
Abstract
Objective
Migraine is a common disorder affecting more than 10% of the population. The prevalence of migraine among physicians and, in particular, among headache specialists is widely unknown as is the impact of suffering from migraine on the attitudes towards migraine and on treatment recommendations of physicians. We designed a survey among headache specialists and neurologists and compared the results to general pain specialists and general practitioners.
Methods
A standardized interview in randomly selected samples of these four groups of physicians was performed. The interview included data on the prevalence of migraine and other primary headache disorders in the physician groups, self-report on their own treatment, attitudes towards migraine, and treatment recommendations for migraine. The prevalence rates were also compared to an age- and sex-matched German general population sample.
Results
The lifetime prevalence of migraine was higher in headache specialists (53.0%) than in general neurologists (43.0%), pain specialists (21.7%), general practitioners (19.3%), and in the general age- and sex-matched population (16.8%). Cluster headache prevalence was high in neurologists (1.9%) and in headache specialists (1.3%); episodic tension-type headache prevalence was significantly lower in general practitioners (19.5%). One reason, among others, was that being a migraine (or cluster headache) patient more often prompted the sufferers to become a specialist in neurology. Physicians with migraine rated the biopsychosocial concept of lower importance for migraine than did physicians without migraine. The self-treatment of migraine in physicians differs from the treatment recommendations to the patients. For example, only 36.4% of the headache specialists with migraine take triptans whereas 94.4% recommend triptans to their patients.
Conclusions
We conclude that being a headache specialist or a neurologist is associated with an increased migraine or cluster headache prevalence. This personal history of migraine leads to a more somatic view of migraine as a disorder and to different treatment recommendations as compared to self-treatment.
Introduction
Migraine is one of the most common neurological disorders worldwide and a lot of epidemiological studies have been published on the prevalence and on the burden of migraine and other headaches (1). However, the epidemiology of migraine and headache among physicians and particularly among neurologists and headache specialists is unknown in detail.
There are some studies on the prevalence of migraine in neurologists and other physicians. In one study in the US (2), the 1-year prevalence of migraine in male headache specialists was 59.3% and in male neurologists 34.7%; in the male general population of the USA, however, it was about 6% (3,4); a similar study was published later, again from the US (5). A study from Taiwan assessed the practice patterns of migraine management in neurologists who are suffering from migraine themselves (6). The prevalence of migraine in neurologists (27.6%) was higher than in the general population (14.4% in females and 4.5% in males). For other countries, there are small observational studies available from the United Kingdom (7), from Italy (8), from Canada (9), from Spain (10), from France (11), from Norway (12), from Portugal (13), and from Australia (14). These studies are mainly in line with the results of the American studies showing a prevalence of migraine in neurologists of about 40%. In the United Kingdom, however, the migraine prevalence among general practitioners was found to be not different from the general population (7).
All these studies suggest that migraine is much more prevalent among headache specialists and neurologists than in the general population, but conflicting results were obtained for general practitioners. However, the impact of suffering from migraine on treatment decisions and on attitudes towards migraine as a disorder has not been studied in detail. We therefore investigated the prevalence of migraine and other primary headache disorders in headache specialists, pain specialists, neurologists, and general practitioners in Germany and compared these data to the general German population. Further, we analysed the attitudes towards migraine with respect to suffering from migraine or not. We analysed the self-treatment of physicians with migraine and compared these data with the treatment recommended to their patients with migraine; we also tried to get insights into why the migraine prevalence is so exceptionally high among neurologists and headache specialists.
Thus, migraine can be a model disorder for physicians who are suffering from a disease or disorder themselves and who are specialised in their own disorder or disease. It might be that the self-affliction has a strong impact on treatment decisions and recommendations and on advising patients on their disorder or disease.
Methods
We contacted actively practising physicians for enrolment into this study (n = 1800). All physicians were randomly selected from the membership lists of different scientific societies or boards. The regional distribution in Germany, according to 10 postal regions, was considered when selecting the physicians. The physicians were separated according to four groups:
The first group was recruited from the membership list of the German Migraine and Headache Society (DMKG), labelling themselves as headache specialists. They received the survey by mail with self-addressed and stamped return envelopes. In addition, physicians attending the German Pain Congress (see ii) and labelling themselves as headache specialists were also included. In total, 300 headache specialists were contacted. Physicians attending the German Pain Congress and who were members of the German Pain Society (DSG; formerly German Society for the Study of Pain, DGSS), labelling themselves as pain specialists but not as specific headache specialists; 500 attendees received the survey while visiting several lectures and were asked to return the completed survey to the reception of the congress. This was done at two different congresses. Members of the German Neurological Society (DGN) with a Board certificate in Neurology, explicitly labelling themselves as no headache and no pain specialists. Five hundred physicians chosen from the membership list of the society received the survey by mail with self-addressed and stamped return envelopes. Members of the German Association of General Practitioners (BVA) without a specific interest in pain therapy and without a Board certificate as a pain specialist. Addresses were sourced from the mailing list of the association, and the survey was likewise sent by mail with self-addressed and stamped return envelopes to 500 members.
The survey questions asked for demographical data (age, sex, years in practice) and for self-reporting of headaches, in particular migraine (asked for as the lifetime prevalence). In addition, we asked for attitudes towards migraine, for treatment of their own migraine (if applicable), and for treatment recommendations to migraine patients. All groups received the same questionnaire.
The survey was completed by 63.2% of all physicians (n = 1137). All questionnaires could be included in the statistical analysis, since all answered the question for headache and since missing data were otherwise rare and only of minor importance. For self-reporting of headaches, we asked for the following headache types according to the criteria of the International Headache Society (IHS) from 2004 or 2013 (15,16): Migraine without aura; migraine with aura; chronic migraine; sporadic and frequent episodic tension-type headache (ETTH); chronic tension-type headache (CTTH); cluster headache; other headache types to be specified. The IHS criteria were provided to those physicians not familiar with them. We also collected data on headache frequency and severity.
Questions dealing with attitudes towards migraine were answered on a six-grade rating scale from “1 = completely agree” to “6 = completely disagree”. Furthermore, they could select “no opinion”. We also asked for the impact of suffering from headache on the decision to study medicine and to become a neurologist, a pain, or a headache specialist. Treatment recommendations to the patients and the self-treatment of physicians with migraine (if applicable) were asked for by answering yes or no to given choices of acute drug treatment, of prophylactic drug treatment, and of complementary treatment such as acupuncture or homeopathy.
We compared the prevalence rates to an age- and sex-matched sample extracted from the German general population (the so-called German DMKG Headache Study, Dortmund region). The data of this study have been published previously (17).
Descriptive and analytical statistics were performed with the Statistical Products for the Social Sciences (SPSS) for Windows, Version 13.0 (SPSS Inc, Chicago, IL, USA). Data are presented as arithmetic mean with simple standard deviation or as percentage. We applied non-parametric testing (Mann-Whitney-U-test, Kruskal-Wallis analysis, χ2 test) and used Bonferroni correction for multiple testing. Significance level was set at p = 0.05.
Results
Demographic characteristics of the different study groups. Statistical analysis by Kruskal-Wallis test or χ2 test (for post-hoc analysis see text).

Related to the subgroup of physicians with migraine.
Not applicable.
Migraine and other primary headache lifetime prevalence rates and migraine data in the different study groups. Statistical analysis by Kruskal-Wallis-test or X2 test (for post-hoc analysis, see text).
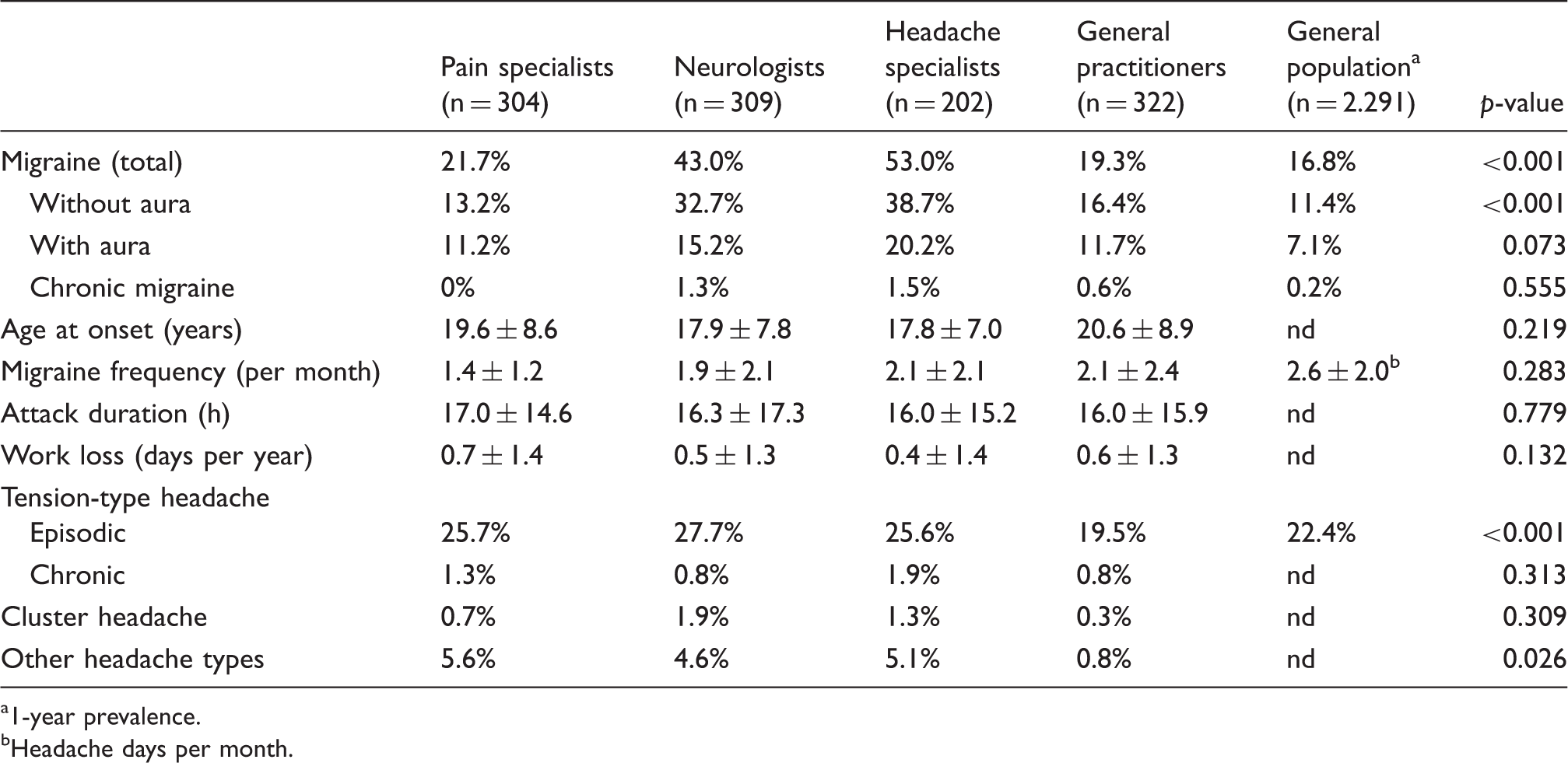
1-year prevalence.
Headache days per month.
Attitudes towards given statements on migraine among physicians with and without migraine given as arithmetic mean with standard deviation (scale from “1 = totally agree” to “6 = totally disagree”). Statistical analysis by Mann-Whitney U-test.

Denotes that the p-value remains significant after Bonferroni correction.
Percentage of physicians recommending different acute and prophylactic drugs or other treatments in migraine therapy. Data are given separately for those physicians with and without migraine. Statistical analysis by X2-test.

including ASA, paracetamol etc.
denotes that the p value remains significant after Bonferroni correction.
Comparison of self-intake and treatment recommendations in physicians with migraine (in %).

including ASA, paracetamol etc.
Discussion
Prevalence of headache disorders
Our main finding is that the lifetime prevalence of migraine in headache specialists and neurologists is much higher than in the general population and in the other two physician subgroups (pain specialists and general practitioners). We were able to individually match our data to the data of an epidemiological study performed in Germany (17); however, this was a historical sample and not recruited specifically for this study. Other German epidemiological studies on the lifetime prevalence of migraine have shown figures of 11% (18) and 16.6% (19) for all age groups and are thus comparable to our findings for the general population and general practitioners. The prevalence of migraine without aura and migraine with aura (note: double diagnosis was allowed) showed the expected ratio for all professional subgroups and was thus also comparable to the general population. The prevalence of chronic migraine seems to be higher in headache specialists and in neurologists compared to the general population and to the other subgroups. However, these differences were not statistically significant and are still in the range of worldwide (20) and national (21,22) prevalence data on chronic migraine.
Also, the prevalence of cluster headache among the three specialised physician groups (between 0.7% and 1.9%) is higher than in the general German population, which has been shown to be 0.15% in two independent studies (23,24) and higher than the prevalence of cluster headache worldwide with 0.12% (25). Since we were not able to match our participants to a sample large enough for statistical comparison, we have no direct comparison with the general population. The prevalence of episodic (but not of chronic) tension-type headache was higher among the specific physician subgroups compared to general practitioners but not to the general population in Germany. Since the differences are rather small (although significant) we regard these as unspecific and not very relevant. It might be that the workload or the behaviour at work is so different compared to general practitioners that it increases the risk for ETTH. It is remarkable that the prevalence of CTTH, in about 1.0% of all physicians, exactly matches the prevalence of this disorder in the general German population (17,18). Finally, we observed considerably and significantly higher prevalence rates for other headache disorders in the specialized physician subgroups compared to general practitioners. It might be that this is just a reporting bias. When classifying these headache disorders in detail, the majority of other headache types among the specialists were headache types from chapter 4 of the International Classification of Headache Disorders (ICHD) edition 2 (in particular, headache associated with sexual activity and idiopathic stabbing headache), which might not be regarded as a headache disorder by general practitioners.
Migraine prevalence (all types of migraine) among different physician subgroups worldwide (percentage).

1-year prevalence.
Lifetime prevalence.
General practitioners.
Only hospital doctors, bias likely.
Bias likely (response only if physicians or relatives had migraine).
All physicians together. Note. nd: no data.
The reason for these high prevalence rates among neurologists and headache specialists could not be determined definitely by our study. Several factors might be responsible for this phenomenon. We believe that there is a multifactorial background behind this observation: a) Participation bias; b) self-diagnosis; c) motivation to become a specialist; d) impact of work on migraine; e) impact of being a migraine patient on working pattern.
Participation bias might have contributed to the high rates of self-reported migraine, since self-affliction might lead to the wish to participate in such surveys because one is interested in the results and supports public interest. However, as the rates of participation were considerably high for a survey among physicians, this bias is probably of minor importance. A similar bias factor might be that attending a pain congress and/or being a member of a scientific society may lead to a selection of physicians who are affected themselves by a (neurological) pain disorder. However, studies with different selection criteria yielded similar results.
Further, we relied on the self diagnosis of all physician groups. Neurologists and headache specialists might have better knowledge in diagnosing their own symptoms and in remembering previous migraine attacks and classifying their symptoms according to the ICHD, so they would report their own migraine more frequently. This is in particular true for isolated migraine auras, which occur predominantly in men over the age of 40. It also might be that, although we provided the ICHD criteria for migraine, some of the physicians apart from neurologists regarded other headaches as a migraine or did not identify migraine.
We could detect one reason for a higher rate of migraine among neurologists and headache specialists in our sample. This is that some of the physicians decided to become a specialized neurologist or headache specialist also because of their own headache. In headache specialists, 23.5% of the migraine patients among them said that their own migraine was one factor, among others, in becoming a headache specialist. In particular, those physicians suffering from cluster headache were influenced by their headache. All but two (one of them with cluster headache starting after becoming a physician) stated that their own suffering from cluster headache was one reason to become a neurologist or pain/headache specialist. It is likely that suffering from this chronic neurological condition leads to the wish to learn more about such a disorder and to learn more about treatment strategies and to be one of the first to have access to new treatment options.
Another factor contributing to this high prevalence of migraine in physicians might be that this profession is in general a stressful job and thus triggers more migraine attacks. Irregular time schedules during work, being on shift or on call, or working on weekends are influencing biorhythmicity and could induce more and/or more severe migraine attacks so that the sufferers are more aware of their disorder. Working as a surgeon is also hardly acceptable for a doctor with a high frequency of migraine attacks. On the other side, working as a neurologist, at least in previous decades, is more plannable and controllable than in other specializations; in this context it might be interesting to know whether the migraine prevalence is also increased among psychiatrists, but we are not aware of any respective data. This all together might lead at least to a higher 1-year prevalence, maybe also to a higher lifetime prevalence of migraine.
Finally, one reason for the high prevalence of migraine among neurologists and headache specialists could be that migraine is associated with a specific cognitive processing (27) that could be more useful for being a neurologist (nearly all headache specialists have neurology as their primary specialisation) than for having a different specialization. The characteristics of migraine patients, who are said to be more accurate or even obsessive, to be more analytical, and to be more sensitive for repetitive cognitive stimulation (28,27), might be better compatible with neurology than with another medical subspecialty. However, the discussion of whether or not migraine predisposes for a specific cognitive processing and behaviour in daily and working life is scientifically still under debate (29).
With respect to the migraine features, physicians do not differ from the typical clinical features of the general population. The time pattern (age at onset, attack frequency, attack duration, time of work loss) are on average about the same as in the general German population (18). This could be another argument that the predisposition for migraine itself (and not the clinical manifestation of migraine) is associated with being a neurologist or headache specialist. The mean time of work loss in one year caused by migraine was less than one day in all groups, which is about the average work loss by migraine in the general German population (18) and nearly exactly the same work loss as was described for physicians with migraine in the United Kingdom (30).
Attitudes towards migraine
Beside the evaluation of prevalence rates, one main goal of this study was to compare the attitudes towards migraine between physicians with migraine and those without migraine. Therefore, we developed a questionnaire with several statements on the pathogenetic concept of migraine and on different treatment procedures. In summary, the results of this questionnaire suggest that physicians with migraine have a more somatic concept of the migraine etiology and more deny psychological factors contributing to migraine. For instance, the biopsychosocial concept, which is nowadays accepted for all chronic pain disorders, is of significantly less importance for physicians with migraine compared to their colleagues without migraine. On the other hand, the importance of diagnostic procedures such as EEG or brain imaging in migraine is lower in physicians with migraine because they know that these procedures are not needed for the diagnosis and are always normal in migraine. Physicians with migraine significantly more strongly support the importance of trigger factors in the etiology of a migraine attack and in migraine treatment. Further, physicians with migraine nearly completely agree to involve their migraine patients actively in the treatment concept. They are more in concordance with the current treatment guidelines of migraine (31) such as NSAIDs as drugs of first choice, endurance sport, and the importance of prevention than the other subgroups. Both groups strongly disagree with both the statement that migraine is a genetically determined disease and the statement that migraine is a psychosomatic disorder. This could be seen as a contradiction but is more likely a result of the nature of migraine, which cannot be explained in all its aspects by genes alone or by psychosocial factors alone. Physicians with migraine significantly more strongly support the use of a headache diary.
Interestingly, the rate of physicians recommending different drugs or treatment procedures for the acute or prophylactic treatment of migraine does not differ between those physicians with and those without migraine. There is only a trend towards a more frequent recommendation of magnesium and flunarizine; the only significant difference is for topiramate, which is more often recommended by physicians with migraine. This can result from the higher prevalence of neurologists among the migraine patients who use this drug quite often in migraine prophylaxis. The rate of recommendations for the different drugs and procedure in our sample reflects the national and international guidelines for the treatment of migraine (31,32). NSAIDs (including ASA and paracetamol) and triptans are recommended as the first choice in acute treatment; to a far lesser extent ergotamine derivatives are also named. For migraine prophylaxis, betablockers, flunarizine, the antiepileptic drugs valproic acid and topiramate, and amitriptyline are most often recommended. This is also in concordance with the national and international treatment guidelines.
Self-treatment of migraine
When physicians with migraine are asked about the treatment of migraine, extreme differences between the treatment of their own migraine and their treatment recommendations to their patients can be observed. Only half of the pain specialists, 15% of the neurologists and about one third of the headache specialists treat their own migraine attacks with a triptan, although nearly all of them have recommended triptans to their migraine patients. This observation cannot be explained just by the fact that physicians with migraine do not need acute attack treatment, since about 80% of them use NSAIDs for acute attack treatment. It might be that the fear for side effects of triptans or the knowledge of their costs (in Germany about €5 per tablet) prevent physicians from taking them themselves. Another explanation could be that many physicians have NSAIDs available in their practice or clinic, whereas the access to triptans is often limited. In addition, it might be that many physicians fear the presence of triptan prescription in their permanent insurance records and the stigma of suffering from a mental disorder, as this has been shown for psychiatrists treating their own depression (33). A presence of migraine in the insurance records would lead to higher rates for private health insurances in Germany.
We know from other studies that the majority of physicians practise self-treatment when they are ill, including such conditions as back pain, allergies, gastrointestinal discomfort, arthrosis, or even migraine and headache, in particular with respect to drug prescription (11,34–37). The most frequently prescribed drugs by neurologists for themselves were NSAIDs (27%) and gastrointestinal drugs (26%); about 12% had prescribed triptans for themselves or their relatives (37). Migraine belonged to those conditions which most of the neurologists would treat even hypothetically (37). Also, in our study nearly all physicians indicated that they treated their headache themselves and did not follow the treatment or the recommendations of colleagues. Therefore, the different treatment pattern in our samples is not the result of treatment suggestions by other colleagues.
A similar but even much more pronounced discrepancy can be observed regarding migraine prophylaxis. Only between 3.8% and 13.3% of all physicians with migraine take drugs for their own migraine prophylaxis, although nearly all of them have recommended a prophylaxis to their patients. Assuming that the indication for migraine prophylaxis is at least two to three attacks per month (which is according to the national guidelines (31)), 16.0% of the pain specialists, 17.0% of the neurologists, and 16.2% of the headache specialists with migraine have an indication for migraine prophylaxis. This means that physicians with migraine are reluctant to take a migraine drug prophylaxis.
In summary, our data suggest (but do of course not prove) that headache and pain specialists, and in particular neurologists, are much more reluctant to take specific acute and prophylactic drugs for their migraine than they recommend to their patients.
We are not aware of similar studies in other chronic diseases (e.g. diabetes in diabetologists or rheumatic disorders in rheumatologists). Only one study showed a considerably high prevalence of depression (over 22%) among psychiatrists (33), which was however not compared to the prevalence in the general population. Our study suggests that suffering from a disorder for which one is an expert or specialist might have an impact on attitudes towards this disorder and on treatment recommendations. Therefore, we suggest further investigations on other physician groups with respect to the impact of self-suffering on treatment decisions.
Limitations
Our study has several limitations. The most important limitation, we believe, is that our samples could be biased. We cannot be sure that our participants really represent the group we have defined. It could be that those physicians affected by migraine were more likely to respond than those without migraine because the interest of the first group in this survey is probably higher. However, since the response rate is above 50% and is in the range of similar surveys, we are confident that at least the trend of our results represents the underlying real figures. We were also not able to select our sample according to the age of the group because this is not known. We used questionnaires sent by mail and given directly to those who accepted this at a medical congress. This could also have influenced the willingness to respond.
Another limitation is that the data are based on the retrospective recall of the participants and not on prospective diary data. This is in particular a problem if lifetime prevalence is asked for. However, we hope that the recall bias (i.e. not remembering previous migraine attacks) is lower in physicians than is known from other epidemiological studies on migraine in the general population.
A further limitation could be that the physicians were not willing to respond correctly regarding their own status and their own treatment. As explained above, this could have consequences for the health system, and thus migraine prevalence and severity and drug treatment of migraine could have been underreported because the respondent feared that the anonymous survey was not really anonymous.
Conclusion
Neurologists and headache specialists show a significantly higher migraine (and also cluster headache) prevalence than general pain specialists, general practitioners, and the normal population in Germany. In headache specialists, this prevalence is even significantly higher than in neurologists. However, the migraine features do not differ between the different groups. Physicians with migraine have a more somatic concept of this disorder than their colleagues without migraine, and their treatment recommendations are more in concordance with the national guidelines and in particular consider the importance of trigger factors. Differences in treatment recommendations to patients could not be observed between physicians with and without migraine. On the other hand, physicians with migraine treat themselves in a different way than their patients; they themselves take less intensive drug therapy (fewer triptans, less drug prophylaxis). This might be of importance for further education in neurology and pain medicine, since the colleagues should be convinced that, for example, triptans are safe and evidence-based drugs. Another implication for future education of doctors is that there are still myths about the aetiology, the diagnosis, and the treatment of primary headaches. For example, brain imaging and EEG are still considered as absolutely necessary for the diagnosis of migraine even by some neurologists. Complementary medicine without any scientific evidence is still used even by some headache specialists. In summary, we conclude that a personal history of migraine of a treating physician might indeed matter for a patient with migraine.
Clinical implications
Neurologists and headache specialists show a significantly higher migraine prevalence than other physicians and the normal population. In headache specialists, this prevalence is even significantly higher than in neurologists. Migraine features do not differ between the different groups. Physicians with migraine have a more somatic concept of this disorder than their colleagues without migraine. Physicians with migraine treat themselves in a different way than their patients.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.