
Abstract
Objective
Head/neck pain is one of the primary symptoms associated with spontaneous cervical artery dissection. Still, data on pain quality, intensity, and long-term dynamics are scarce.
Methods
Spontaneous cervical artery dissection subjects were included if mural hematoma was visualised through T1 fat-saturated MRI at baseline. All available medical records were evaluated and patients were invited to standardised clinical follow-up visits at least 1 year after the index event.
Results
In total, 279 subjects were included in the ReSect-study with head/neck pain being the most frequent symptom of spontaneous cervical artery dissection (220 of 273, 80.6%). Pain was of pulling nature in 107 of 218 (49.1%), and extended to the neck area in 145 of 218 (66.5%). In those with prior headache history, pain was novel in quality in 75.4% (42 of 55). Median patient-reported pain intensity was 5 out of 10 with thunderclap-type headache being uncommon (12 of 218, 5.5%). Prior to hospital admission, head/neck pain rarely responded to self-medication (32 of 218, 14.7%). Characteristics did not differ between subjects with and without cerebral ischemia. Pain resolved completely in all subjects within a median of 13.5 days (IQR 12). Upon follow-up in 42 of 164 (25.6%) novel recurring headache occurred, heterogeneous in quality, localisation and intensity.
Conclusion
We present an in-depth analysis of spontaneous cervical artery dissection-related head/neck pain characteristics and its long-term dynamics.
Keywords
Introduction
The clinical presentation of spontaneous cervical artery dissection (sCeAD) includes a variety of symptoms ranging from local signs and symptoms, attributable to the local mass effect of the mural hematoma, to secondary TIA or ischemic stroke (1–3). As demonstrated previously, head/neck pain is the most frequent local sign and well-recognised to be one of the primary symptoms in sCeAD, commonly preceding cerebral ischemia (2–6). Yet, detailed pain assessments are scarce and information on specific clinical patterns in sCeAD-related head/neck pain are lacking. Reported clinical pain characteristics vary from unilateral temporal or occipital headache, dependent on the dissected cervical vessel, to migraine or cluster headache mimics (7–9). In addition to the sparse data in the acute setting, long-time dynamics have not been a focus in analyses of large sCeAD cohorts so far. Therefore, considerable differences exist concerning the frequency and characteristics of chronic post-sCeAD head/neck-pain (10). Consequently, we aimed to evaluate the quality, intensity, localisation and time-course of sCeAD-related head/neck pain in the acute setting as well as its long-term dynamics in our large single-centre sCeAD-cohort (ReSect-study).
Material and methods
Patient recruitment and selection
Details of patient selection and recruitment methods for the ReSect-study have been published previously (3,11). In short, a retrospective chart review of all subjects that suffered CeAD between 1998 and 2015 and were treated at the Medical University of Innsbruck was performed in December of 2015. Onwards, until December 2018, patients were screened prospectively. Subjects were evaluated according to the ReSect-study’s stringent criteria of inclusion. Patients were included if mural hematoma was evident in T1 fat-saturated MRI and no timely association to major head/neck trauma was reported. In all qualifying patients, all available electronic medical files (in-house and out-patient) were assessed. Each recruited subject was invited to a standardised in-house study visit encapsulating detailed history taking, clinical assessments, psychosocial questionnaires, whole body 3T contrast enhanced MRI as well a skin punch biopsy. The study specific visit was performed one year after sCeAD event at the earliest and by the same stroke neurologist in every instance. The classification of headache characteristics was done together with an in-house headache specialist. If subjects did not participate in the in-house follow-up, all available data were collected retrospectively through chart review (Supplemental Table 1).
Variable definitions
Details of head/neck-pain related to sCeAD in the acute phase and on a long-run were recorded and consequently evaluated by a headache specialist of the Medical University of Innsbruck according to the most recent guidelines of the International Headache Society (The International Classification of Headache Disorders 3rd edition [ICHD-3]) (9). Data were collected at two separate time points: a) during retrospective chart review of all recruited subjects; b) within the study-specific in-house follow-up visit. Pain intensity was assessed using the visual analogue scale by means of detailed patient history taking at follow-up as well as data from the electronic files of each patient. If patients reported recurrent head/neck pain that was new to them during follow-up, after the head/neck pain of the acute phase had already resolved, it was classified as a novel recurring head/neck pain. Group differences were assessed for the following subgroups: a) subjects suffering cerebral ischemia (ischemic stroke and/or TIA) vs. local signs and symptoms only. TIA was defined time-based as the duration of neurological symptoms <24 h and diagnosed by the treating stroke physician; b) sCeAD affecting internal carotid arteries versus vertebral arteries; c) women vs. men; d) sCeAD causing pseudoaneurysm vs. vessel stenosis. Concerning vessel pathologies, and subjects with both pseudoaneurysm and stenosis were excluded from the respective subgroup analysis. Dissection recurrence was defined as two sCeAD occurring at least 6 months apart.
Statistical methodology
Descriptive data are presented as sample number of total population (n) with respective percentage. Categorical variables were compared across groups using χ 2 test. Likelihoods for respective outcomes were calculated using a binary logistic regression. For group comparisons of continuous variables non-parametric tests were performed utilising a Mann–Whitney U test or Kruskal–Wallis test, where applicable. The family-wise error rate for multiple comparisons was addressed using the Holm–Bonferroni correction. To identify differences in means between subjects attending and not attending the ReSect-study visit, an analysis of variance was performed. Subjects were classified by age into categories by building three intervals comprising two standard deviations of mean. As level of significance a p-value below 0.05 was considered significant.
Standard protocol approvals, registration, and patient consents
All analyses were approved by the local ethics committee at the Medical University Innsbruck and appropriate informed consent of patients who took part in the ReSect-Study was obtained.
Data availability
Study data that support the findings of this study are available from the corresponding author upon reasonable request after ethics approval and receipt of a signed data transfer agreement.
Results
In total, 279 subjects were enrolled in the ReSect study. Table 1 holds baseline as well as relevant patient history, especially concerning head/neck pain, for the entire cohort. Supplemental Table 1 depicts baseline characteristics of those who did and did not attend the in-person ReSect-study visit. As these groups did not differ in any relevant characteristic, the cohort was pooled and all analyses were performed in all included subjects. Clinical features of sCeAD and imaging characteristics are described in Table 2 and head/neck pain details are given in Table 3. Head/neck pain was the most frequent symptom attributable to sCeAD (220 of 273, 80.6%) in the ReSect study cohort. In these subjects experiencing pain due to sCeAD, onset was sudden in every patient (220 of 220). Quality was of pulling nature in 107 of 218 (49.1%), localised at the ipsilateral site of sCeAD in all instances but did extend to the contralateral hemicranium in 122 of 217 (56.2%) and to the neck area in 145 of 218 (66.5%). In those with prior history of primary headache, pain was novel in quality in 43 of 55 (75.4%). The median duration until subjects experienced head/neck pain relief at index the event was 15.29 hours (SD: ± 9.94) with longer durations in patients with vertebral artery dissection compared to carotid artery dissection (median: 15.0 [IQR 10.0–21.0] vs. 11.0 [IQR 6.0–18.0] hours; p = 0.025). Pain resolved in all (220 of 220) subjects within a median of 13.5 (IQR 12) days. Pain was continuous in all patients (220 of 220) and of moderate intensity (median 5 of 10 [IQR 3] on visual analogue scale). None of our subjects reported symptoms suggestive of cluster-type headache, with sudden onset thunderclap-type intensity being uncommon as well (12 of 218, 5.5%). Migraine-like characteristics, such as photo- (four of 218, 1.8%) and phonophobia (one of 218, 0.5%), were rare, with nausea as an unspecific symptom (i.e. not related to cerebral ischemia) being evident in 25 of 218 (11.5%). In those subjects reporting a history of migraine, sCeAD-related pain was novel in quality in 81.1% (30 of 37). When comparing subjects with and without cerebral ischemia due to sCeAD at baseline, no difference was found concerning the head/neck-pain localisation (p = 0.548), quality (p = 0.372), intensity (p = 0.624) or response to self-administered analgesia (p = 0.315). Subjects with sCeAD causing local symptoms only (i.e. no cerebral ischemia), however, were more likely to have head/neck pain compared to those with cerebral ischemia (relative risk increase 66.7% vs. 13.9%, p < 0.001). Pain quality in vertebral artery dissection was mostly of pulling nature (68 of 116, 58.6%) and mostly dull-throbbing (44 of 93, 47.3%) in anterior circulation sCeAD (p = 0.003). Women solely differed to men in likelihood of sCeAD being painful (88.1% vs. 75.6%; p = 0.011). Lastly, there was a trend towards sCeAD being more frequently causing pain if it resulted in pseudoaneurysm formation and not in vessel stenosis (92.1% vs. 79.0%; p = 0.058) but neither pain quality (p = 0.945), localisation (p = 0.307) nor intensity (p = 0.147) differed in this subgroup analysis. Age was a significant predictor for painful dissection with younger subjects being more likely to experience pain than older subjects. During the median follow-up duration of 6.5 years, and after the initial CeAD-related head/neck-pain has already resolved, 42 of 164 (25.6%) of patients developed novel recurring head/neck pain, which was heterogeneous in quality, intensity and localisation and (only rarely) matched the head/neck pain at baseline (five of 42, 11.9%). Subjects that developed novel recurring pain did not differ concerning baseline or sCeAD characteristics from those who did not. Further, long-term concomitant medication, especially antiplatelet therapy, did not differ between the two groups (antiplatelet use upon follow-up 24 of 42 [57.1%] vs. 100 of 161 [42.2%]; p = 0.56).
Baseline characteristics of entire cohort.

*n (%); #mean (min-max).
Overview of demographic data collected.
aOther headache types include any other primary headache, medication overuse headache (MOH) and headaches that could not be classified according to the International Classification of Headache Disorders, 3rd edition (ICHD-3). Sample size (n) varies as a result of pair-wise deletion of missing data.
Presentation of dissection.

*n (%).
Overview of clinical and imaging presentation of dissections. Pain was the most common initial symptom in both groups. Spontaneous cervical artery dissection was commonly accompanied by cerebral ischemia. Sample size (n) varies as a result of pair-wise deletion of missing data.
Pain description and concomitant symptoms.
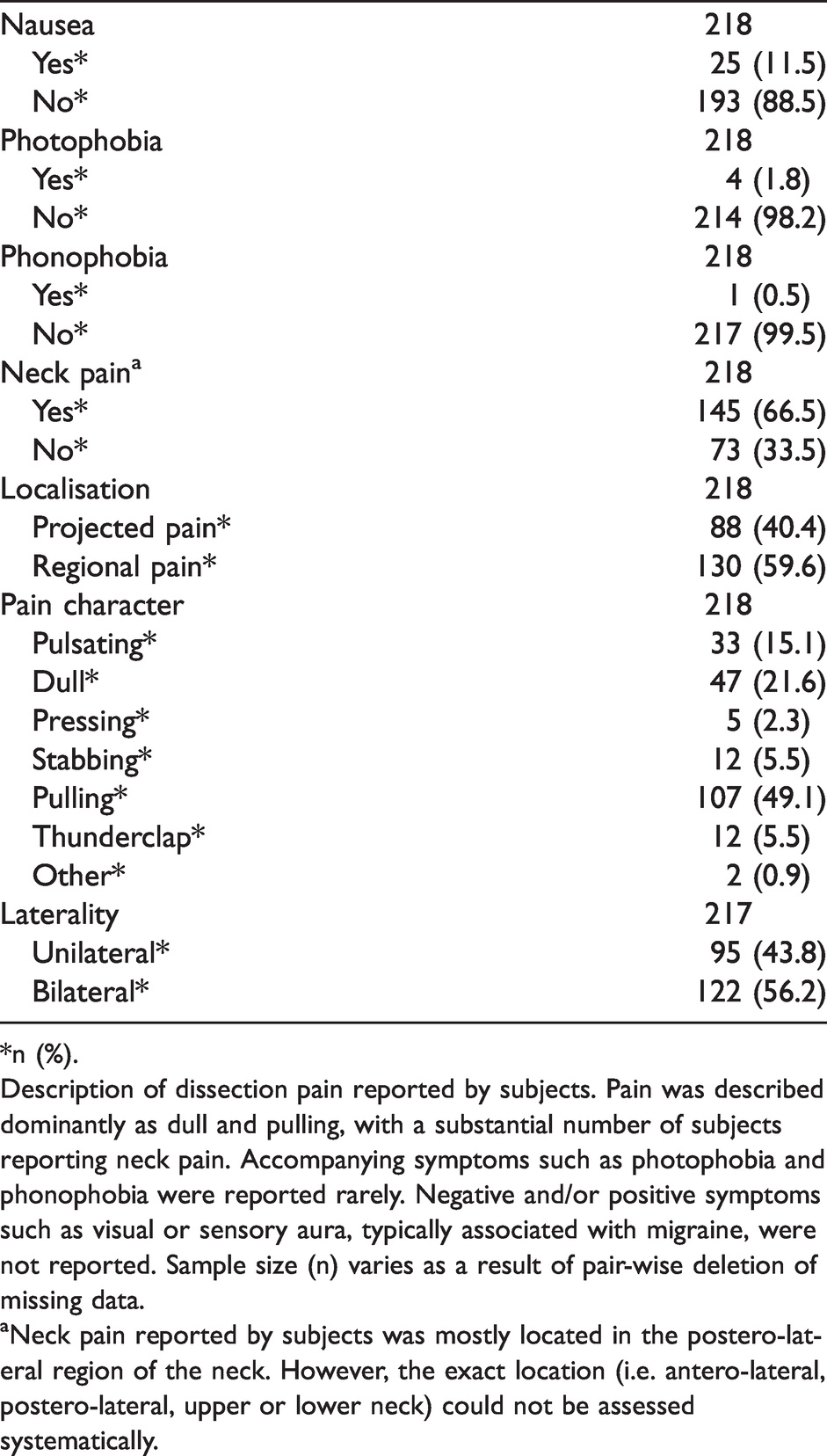
*n (%).
Description of dissection pain reported by subjects. Pain was described dominantly as dull and pulling, with a substantial number of subjects reporting neck pain. Accompanying symptoms such as photophobia and phonophobia were reported rarely. Negative and/or positive symptoms such as visual or sensory aura, typically associated with migraine, were not reported. Sample size (n) varies as a result of pair-wise deletion of missing data.
aNeck pain reported by subjects was mostly located in the postero-lateral region of the neck. However, the exact location (i.e. antero-lateral, postero-lateral, upper or lower neck) could not be assessed systematically.
Discussion
Recently, sCeAD-related research has primarily focused on genetic and pathophysiologic work-up as well as the identification of laboratory biomarkers establishing the risk of dissection recurrence (11–15). Head/neck pain is well recognised as one of the most frequent symptoms in sCeAD and, as it can predate cerebral ischemia in these subjects, early clinical detection is of the essence (2,3,7,8,10) Over the past decade, increased availability of MR imaging has facilitated the diagnosis of sCeAD, in the anterior and even more so in the posterior circulation (16). Most of what we know about headache characteristics in sCeAD stems from older descriptive studies that are likely to have missed smaller and non-stenotic dissections as well as dissections of the vertebral arteries (4). Through our study, we present an in-depth analysis of head/neck pain encompassing characteristics in the acute phase and on a long-run within our large single-centre long-term cohort of sCeAD patients (ReSect study). To date, sCeAD-related head/neck pain in the acute phase has mostly been described as gradual at onset, of throbbing quality, of moderate to severe intensity and unilaterally ipsilateral to the dissected cervical artery (2,8,10,17). Our data, as depicted in Tables 1–3 and Figure 1, however, suggests otherwise. In our cohort, each patient reported a sudden onset of head/neck pain, which additionally was continuous in course and rarely responded to self-administered oral analgesics. A pulling pain quality was present in half of patients with sCeAD. Neck pain was mostly reported in the postero-lateral region. Due to the dissemination of the pain, however, the exact localisation could not be addressed systematically in this study. The traditional presentation (throbbing to dull) was the predominant pain characteristic in internal carotid artery dissection in our evaluation. This fits well to the hypothesis that older studies primarily included subjects with internal carotid artery sCeAD with only more recent studies being able to adequately encapsulate vertebral artery dissection as well, as a result of imaging modality improvement (10). Further, our data does not support recent studies suggesting a high prevalence of thunderclap-like onset of sCeAD-related headache (described in up to 45%) and high frequency of migraine-like features such as phono- and photophobia in sCeAD subjects, if the vertebral artery is affected (18). Au contraire, thunderclap-like onset was reported in only 5.5% of cases in our cohort and was predominantly evident if subjects presented with cerebral ischemia (11 of 12 reporting thunderclap-like onset had ischemia); however, thunderclap headache per se was not a predictor for ischemia (p = 0.064). Photo- and phonophobia were equally rare. Consequently, in the acute phase, sCeAD-related head/neck pain can be differentiated from primary headache syndromes most certainly as it is characterised as novel in almost all cases; furthermore, accompanying symptoms such as photo- and phonophobia, nausea and osmophobia only rarely occur in sCeAD related head/neck pain (Figure 1). Therefore, it can be emphasised that in an emergency department setting the clinical distinction between sCeAD and primary headaches can be based on the red flag “onset of a new type of headache”. Presence of accompanying symptoms, usually related to migraine, render sCeAD less likely. Additionally, our data aids in counselling patients, in that sCeAD-related head/neck pain always resolves within a median of 2 weeks. Still, novel recurring head/neck pain heterogeneous in quality and intensity developed in the long-run in one of four subjects. This is considerably higher than in previous clinical studies of sCeAD-related pain and exceeds the expected rate of developing a new type of chronic headache in the general population (19–22).

Differential features of sCeAD related head/neck pain compared to other headache syndromes.
Strengths of our study include the strict inclusion criteria with mural hematoma visualisation in T1 fat-saturated MRI in the acute phase being obligatory, therefore generating a cohort consisting of subjects with definitive sCeAD diagnosis. Additionally, the ReSect study encompasses one of the largest structured single-centre sCeAD cohorts with one of the longest in-person follow-ups in these patients to date. Limitations include the missing data on novel recurring head/neck pain generated by the group evaluated retrospectively. Lastly, even though we cannot exclude a certain recall bias of the included subjects, the combined retrospective approach incorporating all available electronic patient records with the structured in-house follow-up minimises the effect.
Conclusion
Head/neck pain is the main symptom related to sCeAD and can, as it regularly predates cerebral ischemia, assist in the primary prevention of ischemic stroke. Pain in sCeAD can, through certain traits, be differentiated from primary headache syndromes in the acute setting, consequently prompting adequate cerebrovascular imaging and secondly enabling primary prevention of cerebral ischemia through early initiation of antithrombotic treatment. Novel recurring head/neck pain after sCeAD remains heterogeneous in quality and intensity.
Clinical implications
Head/neck pain is the most frequent symptom in sCeAD and can predate cerebral ischemia. Pain characteristically is of sudden onset, pulling nature, continuous in course and rarely responds to self-administered oral analgesics. Pain in sCeAD is characterised as completely novel and can therefore be differentiated from primary headache syndromes in the acute setting. Novel recurring head/neck pain after sCeAD is rare and heterogeneous in quality and intensity.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221079298 - Supplemental material for Head/neck pain characteristics after spontaneous cervical artery dissection in the acute phase and on a long-run
Supplemental material, sj-pdf-1-cep-10.1177_03331024221079298 for Head/neck pain characteristics after spontaneous cervical artery dissection in the acute phase and on a long-run by Lukas Mayer-Suess, Florian Frank, Thomas Töll, Christian Boehme, Elke R Gizewski, Gudrun Ratzinger, Gregor Broessner, Stefan Kiechl and Michael Knoflach in Cephalalgia
Footnotes
Author contributions
LM-S: Data acquisition, analysis and drafting of the manuscript; FF: Data analysis, drafting of manuscript, provided figures; TT: Critical revision of the manuscript; CB: Critical revision of the manuscript; ERG: Critical revision of the manuscript; GR: Critical revision of the manuscript; GB: Assisted in drafting of manuscript; SK: Critical revision of the manuscript; MK: Conceptualised the study, assisted in drafting of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Study funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LM-S, MK: OeNB Anniversary Fund (#15644); FF: Honoraria from Novartis AG; DOC Fellowship of the Austrian Academy of Sciences at the Department of Neurology, Medical University of Innsbruck. The remaining authors report no disclosures.
Additional funding: Excellence initiative VASCage (Center for Promoting Vascular Health in the Ageing Community), R&D K-Center of the Austrian Research Promotion Agency (COMET program – Competence Centers for Excellent Technologies, No. 16427332) funded by the Austrian Ministry for Transport, Innovation and Technology, the Austrian Ministry for Digital and Economic Affairs and the federal states of Tyrol, Salzburg and Vienna. The study was not industry funded.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.