
Abstract
Background
Headache is a common presentation of postural tachycardia syndrome, yet robust prevalence data is lacking.
Objectives
To undertake a systematic review and meta-analysis to estimate the prevalence of headache disorders in postural tachycardia syndrome, and to explore the potential shared pathophysiological mechanisms that underpin these conditions as well as treatment options.
Methods
Three databases were searched for publications evaluating prevalence of migraine (primary outcome) and general and orthostatic headache (secondary outcomes) in patients with postural tachycardia syndrome. Two independent reviewers selected studies and extracted data. A random-effects meta-analysis calculated the pooled prevalence of migraine in postural tachycardia syndrome. A narrative literature review explored the pathophysiology and treatment options for concurrent headache disorders and postural tachycardia syndrome.
Results
Twenty-three articles met inclusion criteria. Estimated pooled prevalence of migraine in postural tachycardia syndrome was 36.8% (95% CI 2.9–70.7%). Various shared pathophysiological pathways for these conditions, as well as proposed treatment strategies, were identified.
Conclusions
Migraine is a commonly reported comorbidity in POTS, however the true prevalence cannot be determined from the current literature. Further studies are required to assess this comorbidity and investigate the underlying mechanisms, as well as identify effective treatment strategies.
Introduction
Postural tachycardia syndrome (POTS) and migraine are both disabling conditions that predominantly affect females of working age. POTS is characterised by symptoms of orthostatic intolerance of ≥6 months duration associated with an increase in heart rate by ≥30 beats per minute within 10 minutes of transitioning to a standing posture, without an accompanying fall in blood pressure of >20/10 mmHg (1). International epidemiological studies are lacking, but POTS is estimated to affect approximately 0.2–1% of the population in developed countries (2). POTS-related disability is significant, rendering up to 25% of people unable to work (3). POTS affects females 4–5 times more often than males (3).
Migraine is a common and disabling condition that presents with recurrent moderate to severe headache attacks and associated neurological and systemic manifestations (4). Worldwide, migraine is the leading cause of reversible disability in people under 50 years of age, affecting 1.3 billion people (4–6), with females affected two to three times more often than males (7). Although “headache” is considered to be a common presentation of POTS, it remains a poorly understood symptomatology in this cohort with respects to exact headache subtype, prevalence, pathophysiology, and optimal management strategies.
While there have been several studies reporting the prevalence of migraine and other headache disorders in POTS, there has been no attempt to systematically review these data and derive a robust prevalence estimate of migraine in POTS. Further, the common pathophysiological mechanisms underpinning these conditions warrant further exploration.
The aim of this study was to undertake a systematic review and meta-analysis of the existing literature to ascertain the prevalence of migraine and other headache disorders in POTS, and to conduct a narrative literature review to explore these conditions’ potential shared pathophysiology.
Methods
Study design
A systematic review and meta-analysis of the existing literature were performed. This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (ID: CRD42020196608). In addition, a narrative review of the included articles and other highly relevant articles was undertaken to explore the pathophysiology underpinning headache disorders and POTS, as well as treatment options.
Eligibility criteria
All cohort, case-control, or cross-sectional publications that reported the prevalence of headache in a clearly defined population of patients with POTS were included. Adult and paediatric populations were both included. Reviews, letters without original data, publications with limited methodological details, and non-English language studies were excluded. The primary outcome was the prevalence of migraine in POTS cohorts. Secondary outcomes were the prevalence of any headache disorder or orthostatic headache in this population.
Search strategy
A systematic literature review was performed of three electronic databases (Ovid MEDLINE and Epub Ahead of Print, In-Process and Other Non-Indexed Citations, Daily and Versions; Embase Classic +Embase and Cochrane Central Register of Controlled Trials) from inception until 6 July 2020 utilising a search strategy combining key words and related database-specific subject terms (supplementary attachment 1). Two authors (JCR and XP) independently evaluated the identified publications for eligibility on Covidence (8), performing two screening reviews of abstract evaluation followed by full-text evaluation. Discrepancies in screening results were resolved by a third author (EF). A repeat search of the literature was performed on 4 January 2022 and identified no further articles for inclusion.
Risk of bias assessment
Articles selected in the study were assessed for risk of bias using the Joanna Briggs Institute (JBI) for Critical Appraisal tool (Supplementary Material 1) (9,10). The JBI critical appraisal checklist for qualitative research was chosen as an appraisal tool for studies assessing prevalence. Risk of bias analysis was performed independently by two reviewers (JCR and XP). Discrepancies were resolved by discussion between reviewers.
Data extraction
A data extraction form was utilised to extract equivalent information from each included study. Data extracted included name of the first author, year of study, country of study cohort, study design, sample size, age of cohort, duration of POTS, diagnostic criteria of POTS (if stated), prevalence of headache, prevalence of each headache type (if stated), diagnostic criteria of headache (if stated). Prevalence figures and 95% confidence intervals were extracted or calculated from the available data using Wilson’s method (11).
Two reviewers independently extracted the predetermined data points using a standardised proforma. Data points were then compared for consistency, and any discrepancies were adjudicated by a EF.
Analysis
An initial descriptive analysis was undertaken for the included studies which reported the primary and/or secondary outcomes. Meta-analysis was undertaken of the primary outcome using a random-effects model, and a pooled prevalence figure was calculated with a 95% confidence interval. Heterogeneity between studies was assessed using the I2 statistic, with an I2 value above 75% indicating high heterogeneity (12). A sub-group analysis was undertaken to assess how the method of establishing migraine diagnosis affected prevalence. Sensitivity analyses were performed to evaluate the robustness of the results. Data analysis was performed in SPSS statistics (v27.0) and Microsoft Excel.
Results
Search results
The search strategy identified 504 studies for title and abstract screening, of which 23 studies fulfilled eligibility criteria for inclusion. A summary of the screening process is presented in Figure 1.

PRSIMA flowchart of studies screened for inclusion.
Included studies
The studies included in the analysis are summarised in Table 1. Of the included studies, 22 were cross-sectional and one a case control study in design. Twenty-one studies were single-centre studies, and two were patient surveys. All but three studies were conducted in the USA, precluding a geographic analysis. Only two studies reported that they employed the International Classification of Headache Disorders (ICHD-3) in the study design, and three studies interviewed patients to ascertain a headache diagnosis, with the remainder relying upon the electronic medical record (EMR), or patient self-report via questionnaire. The method by which the diagnosis of POTS was established varied between the clinical studies. In 15 studies, it was determined by clinical and/or laboratory assessment, in four by review of the EMR, in two by self-report, and in two the method of diagnosis was not reported.
Summary of studies included in analysis.

CS: Cross-sectional; CC: Case-control; JHS: joint hypermobility syndrome; R: retrospective; P: Prospective; NIH: National Institute of Health; CIHR: Canadian Institutes of Health Research; CANet: Cardiac arrhythmia network of Canada; POTS-A: Adults with POTS; POTS-P: Paediatrics with POTS; POTS-B: Both adults and paediatrics with POTS; POTS*: population group not defined: EMR; electronic medical record.
Risk of bias
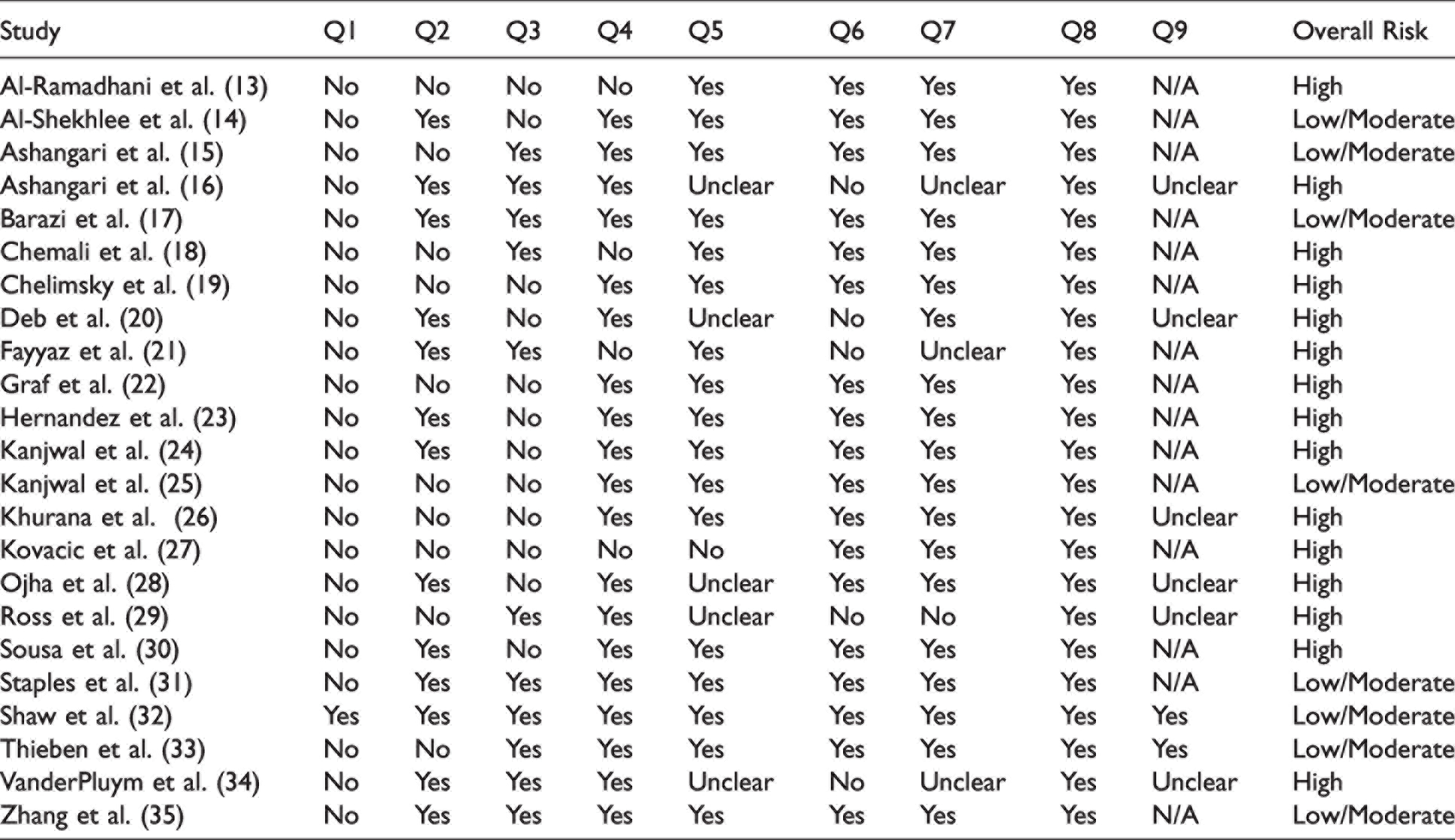
A summary of the JBI critical appraisal of risk of bias is included in Table 2. Due to the small number of studies, no studies were excluded from the review on the basis of the risk analysis.
JBI risk of bias.
Analysis
Prevalence of migraine
Of the 23 eligible studies, the prevalence of migraine in POTS was reported in 16 studies (Table 3) and included in the meta-analysis. The overall prevalence of migraine in the random-effects model (Figure 2) was 36.8% (95% CI 2.9–70.7%), with a high degree of heterogeneity (I2 = 86.75%).
Summary of reported prevalence of headache disorders in included studies.

ICHD-3; International Classification of Headache Disorders third edition.

Forest plot of the prevalence of migraine in patients with POTS, sub-grouped by method of data collection. CI; confidence interval, wes; weighted effect size, EMR; Electronic medical record.
Prevalence of headache disorder
In 12 studies, the authors either did not differentiate the headache disorder, or reported the combined prevalence of both migraine and other headache disorders (Table 3). The pooled prevalence of any headache disorder in these studies was 66.8% (95% CI 0–100%) (Figure 3). Only one of the included studies determined the prevalence of headache by interview, and the studies had significant heterogeneity (I2 = 96%), limiting detailed analysis.

Forest plot of the prevalence of a headache disorder in patients with POTS. CI; confidence interval, wes; weighted effect size.
Prevalence of orthostatic headache
The prevalence of orthostatic headache in patients with POTS was reported in four studies, two of which determined the diagnosis by patient interview (Table 3). The prevalence of orthostatic headache in this population ranged between 2.2% to 58.3%. Due to the small number of studies which provided this information, meta-analysis was not performed for orthostatic headaches.
Sub-group analysis based on migraine diagnosis method
A sub-group analysis was performed to explore the effect of differing methodologies for establishing migraine diagnosis on migraine prevalence. In the two studies that directly interviewed patients in order to establish a migraine diagnosis, the pooled prevalence of migraine was 92.3% (95% CI 24.0–100%) (Figure 2). The remaining studies, which relied on self-reporting via survey or EMR documentation, found a lower prevalence of migraine of 40.3% (95% CI 2.5–78.2%) and 32.1% (95% CI 4.0–60.2%), respectively.
Sensitivity analysis
Due to the small number of identified studies, no studies were excluded on the basis of the risk of bias assessment. Two sensitivity analyses were undertaken to determine the potential effect of this decision. Inclusion of articles only of a low or moderate risk of bias (answering yes to at least seven of nine questions) reported a prevalence of migraine of 36.8% (95% CI 3.0–70.7%) (Figure 4). Inclusion of studies that had undergone peer-review, excluding conference proceedings and posters, revealed a prevalence of migraine of 36.4% (95% CI 4.2–68.7%) (Figure 5).
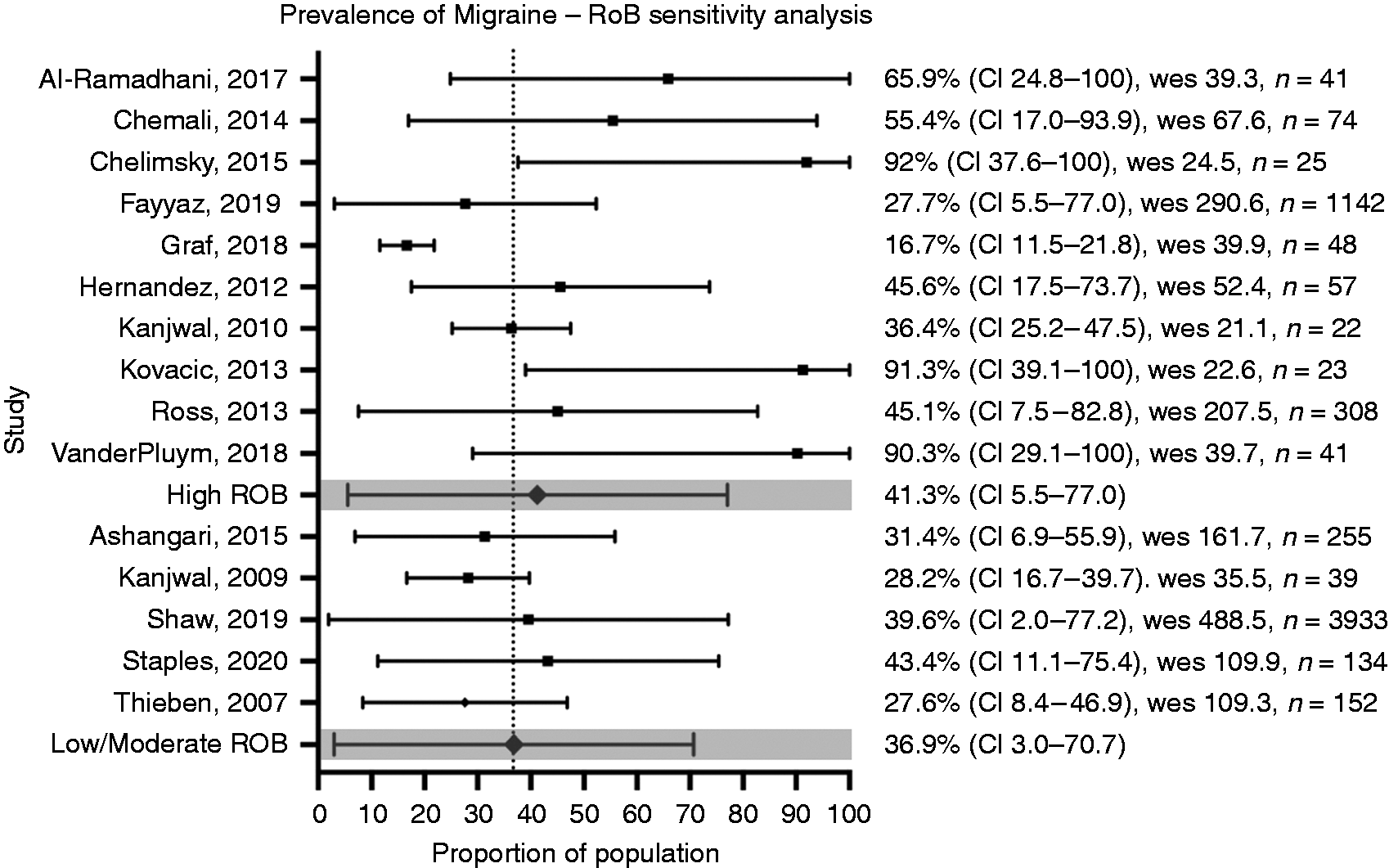
Migraine prevalence sensitivity analysis – risk of bias. CI; confidence interval, wes; weighted effect size, ROB; risk of bias.

Migraine prevalence sensitivity analysis – peer reviewed status. CI; confidence interval, wes; weighted effect size.
Finally, a sensitivity analysis was undertaken to determine the effect of adult vs paediatric population on the prevalence of migraine in POTS cohorts. Restriction of the analysis to studies evaluating the paediatric population revealed a prevalence of migraine of 50.1% (95% CI 9.9–90.3%). The prevalence of migraine in adult patients with POTS in this analysis was 31.2% (95% CI 5.4–57.0) (Figure 6).

Migraine prevalence sensitivity analysis – Age of population.
Discussion
The prevalence of headache disorders in POTS
This is the first publication evaluating the prevalence of headache in patients with POTS through a systematic literature search. Twenty-three eligible studies were identified for inclusion in this review. A meta-analysis was performed for 16 studies evaluating the prevalence of migraine, and 13 studies for headache type unspecified. The pooled-prevalence estimate of migraine in studies where patients were interviewed to establish the migraine diagnosis was 92.3%, higher than in studies which relied upon self-report (40.3%) or the EMR (32.1%) for migraine diagnosis.
The disparity in these estimates provides an insight into the heterogeneity of the literature, and the importance of methodological control and applying ICHD-3 criteria when assessing migraine in this population. Migraine headaches may either be under-recognised by treating clinicians, leading to underestimation, or even mistakenly reported, given light sensitivity may be reported in POTS without migraine (36).
The association of POTS in patients with migraine
The Dutch population-based study of migraine, the CAMERA study, has previously reported that the rate of POTS is not increased in patients with migraine (37). Considering the question from the other perspective, on the basis of this review, it appears that there is an increased prevalence of migraine in patients with POTS compared to population estimates of 15% (38).
The persistence of orthostatic and non-orthostatic symptoms despite control of the heart rate in POTS is suggestive of an ongoing unidentified central process in patients with POTS. Impaired processing of viscero-sensory information, conditioning, and behavioural amplification have been suggested to be contributory (39).
Orthostatic stress results in reflex sympatho-excitation from the rostral ventro-lateral medulla by reducing baro-receptor input to the nucleus of the solitary tract and activating the vestibulo-sympathetic reflex via the medial vestibular nucleus (40–44). Altered processing of interoceptive information relayed via the nucleus of the solitary tract and the parabrachial nucleus via the ventromedial portion of the thalamus could activate central circuits involved in visceral sensation, stress response and pain processing (39).
This central circuit, including the anterior cingulate cortex, insular cortex, amygdala, hypothalamus, and periaqueductal gray region have significant use-dependent synaptic plasticity which may lead to maladaptive responses to chronic stress or pain, and exhibit reciprocal interconnectivity. They may also have a role in controlling sympathetic cardiovascular output via the medulla (39,40,44–48).
Whilst untested, this theory of orthostatic stress activating the rostral ventrolateral medulla, and nociceptive activation of the thalamus and subsequent activation of central structures involved in pain modulation, stress response, behavioural arousal, and emotional response may provide a framework for understanding the presence and persistence of orthostatic and non-orthostatic symptoms of POTS and warrants further investigation.
The association of migraine in patients with orthostatic intolerance and POTS
Orthostatic intolerance is a commonly reported symptom amongst patients with migraine. The largest study assessing the prevalence of orthostatic intolerance was the CAMERA study, which found that compared to the general population, people living with migraine had significantly higher rates of orthostatic intolerance (32 vs 12%), and frequent syncopal episodes (13 vs 5%) (37). The study did not find a correlation between severity or sub-type of migraine with autonomic symptoms, and curiously did not find an association between POTS and migraine (37).
In light of the reported orthostatic intolerance associated with migraine, attempts have been made to assess the autonomic system in migraine, with varying results, prohibiting any useful conclusions. In non-invasive assessment of the autonomic system, a majority of studies have found evidence of sympathetic hypofunction (49–55), while other studies have found evidence of sympathetic hyperfunction (56), parasympathetic hypofunction (49,50), and parasympathetic hyperfunction (56).
Anatomically, there is a plausible connection between migraine and the autonomic nervous system (Figure 7). The nucleus tractus solitarius, locus coeruleus and periaqueductal gray are all involved in migraine as well as cardiovascular control. In particular, the periaqueductal gray region, which receives nociceptive inputs from the spinal and trigeminal dorsal horn, initiates sympathetic activation (57). Functional imaging studies would provide greater insight into the connection of these structures and their activation in patients with orthostatic intolerance.

Shared Migraine and autonomic pathways. Thal: Thalamus, Hyp: Hypothalamus, CVO: Circumventricular organs, PVN: Paraventricular nucleus, SON: Supraoptic nucleus, PAG: Periaqueductal Gray, LC: Locus coeruleus, NTS: Nucleus tractus solitarius, MNX: Motor Nucleus Cranial Nerve X, TCC: Trigeminocervical Complex, CVM: Caudal ventrolateral medulla, RVM: Rostral ventrolateral medulla, TNC: Caudal trigeminal nucleus, SSN: Superior Salivatory Nucleus, Hipp: hippocampus, Amy: Amygdala, ADH: Anti-diuretic Hormone.
Treatment of concomitant migraine and POTS
Recognition of the association of migraine and POTS has significance for patient management. Migraine preventative treatment may be chosen to treat both conditions, such as with beta-blockade, and lifestyle advice may need to be tailored in consideration of the co-morbidity (58,59). Further prospective study is required however to determine the optimal treatment of these comorbid conditions.
The association of orthostatic headache in patients with POTS
Orthostatic headaches are so termed due to the nature of the headache worsening with change in posture. Orthostatic headaches occurring in the setting of spontaneous intracranial hypotension is postulated to occur due to the increased gravitational pull when upright leading to an increase in brain sag at the level of the cerebrum and/or cerebral-spinal fluid (CSF) hypotension (60). Pain is believed to be caused by traction of pain-sensitive structures caused by brain sag, or dilation of cerebral veins and sinuses (60). The mechanism of orthostatic headache in POTS has not been elucidated.
In the International Classification of Headache Disorders (ICHD-3), orthostatic headache is described as a key clinical feature in most cases of spontaneous intracranial hypotension (SIH) (61). SIH is caused by a spontaneous CSF leak, often due to an underlying structural weakness in the spinal meninges (62). In a prospective study, SIH has been associated with a spectrum of connective tissue abnormalities and genetic disorders (63), however this association has not been found by others (64). Conversely, orthostatic headache has also been proposed as a predictive symptom in POTS. In one study of adolescent patients referred for tilt-table testing, orthostatic headache was observed in 89.2% (33/37) who had POTS and 21.2% (7/33) patients without POTS, which in this population translated to a pre-test sensitivity of 89.2% and specificity of 78.8% (65). Orthostatic headache therefore may be a presenting symptom of either SIH or POTS, and therefore presents a management challenge for treating clinicians. This diagnostic challenge has been highlighted by Graf et al. (66), who found that in a study of patients with SIH, all patients otherwise met the criteria for POTS on autonomic testing.
The majority of studies included in this analysis did not phenotype orthostatic headaches, and so meta-analysis of the prevalence of orthostatic headache was not possible. Similarly, prospective studies exploring the association of orthostatic headache and POTS are lacking, and as such the cause of the association can only be speculated upon. Prospective study is required in order to characterise orthostatic headache in POTS, formulate diagnostic criteria and gain insight into the underlying aetiology. The high reported prevalence of hereditary connective tissue disorders, and alterations in cerebral blood flow described in patients with POTS are two possibly significant observations that require further enquiry (67–69).
Limitations
The major limitation of this systematic review is the heterogeneity of the literature. The majority of the reviewed articles did not differentiate between headache disorders, employ the ICHD-3 criteria, or interview patients to establish headache subtype diagnosis. As discussed this could lead to either an under-, or over-reporting of the prevalence of migraine in POTS. Owing to the overall paucity of data, no articles were excluded on the basis of their risk of bias score, and furthermore the authors erred on the side of inclusiveness in their risk assessment, and did not require a 'gold-standard’ of prospective collection of data according to ICHD-3 criteria, when considering if the condition was collected in a reliable manner (Q6/7, JBI risk of bias tool). A sensitivity analysis was performed to try and address this issue, which did not identify significant differences between included studies, however given the overall heterogeneity and the overall lack of utilisation of the ICHD-3 criteria in these studies, it remains a significant limitation. Finally, this review provides an estimate of the prevalence of migraine primarily in clinic populations, which may not be representative of the general POTS population. Given the significant disability associated with migraine (6), this review highlights the need for further prospective studies in this area to delineate the true prevalence of headache disorders in POTS.
Conclusion
Migraine and orthostatic headache are commonly reported comorbidities in patients with POTS. However on the basis of the current literature and analysis, the true prevalence cannot be reliably determined. More studies with less heterogeneity and similar methods and study designs are required to identify and address this significant comorbidity, and investigate the underlying mechanisms and most effective treatment strategies.
Clinical implications
Migraine and headache disorders are common co-morbidities in patients with POTS Further robust prospective trials are required to assess the prevalence and impact of migraine in this population
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221095153 - Supplemental material for The prevalence of headache disorders in Postural Tachycardia Syndrome: A systematic review and meta-analysis of the literature
Supplemental material, sj-pdf-1-cep-10.1177_03331024221095153 for The prevalence of headache disorders in Postural Tachycardia Syndrome: A systematic review and meta-analysis of the literature by Jason C Ray, Xiuxian Pham, Emma Foster, Sanjay Cheema, Susan J Corcoran, Manjit S Matharu and Elspeth J Hutton in Cephalalgia
Footnotes
Author contributions
JCR designed the study protocol with the assistance of XP and EH. JCR designed the search strategy, reviewed by XP. JCR and XP independently reviewed studies for screening and data extraction, with EF as third author for resolving discrepancies. JCR, MSM, SC, and EH performed data analysis/interpretation. JCR was responsible for the preparation of the manuscript which was revised and edited by all authors.
Acknowledgements
Figures made with biorender.com
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
JCR has received funding from the Pharmaceutical Society of Australia supported by an unrestricted educational grant from Viatris. XP has no relevant disclosures to report. EF has been supported by grants from the NHMRC Medical Postgraduate Research Scholarship (APP1150482), The Royal Australasian College of Physicians Research Entry Scholarship, AVANT Doctors In Training Scholarship, and Monash University Bridging Postdoctoral Fellowship, and she/her institution has also received research grants from Brain Foundation, the Australian Epilepsy Research Fund, and the Viertel Foundation, outside the submitted work. SC has no relevant disclosures to report. SJC has no relevant disclosures to report. MSM serves on the advisory board for Allergan, Novartis, Eli Lilly, Autonomic Technologies Inc and TEVA and has received payment for the development of educational presentations from Allergan, electroCore, Eli Lilly, Novartis and TEVA. EJH has served on advisory boards for Sanofi-Genzyme, Novartis, Teva, Eli Lilly, Allergan, Lundbeck, been involved in clinical trials sponsored by Novartis,Teva, Calud, Cerecin, and has received payment for educational presentations from Allergan, Teva, Eli Lilly and Novartis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.