
Abstract
Objectives
We determined headache patients’ satisfaction with telemedicine and assessed how telemedicine influenced headache burden, compliance with diagnosis and treatment, and need for follow-up consultations.
Methods
During 2.5 years, patients from Northern Norway referred with non-acute headaches for a specialist consultation at Tromsø University Hospital were consecutively randomised to either telemedicine or traditional visits. Baseline data were recorded and compared to data from a three-month follow-up questionnaire (see Supplementary material). The following were evaluated: (1) satisfaction with the consultation; (2) headache status; subjective improvement, average pain intensity, treatment, headache days per month, and Headache Impact Test (HIT-6); and (3) treatment compliance and follow-up visits.
Results
Out of 402 consultations, 348 (86.6%) answered the questionnaire. Satisfaction was similar in the telemedicine and the traditional group (88.8% vs. 92.3%; p = 0.35). Subgroup analyses were not prespecified, but there were no differences in satisfaction among females, migraineurs, rural patients and urban patients. Improvement from baseline after three months was reported equally in the telemedicine and the traditional groups. There were also no differences in treatment compliance, but rural telemedicine patients had less-frequent headache visits at three months’ follow-up (28.9% vs. 48.7%, p = 0.002).
Conclusion
Telemedicine is non-inferior to traditional consultations in patient satisfaction, specialist evaluation, and treatment of non-acute headaches. ClinicalTrials.gov ID: NCT02270177.
Introduction
Epidemiological data show that around half of the world’s adult population report having an active (during the last year) headache condition fulfilling the criteria for tension-type headache (42%), migraine (11%) and chronic daily headaches (3%) (1). The headache population of Northern Norway is spread over a large geographical area with challenging weather conditions, making travelling and access to specialist health care cumbersome. This may contribute to suboptimal treatments of primary headaches (2–4).
Telemedicine provides an information and communication technology that is independent of geography and weather conditions and has the potential to increase access to specialist care. However, implementation of new information and communication technologies is often based on politics and ideology rather than evidence and rationality and often without performing a prior consequence and economic analysis (5–7).
Although European guidelines for second opinion teleheadache consultations exist, the evidence is only case based (8–10). Randomised studies are thus required (11). We performed an open-labelled, non-inferiority trial to compare telemedicine with traditional headache specialist consultations. The primary hypothesis was that headache patients’ satisfaction and specialist management of non-acute headaches with telemedicine is non-inferior to traditional specialist consultations.
Methods
Study design and patients
From 30 September 2012 until 30 March 2015, we consecutively screened all referrals of non-acute headache patients from Northern Norway to the Department of Neurology at the University Hospital of Tromsø. Patients who fulfilled the following criteria were invited to participate in the study:
Norwegian-speaking females and males ≥ 16 and ≤ 65 years of age; referred to a neurologist for headache diagnostic clarification and/or treatment; lack of symptoms and abnormal findings on either clinical neurological examinations reported by the referring doctor or by brain imaging, suggestive of a secondary cause; and wait time ≤ 4 months from the date of the referral letter.
Patients who had been evaluated by a neurologist for headaches within a two-year period prior to referral were excluded to hinder potential benefits of including those who were already headache-specialist evaluated.
Interventions and equipment
All consultations took place in the Department of Neurology at the University Hospital of North Norway in Tromsø. Telemedicine consultations were performed with the following videoconference system: Cisco C40 Integrator Package, Cisco C40 Integrator Multisite, Cisco Precision HD 1080p 12xcamera, an NEC X551s 55-inch light-emitting diode (LED) monitor, Audio-Technica ceiling microphones and JBL LSR2325P active speakers, Integrator Package C40 Dual Display option and a Cisco Touch-Control Device for C Series. This equipment is installed in one office. The neurologist consulted the patients from two other offices via a Cisco EX60 unit with an InTouch panel. There was only virtual contact between the patients who used telemedicine and the consultants. Traditional consultations took place in one of the offices where the Cisco EX60 is installed.
All consultations were conducted by two experienced neurologists (KIM and SIB). Patients from both groups underwent standardised, structured, and thorough anamnesis via the use of an administrative protocol. Diagnoses were made according to the 2004 criteria of the International Classification of Headache Disorders, second edition (IDHD-2) (12). Additionally, we used ICHD-2 and established red flag criteria to rule out structural causes (secondary headaches) (12–14). These criteria were also used as a checklist during the interviews with the patients. Neurological examination was not performed at the specialist consultations. Moreover, treatment prescriptions were given to the patients in the telemedicine group by a study nurse. Consultation fees were not charged.
Participants received a questionnaire three months after the headache consultation to assess the outcomes. According to patient preference, three-month questionnaires were sent either by an online survey service (Questback) or by ordinary letter mail (15). A reminder was sent out if patients failed to answer the questionnaire within two weeks. A 12-month follow-up is being planned.
Questionnaire
A three-month, 28-item structured questionnaire was designed to evaluate patients’ opinions of the specialist consultation and to describe their current headache burdens.
The patients were asked:
If they were ‘satisfied with the consultation’ three months earlier (‘Yes’ or ‘No, why not?’). For the subjective change in headache frequency and intensity: Is the headache better, unchanged, or worse? Is the headache frequency reduced, unchanged, or increased? Is the headache intensity reduced, unchanged, or increased? To fill in the number of headache days and headache attacks per month. For the intensity of headache measured on a standard visual analogue scale (VAS, 0 being ‘no headache’ and 10 being ‘worst possible headache’). To complete the Headache Impact Test (HIT-6) to assess impact of headache in daily life (16). For other lifestyle parameters including employment, sick-leave, and other allowances. For use of medications, including frequency of painkillers and triptans. For recall of headache diagnosis, compliance with treatment, number of general practitioner (GP) visits, and number of GP visits due to headache within three months after consultation.
Outcome variables
Frequency of satisfied patients at three months. Change from baseline in number of headache days per month at three months. Changes in VAS from baseline at three months. Changes from baseline in HIT-6 at three months. Frequency of patients that remembered the headache diagnosis correctly at three months. Patient’s compliance with treatment that was initiated at the consultation at three months. Frequency of patients that visited GP due to headaches within three months after the specialist consultation. Number of GP visits due to headaches within three months after specialist consultation.
Sample size
Sample size was calculated for the three-month follow-up satisfactory binary outcome. We chose satisfaction as the first outcome because it is the first and most important dimension to assess in the research of telemedicine impact. Without headache patients being satisfied with telemedicine, implementation of such information and communication technology would be very difficult, short lived, and unsuccessful in clinical practice. Based on a previous study, only half of the headache patients in Northern Norway would be satisfied with their specialist consultation (17). However, patient satisfaction with telemedicine in international studies has been reported as being above 90% (18), and a non-prespecified interim analysis of the first 40 individuals in the present study, regardless of group allocation, showed a satisfaction of 92.5%. Based on this figure, we decided to recalculate the original sample size by setting the satisfaction to 90% in both groups. Considering a non-inferiority margin of 10% as being strict and 20% as being liberal, and the advantages of telemedicine (e.g. elimination of unnecessary travelling, reduction of direct and indirect costs, and increased access to care especially in rural areas), we chose a non-inferiority limit of 15% or greater between the groups as clinically relevant (19). Using a significance level of 0.01 of a two-sided 98% confidence interval, sample sizes of 127 participants in each group are required to achieve a power of 95% to demonstrate a non-inferiority limit of 15% (20). Considering responder and dropout rates, the number of participants needed to include was estimated to be 400.
Randomisation
A study nurse at the Department of Neurology randomised patients just before the consultation. Randomisation to either telemedicine or traditional consultation was made through a centralised telephone line to the randomisation office in the Research Department at the University Hospital. All patients were block randomised with randomly selected block sizes by using a developed application with an (Rnd) function in the computer program, Microsoft Access (21).
Statistical methods
We analysed the data with the computer program SPSS version 21. Continuous variables were tested for normality with Shapiro-Wilk’s test, skewness, and kurtosis. Additionally, histograms, Q-Q plots, and box plots were visually inspected. The Mann–Whitney U test and independent samples T test had coinciding conclusions for non-normally distributed variables. For consistency, we presented them as mean with standard deviation (SD). Normally distributed variables were analysed with independent sample T tests and chi-squares and were presented as mean with SD and numbers with percentages, respectively. Yates continuity correction was used for 2 × 2 tables. All tests are two-sided, and statistical significance is defined as p < 0.05. Meanwhile, all subgroup analyses are from non-prespecified comparisons. We made intention-to-treat (ITT) analyses by using last observations carried forward (LOCF) from baseline for continuous variables, and chi-square cross-tabulation with missing values for categorical variables. The seven patients who were excluded after randomisation due to not having fulfilled the eligibility criteria were not included in the ITT analyses (Figure 1).
Flow chart over patients. ITT: intention-to-treat.
Consent, registration and ethical approval
We obtained informed oral and written consent from all participants before data collection began. The study was approved by the Norwegian National Committee for Medical and Health Research Ethics (REC), number 2009/1430/REK, and conforms to the Helsinki Declaration (22). The trial is registered at the Norwegian Research and Management database (FAS, ID3897/HST959-10) and at ClinicalTrials.gov (ID. NCT02270177). Our trial was planned in 2008. Initially, it started in a small rural hospital in Northern Norway in 2009, but it was reorganised due to in-hospital difficulties. We did not regard a health-service study on consultations as being an intervention within the registration requirements according to the International Committee of Medical Journal Editors (ICMJE)’s definition in 2008, and it was therefore registered retrospectively (23). As shown by the FAS registry, this has not resulted in any changes or omissions of planned outcomes (24).
Results
Demographics and clinical characteristics of the randomised groups in patients referred to specialist for headaches.

p = 0.03 of those answering three-month questionnaire. All other comparisons are non-significant. BMI: body mass index; TTH:tension-type headache; MOH:medication-overuse headache; HIT-6: Headache Impact Test-6; VAS: visual analogue scale.
First three columns correspond to all patients. Last three columns correspond to those that answered the three-month questionnaire.
Headache sufferers in the telemedicine group did not differ in demographics and clinical characteristics from the traditional group. Neither did the 402 consulted patients, 101 men (age 40.6, SD 13.7), and 301 women (age 35.8, SD 13.1) differ significantly from individuals not included (n = 155) in gender and age (p = 0.17 and 0.41, respectively). Female participants were younger than the males (p = 0.001) and had slightly more extensive education than the males (p = 0.022). Additionally, females had higher VAS and HIT-6 scores at baseline (p = 0.007 and 0.032, respectively). Females who answered the three-month questionnaire were still five years younger and had more years of education than male respondents (p = 0.001 and 0.022, respectively). After three months, VAS and HIT-6 scores were not statistically different in females as compared to men (0.5 and 1.1; p = 0.15 and 0.26, respectively).
Per-protocol satisfaction comparisons of telemedicine and traditional headache specialist consultations at three months.

Prespecified per-protocol analysis.
Non-prespecified per-protocol subgroup analysis.
Living in Tromsø City.
Living outside Tromsø City.
MOH: medication-overuse headache.
All per-protocol comparisons are non-significant. All intention-to-treat comparisons are non-significant.
Intention-to-treat satisfaction comparison of telemedicine and traditional headache specialist consultations at three months a .
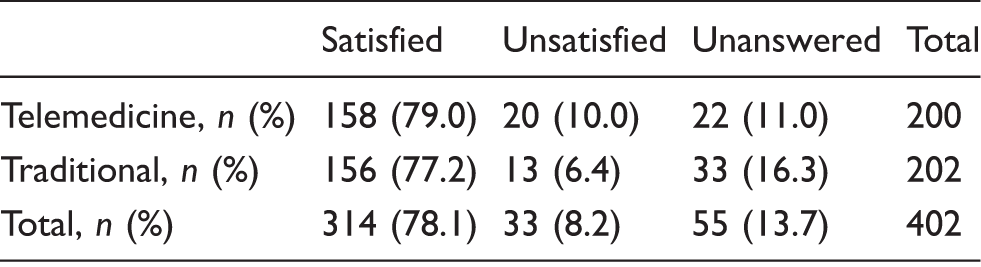
Pre-specified. Pearson Chi-Square 3.7, p = 0.16.
Per-protocol comparisons of treatment efficiency within telemedicine and traditional headache specialist consultation a .

Intention-to-treat analysis showed that more patients visited their general practitioners (GP) in the traditional group (p = 0.041). The other per-protocol and intention-to-treat analyses were not statistically significant.
Baseline data.
The difference between three-month follow-up and baseline data.
HIT-6: Headache Impact Test-6; VAS: visual analogue scale; GP: general practitioner.
Per-protocol comparison between telemedicine and traditional consultation of rurala headache patients’ GP visits at three months after the headache specialist consultationb,c.

Those living outside Tromsø.
Non-prespecified data.
Intention-to-treat analysis showed trends towards significance, p = 0.07, 0.051 and 0.05. The other intention-to-treat comparisons were significant.
Those living ≥ 25 km outside Tromsø
Those living ≥ 40 min outside Tromsø.
GP: general practitioner; min: minutes.

Those living in Tromsø
Non-prespecified data. Intention-to-treat analysis did not show statistical significance.
Those living < 25 km outside Tromsø.
Those living < 40 min outside Tromsø.
GP: general practitioner; min: minutes.
Discussion
In general, the majority of patients with non-acute headaches who were allocated to telemedicine reported satisfaction (88.8%), and this figure is in agreement with other international studies (18,25,26). These patients were not less satisfied than those who were allocated to traditional consultation. Comparisons of headache status, treatment and compliance in these two groups three months after the consultation did not show any inferiority of telemedicine compared to traditional consultations. Although satisfaction rates are often reported to be higher in telemedicine than in traditional consultations, different education and equipment as well as use of different methodologies require cautious interpretations of most telemedicine studies (25,27,28). Among 495 telemedicine consultations from different specialties in South Carolina, United States (US), 98% were satisfied overall with telemedicine, and only 21 (4%) reported a preference for a traditional consultation (18). The authors speculate that confounders such as less travel and waiting time, easier arrangements, and consultations in the patients’ local areas may explain the high satisfaction rates in their own and other telemedicine studies (18).
A systematic Cochrane review identified overall positive satisfaction among eight studies with 371 children and adolescents altogether younger than 18 with chronic and recurrent pain (75% with headaches) who underwent psychological therapy through different remote technologies (29). However, this review analysed the data qualitatively and did not give specific satisfaction numbers (29). Of 354 US veterans with neurological disorders (13% headache), 90% reported satisfaction with follow-up visits through telemedicine (26).
In contrast to other studies, our design made telemedicine technology the only difference between the intervention and control group. By using the same location, the same personnel, and the same protocol in both groups, we removed the effects of travel, location, arrangement and waiting time as potential confounders. Moreover, randomisation rendered baseline characteristics in both groups similar and promoted internal validity. Yet the number of satisfied patients was high and similar in both groups.
Overall, our study showed much higher satisfaction among headache patients than previously reported in the literature (27). On one hand, the overall high satisfaction in our study might be explained by the highly standardised consultations and the fact that consultations were made exclusively by headache specialists. However, including patients in a study might bias the results.
In our study, we consecutively recruited from a general neurological outpatient clinic during a 2.5-year period, mirroring a daily outpatient practice. A relatively large number of participants, high rate of inclusion, and a three-month responder rate of 86.6% strengthen the external validity further.
On the other hand, telemedicine consultations inside the hospital may have given patients a false sense of security and possibly made the study less realistic.
Telemedicine has many benefits for headache patients that include improved access to specialist care, less geographic disparity, and avoidance of travel (30). However, traditionalists would argue that such technology would disrupt the doctor-patient relationship and weaken local health care in rural areas. Other barriers are reluctance to adopt new technology in clinical practice, expensive technology, liability concerns, and difficulties in performing proper neurological examinations through telemedicine (30).
An effect of telemedicine in our study was that it led to redistribution of the neurologic examination from the neurologist to the GP. Others have shown that information and communication technologies, and in particular telemedicine, often lead to modification and redistribution of clinical tasks among health care personnel (30,31).
An unexpected finding was that patients from rural areas who underwent telemedicine had fewer GP follow-ups due to suffering headaches after three months than those who had traditional visits (Table 5). We speculate that employing telemedicine may have a trivial effect on non-acute headaches but could not find such a difference in urban patients (Table 6). Although this finding was consistent over different variables, multiple univariate analyses were conducted without adjustment, making it likely that some significant results are due to chance. Nonetheless, our findings indicate that a realignment of tasks may occur, possibly strengthening the centralised specialist health care centre at the expense of local follow-up routines. Further follow-up studies are warranted to evaluate the long-term results of these and other realignments caused by telemedicine technology.
The far-reaching changes in computer-supported cooperative work throughout time have made our society globally digitalised. Today, we have access to advanced information and communication technology in almost every place, at any time, in every city, and in remote areas. In the US, the Veterans Health Administration has provided care to more than one million people through telemedicine in 2012, but due to legislations and political priorities, there are great disparities in telemedicine practices among different states (26,32).
Despite headache being among the most common ailments in humans, a lack of studies exists that addresses satisfaction, burden, management, and safety issues of handling newly referred non-acute headaches through information and communication technologies. In PubMed, we identified only two case series in primary diagnoses of non-acute headaches with telemedicine (9,10). From October 2006 to December 2010, telemedicine consultations from a US military program retrospectively identified 265 headache consultations (115 migraines) (33). The most common recommendations to patients were work-up and therapeutic suggestions, and medications were recommended for 46% of patients. In our study, 82% were recommended medication, but the patients in the US military are composed of 86% males and do not mirror a general headache population.
In conclusion, recognising a high need for specialist headache care and the lack of evidence for proper diagnostics and treatment of non-acute headaches via telemedicine, we conducted a randomised study to compare telemedicine with traditional consultations. We found that satisfaction with telemedicine was high and non-inferior to traditional visits. Our study ultimately provides evidence that telemedicine is a well-suited technology for diagnosing and treating non-acute headaches, but safety should be assessed via a longer follow-up period.
Article highlights
Nine out of 10 patients with non-acute headaches are satisfied with telemedicine consultations. Telemedicine is a well-suited information and communication technology for diagnosing and treating non-acute headaches and is not inferior to traditional consultations. Telemedicine causes realignment of headache health-care structure and clinical tasks, but the long-term results of these changes are yet to be investigated.
Footnotes
Acknowledgements
We would like to thank Jorun Willumsen, Anna-Kirsti Kvitnes, Marlen Lauritzen, Nora Bekkelund, Karin Flatekval Eines, Torill Erdahl, Marianne Røst and Grethe Berg Johnsen in the Department of Neurology in Tromsø for helping us to collect and organise the project data. We also thank Bjørn Straume in the Research Department for statistical advices.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Northern Norway Regional Health Authority (Helse Nord RHF).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.