satisfaction between some subgroups differed in one study where telemedicine was used in an outpatient setting for initial consultations. Thus, women who had telemedicine consultations tended to be more satisfied than women who had traditional consultations (22). One study (22) compared participants in the telemedicine group who preferred traditional consultations to those who preferred telemedicine or were indifferent to consultation type. The group that preferred traditional consultations consisted, to a higher degree, of patients with medication overuse headache (MOH) and patients with ≥15 headache days per month (22). The same study (22) found that patients in the traditional group more frequently preferred traditional consultations over telemedicine consultations. Another study (26) based on the same trial investigated a subgroup of patients who had remission from chronic headache at the one-year follow-up. This study found no difference in satisfaction between patients with remission from chronic headache who had teleconsultations and traditional consultations (26).
Convenience
Telemedicine was found to be more convenient than traditional visits (25,30). Furthermore, telemedicine was found to be both timesaving and advantageous because travel expenses were kept to a minimum (29,30). Rural patients had to travel further to the hospital and had higher travel expenses than urban patients (24).
Compliance
Compliance with treatment for patients receiving care via telemedicine was found to be similar to that of patients receiving traditional care (21,23). This was found in studies investigating telemedicine used for initial consultations in an outpatient setting.
Safety
Safety when using teleconsultations was found to be similar to safety in traditional consultations in a study investigating telemedicine used for initial outpatient consultations (21). Safety was assessed by the presence of secondary headaches within 12 months after a one-time consultation (21). Furthermore, the number of abnormal findings on brain imaging, number of hospitalizations, and other factors were used as outcome measures (21).
Discussion
We identified 13 articles, of which seven were RCTs. As the studies included were few and heterogeneous it is difficult to draw any definitive conclusion based on the present evidence. However, this systematic review suggests that consultations via telemedicine were overall similar to traditional consultations for headache in terms of efficacy, feasibility, safety, convenience and patient satisfaction. Teleconsultations were found to be shorter than traditional consultations and to improve access to health care.
All studies except one investigated the use of telemedicine in an outpatient setting. Based on this review, it is therefore not possible to compare how the setting affects the outcomes stated above. Even though the number of included studies is limited, this review suggests that findings regarding feasibility, treatment efficacy and patient satisfaction are similar when using telemedicine for initial consultations and follow-up consultations.
Telemedicine has the potential to give equity of access to headache care, which is currently an unmet need (33). Overall, better access to health care is an improvement but comes with certain costs balancing over- and underuse. Due to the high prevalence of headache, general practitioners must have adequate clinical skills to treat most headache patients. However, the most difficult to treat patients should be seen by a headache specialist. More widespread use of telemedicine could result in the referral of new patient groups to headache specialists. Making it easier to consult a headache specialist via telemedicine without appropriate patient selection might result in patients being treated by a specialist even when it is not needed. This may inadvertently challenge the principle of treating patients at the lowest possible level of specialization to constrain spending in health care (the LEON principle). This could altogether contribute to an increased and unnecessary workload for headache specialists.
Even though teleconsultations were found to be shorter than traditional visits, there is no indication that the patient’s experience of the consultation was compromised. This is supported by an overall high patient satisfaction when using telemedicine. Teleconsultations might be shorter because they somewhat lack the formal, physical framework that forms part of traditional consultations. Moreover, patients might find a video consultation less suited for talking about subjects not related to their medical issue. This could explain why teleconsultations are shorter, but it also means that teleconsultations might be less suited for talking about personal problems that could affect headache frequency and compliance. These findings suggest that the use of telemedicine could potentially heighten physician productivity. However, telemedicine should not be used uncritically to save time and money, and higher productivity must not compromise the quality of health care. Telemedicine requires thorough training of health care professionals, and the right technology and the value of hands-on clinical examination and face-to-face meetings should not be underestimated.
Clinical outcomes did not differ significantly between patients receiving care via telemedicine and patients receiving traditional care. For this reason, differences in clinical outcomes cannot be considered a confounder for patient satisfaction in this review. Müller et al. (22) found that patients in the traditional group more frequently preferred traditional consultations over telemedicine consultations. The explanation might be that patients in the telemedicine group had more experience and knowledge regarding telemedicine. Patients in the traditional group never tried specialist teleconsultations because participants were randomized before the initial visit. This could potentially cause the assessment of preferred consultation type to be biased. The same study found that patients with MOH and ≥15 headache days per month were less satisfied with teleconsultations. This indicates that patients with certain headache characteristics might be less suitable for telemedicine, but further research is needed.
Technical difficulties were observed in all studies. The prevalence of technical issues depends on the equipment type and whether the patients and doctors are able to use the equipment. Thus, it is not possible to compare technical error outcomes between studies. Especially for patients receiving care via telemedicine at home, technical problems due to user errors or local conditions must be an expected challenge. In the study by Friedman et al. (25), the kind of equipment patients used to attend teleconsultations was not reported. This makes it difficult to compare the technical setup in this study to that of similar studies. In studies by Müller et al. (20 –24,26) and Vierhile et al. (28), the same equipment was used in all consultations. This could potentially be a way to rule out confounding issues caused by the arrangement of technical equipment. However, a study nurse assisted patients who had teleconsultations in the arrangement of technical equipment in the studies by Müller et al. This could mistakenly increase patient satisfaction since patients in this setup might find telemedicine easier to use than patients located remotely who have to take care of the technical setup themselves.
It can be anticipated that the relatively low mean age of headache patients might correlate with having good computer literacy. This is another reason why headache patients might be particularly suitable for telemedicine. It is not possible to rule out that patients with good computer literacy were overrepresented in the included studies. This makes it difficult to conclude the importance of computer literacy based on this review. However, the current age-gap in computer literacy must be expected to be reduced in the near future, and at the same time, software is constantly being improved to become more available and user-friendly. For this reason, it should be expected that age will be an influential barrier to a lesser extent in using telemedicine in the future.
This systematic review demonstrates that telemedicine is particularly advantageous for patients living far away from a hospital. Travel costs and time spent on transportation are exactly some of the challenges that telemedicine could help conquer. The study by Friedman et al. (25) is somewhat ideal to elucidate this problem. Participants in the study received telemedicine care while they were located remotely. For this reason, the higher rating for convenience in the telemedicine group was probably due to patients not having to attend the hospital. Another study design was proposed by Müller et al. (24), where patients in both groups had to attend the hospital. Both studies (24,25) reported similar levels of satisfaction, which shows that the convenience of travelling less might be less important than the satisfaction of being seen by a headache specialist.
Participants in the study by Friedman et al. (25) were offered reimbursements for their travel expenses and parking fees, while Müller et al. (24) stated that a minimum of travel expenses were paid by the patients. Economic differences between patients in these studies are therefore unlikely to have had a confounding effect on convenience. However, differences in reimbursement between studies and different health care systems should be considered a potential confounder.
Compliance was assessed in two studies based on the same trial. Compliance was self-reported in these studies, and no clear definition of compliance was stated, which calls the generalizability of findings regarding this outcome into question. Furthermore, compliance was assessed in questionnaires at three (23) and 12 months (21), which is why the introduction of recall bias was a potential risk. However, the data in these studies were randomized, which minimized the risk of introducing most types of bias.
Several studies in this review assessed the use of telemedicine in follow-up consultations (25,28,30). Patients in these studies were initially seen in person. Participants receiving telemedicine care in the studies by Müller et al. were never seen in person by the headache specialist, and only the referring doctor conducted a neurological examination (21). Performing a thorough neurological examination is a potential challenge when using telemedicine (34). However, studies suggest that neurological examination using telemedicine is at least as good as face-to-face examinations (31,35). The challenge consists in adjusting the neurological examination to adapt to a telemedicine setting and will depend on the clinical condition, the patient's knowledge of their symptoms, and the ability to collaborate effectively. Altogether, this may be even easier in nonacute headache consultations than in consultations for many other neurological disorders (11).
Finding that safety was not compromised in the study by Müller et al. (21) indicates that it is safe to conduct initial consultations using telemedicine in an outpatient setting, but this will require further research. In the study by Müller et al. (21), it was found that patient safety very much depends on the work of the referring doctor. This could lead to headache specialists missing secondary headaches in referred patients. However, given the high prevalence of primary headaches compared to secondary headaches, it is relatively unlikely that a specialist will miss a secondary headache in elective, referred patients. This is even less likely if patients have undergone MRI prior to attending a neurological outpatient department which is the case in some countries. For these reasons, it is unlikely that a neurological examination in a specialist consultation for headache would lead to the identification of secondary headaches that would not have been diagnosed otherwise. Therefore, a neurological examination conducted by a headache specialist is usually of low value even if the referring general practitioner does not perform a thorough physical examination. In a telemedicine setting, a thorough anamnesis for ruling out warning signs, such as the SNNOOP10 list (36), should be a focus instead. In any case, the implementation of telemedicine requires a clear assignment of tasks between the different parts of the health care system. In particular, good communication with primary care facilities and providers, which is already well established in many countries, will be necessary.
Methodological limitations
The main challenge in the present systematic review was the relatively low number of studies meeting the eligibility criteria. Moreover, the included studies were heterogeneous in terms of both population and type of consultation setting and had small sample sizes. The use of the ICHD (37) was not an eligibility criterion in this study. This was done to avoid excluding relevant studies but might have resulted in the inclusion of more heterogeneous studies.
One fundamental challenge associated with investigating telemedicine is that telemedicine is a type of health care delivery. Since telemedicine is part of the framework surrounding headache medicine, it will necessarily be influenced by a variety of parameters. This includes the patient’s and doctor’s attitudes towards teleconsultations and their ability to use the technical devices facilitating such consultations. Even varying conditions such as the subject of a consultation and the way information is communicated will differ largely from one consultation to another. Thus, when conducting studies investigating telemedicine, numerous confounding variables must be considered no matter how homogenous a study population is. This was attempted in the trial by Müller et al. (20 –24). However, this approach makes it difficult to unveil the advantages of telemedicine. For this reason, a study design similar to the one in the study by Friedman et al. (25) should be considered.
The risk of bias in the included studies was only assessed qualitatively, which is a limitation. It was necessary to extend the eligibility criteria to include studies without a comparison group, which also meant including studies with a lower level of evidence. The lack of a control group made it difficult to evaluate causality between a particular outcome and the use of telemedicine. It cannot be ruled out that this might have introduced bias in the search process.
In two of the non-randomized studies, it was stated that patients were able to voluntarily choose to participate in the telemedicine program (28,30). Moreover, patients were excluded from one of the RCTs (25) if they were unwilling to be randomized. This might have caused only patients with particular advantages of teleconsultations and a positive attitude towards telemedicine to be included. Thus, the assessment of patient satisfaction and convenience could be mistakenly high in these studies. The same problem arises in the study that assessed telemedicine use in acute care (32). In this study, the back-up neurologist on call decided whether he wanted to conduct a video consultation. This might have caused the most complex patients to be consulted using video consultations, thereby introducing selection bias.
Implications for future research
The limited number of studies calls for more randomized studies assessing telemedicine in headache care. Ideally, studies investigating telemedicine in a double-blinded, randomized manner should be conducted even though this is challenging. Studies should pursue a realistic design with patients located remotely, either at home or at a “spoke-site”. This will help clarify advantages and disadvantages of telemedicine and evaluate when to use telemedicine in the clinical everyday practice. Moreover, future studies should focus on clinically relevant outcome measures. Specific outcome measures will vary depending on which aspect of telemedicine is investigated. Video-based consultations with synchronous video and sound should be the minimum standard to conduct telemedicine. This setup closely resembles the setting of a traditional consultation and the technology is already widespread.
Conclusion
Telemedicine was found to be a safe and feasible way of delivering health care to headache patients. Treatment efficacy and patient compliance were found to be similar to those of in-person visits, and telemedicine had overall high patient satisfaction. The use of telemedicine for headache patients is timesaving and cost-effective and has the potential to facilitate access to care for many patients, no matter where they live, work or travel. However, telemedicine cannot replace all traditional visits but should be considered an alternative to traditional consultations for selected patients.
Article highlights
Telemedicine is a safe and feasible way of delivering health care to headache patients. Treatment efficacy and patient compliance using telemedicine are similar to those of in-person consultations. Teleconsultations are a convenient alternative to in-person consultations from a patient perspective and have high patient satisfaction. Telemedicine has the potential to increase physician productivity. Telemedicine should not replace all traditional visits but can be considered a valuable alternative for headache patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.