
Abstract
Background
Merging of sensory information is a crucial process for adapting the behaviour to the environment in all species. It is not known if this multisensory integration might be dysfunctioning interictally in migraine without aura, where sensory stimuli of various modalities are processed abnormally when delivered separately. To investigate this question, we compared the effects of a concomitant visual stimulation on conventional low-frequency somatosensory evoked potentials and embedded high-frequency oscillations between migraine patients and healthy volunteers.
Methods
We recorded somatosensory evoked potentials in 19 healthy volunteers and in 19 interictal migraine without aura patients before, during, and 5 min after (T2) simultaneous synchronous pattern-reversal visual stimulation. At each time point, we measured amplitude and habituation of the N20-P25 low-frequency-somatosensory evoked potentials component and maximal peak-to-peak amplitude of early and late bursts of high-frequency oscillations.
Results
In healthy volunteers, the bimodal stimulation significantly reduced low-frequency-somatosensory evoked potentials habituation and tended to reduce early high-frequency oscillations that reflect thalamocortical activity. By contrast, in migraine without aura patients, bimodal stimulation significantly increased low-frequency-somatosensory evoked potentials habituation and early high-frequency oscillations. At T2, all visual stimulation-induced changes of somatosensory processing had vanished.
Conclusion
These results suggest a malfunctioning multisensory integration process, which could be favoured by an abnormal excitability level of thalamo-cortical loops.
Introduction
Merging of sensory information is an essential process in all species for guiding biological behaviours and enabling adaption to the environment. When two different sensory modalities are activated simultaneously brain circuits integrate them, forming a unique and better percept, a process defined as “multisensory integration” (1). Both in humans and in animal models, co-application of two sensory stimuli of a different modality results in greater neural activation than the sum of the activations produced by each stimulus separately (2). There are many cortical and subcortical sites where sensory information converge and are processed by specialised neurons that can respond to the simultaneous presentation of different types of sensory stimuli. One of the first pieces of evidence in favour of the existence of these neurons was obtained long ago by Rizzolatti et al. (3). They described the existence of neurons in the premotor cortex of macaque monkeys that could be activated both when visual or somatosensory stimuli were presented alone and when they were given simultaneously (bimodal neurons) (3). A small portion were even trimodal and could also be activated by auditory stimuli (4). Moving to healthy humans, evidence from neuroimaging studies suggest the existence of multisensory areas with visuo-tactile responses in cortical and subcortical regions. Brain regions activated by both visual and tactile stimuli with multisensory linear (additive response) were identified in posterior and inferior parietal cortices (5).
Given the sensitivity of migraine patients to multiple environmental stimuli and knowing that their processing of unimodal visual, somatosensory, olfactory, or auditory stimuli is abnormal over the migraine cycle (6), it is tempting to speculate that multisensory integration could also be altered. During a migraine attack, somatosensory hypersensitivity (cutaneous allodynia), photo- and phonophobia, as well as osmophobia are the rule. Such hypersensitivity to all sensory modalities is also present in the interictal phase, though to a lesser degree: Compared with healthy subjects, migraineurs may have lower cutaneous pain thresholds (7,8), lower visual discomfort thresholds (9) and increased sensitivity to sounds (9–11). Although there are abnormalities in unimodal sensory processing, it seems clinically appropriate in migraine to consider multimodal hypersensitivity rather than to focus on a single sensory modality. This is supported by some facts. For instance, migraine attacks can be triggered by olfactory, auditory, and visual stimuli (12,13). Symptoms could influence each other, with headache intensity correlating directly with presence and intensity of photo-, phono- and osmophobia and vice versa (14). Furthermore, neuroimaging studies have shown in migraine an aberrant activation and atypical functional connectivity in multisensory convergence areas of the brain (15).
Based on these observations, we hypothesised that migraine patients could have a different adaptation to multisensory stimulation, indicating that their aberrant sensory processing is not only limited to unimodal sensory modalities. To demonstrate this, we studied multisensory integration in migraine patients by recording somatosensory evoked potentials (SSEP) combined with simultaneous visual stimulation. This allows study of non-invasively cortical responsivity by analysing the baseline level of cortical excitability and habituation occurring during prolonged stereotyped stimulation (16), as well as thalamocortical activation indexed by high-frequency oscillations extracted via high frequency band-pass filtering of SSEP recordings.
Materials and methods
Subjects
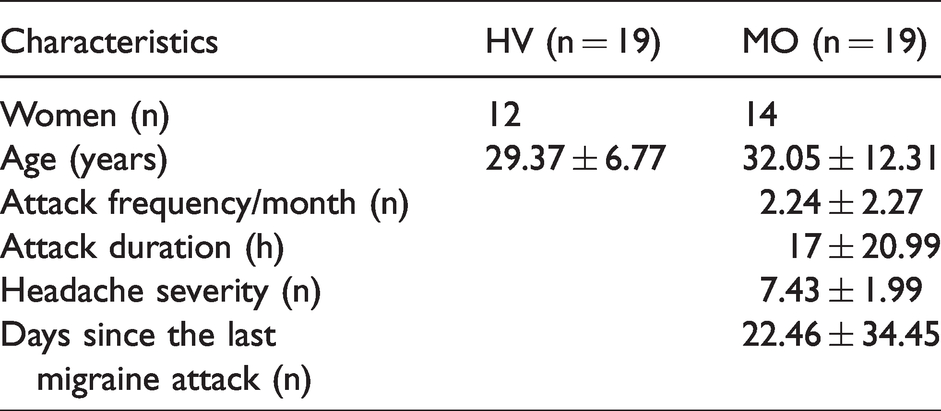
Nineteen patients with a diagnosis of episodic migraine without aura according to the diagnostic criteria of the International Classification of Headache Disorders (ICHD third edition) (17) were recruited among consecutive patients attending the Headache clinic of Sapienza University of Rome Polo Pontino. They were recorded during the interictal period; that is, at least 3 days before and after an attack. None of them was taking a prophylactic therapy or had taken one during the last 3 months. We collected information about the patients’ clinical characteristics: Severity of headache attacks (VAS 0–10), duration of the migraine disease (years), attack duration (hours), monthly attack frequency (n/month), and days elapsed since the last (n). For comparison, we recorded with the same protocol 19 healthy volunteers (HV) recruited amongst medical school students and healthcare professionals at Sapienza University in Latina. The clinical and demographic characteristics of the recruited subjects are shown in Table 1. Inclusion criteria were absence of a personal or family history (first- and second-degree relatives) of any neurological or psychiatric illness and any overt medical condition. Subjects with regular medication intake, except for the contraceptive pill, were excluded. All study participants underwent an ample neuro-ophthalmological evaluation including best-corrected visual acuity, intraocular pressure measurement, slit-lamp biomicroscopy, and binocular indirect ophthalmoscopy. To minimise variability due to the hormonal influences on cortical excitability, we managed to schedule recording sessions of female subjects outside their premenstrual or menstrual periods. The project was approved by the ethical review board of the Faculty of Medicine, University of Rome, Italy, and all subjects gave written informed consent to participate in the study.
Demographic and clinical features of included healthy volunteers (HV) and migraine patients. Data expressed as means ± SD.
Procedure
Data acquisition
Somatosensory evoked potentials (SSEP)
SSEP were elicited using the procedure published in our previous studies (18,19). In brief, EEG signals were acquired after electrical stimulation (1.2 times motor threshold, 3.1 Hz repetition rate) of the median nerve at the right wrist. Electrodes were placed as follows: One recording electrode at the Erb point ipsilateral to the stimulation side, referred to the contralateral Erb point; one recording electrode at the level of the fifth cervical spinous process and one at the level of the contralateral parietal cortex (C3′, 2 cm posterior to C3), both referred to Fz; the ground electrode was placed on the right arm.
We acquired the brain signals using a Digitimer D360 preamplifier and amplifier (Digitimer Ltd, UK) and a CED power1401 analogue-to-digital converter (Cambridge Electronic Design Ltd, Cambridge, UK). While the subject sat relaxed with open eyes in an armchair in an acoustically isolated room with dimmed lights, we acquired 300 traces of 200 ms duration (sampling rate 5000 Hz) that were analysed off-line using the Signal 4.11 software. After suppressing artefacts with the software’s automated procedure, we first analysed the evoked low-frequency (LF) responses by applying a digital filter between 0 and 450 Hz and measured latency and amplitude of the N9, N13, N20, P25 and N33 components. Thereafter, we calculated SSEP habituation, as in our previous studies, by dividing the first 200 traces into two blocks of 100 sweeps and computing the linear regression between N20-P25 amplitudes of the first and second block of acquisitions.
High-frequency oscillations (HFO)
The extraction of the HFO was performed according to the method described elsewhere (18,19). After elimination of the stimulus artefact, HFO superimposed on the N20 left parietal component of the SSEP was extracted applying an off-line digital zero-phase shift band-pass filtering between 450 and 750 Hz. We identified two separate bursts of HFO: An early one occurring in the latency interval of the ascending slope of the conventional N20 component, and a late one occurring in the time interval of the descending slope of N20, sometimes extending into the ascending slope of the N33 peak. We measured the latency of the negative oscillatory maximum and the maximum peak-to-peak amplitude of the early and late oscillatory bursts. All SSEP recordings were performed in the morning by the same investigator (GS), who was not involved in the patient’s enrolment phase. Immediately after the recording session, all traces were anonymised and blandly analysed offline by one investigator (GC).
Visual stimulation
A TV monitor surrounded by a uniform luminance field of 5 cd/m2 was placed in front of the subjects. Before performing the visual stimulation, each subject was left for some time in the ambient room light to obtain a stable pupillary diameter. Visual stimulation consisted of full-field checkerboard patterns (contrast 80%, mean luminance 50 cd/m2) generated on the TV monitor with a 3.1 reversal rate per second. The left eye was covered by a patch and the visual stimulation was applied only on the right eye. Subjects were instructed to fixate with their right eye a red dot in the middle of the screen. The single checks subtended a visual angle of 15 minutes at a viewing distance of 114 cm. The reversal of the checkerboard was synchronised with the electrical stimulus applied to the wrist.
Study protocol
In both groups of subjects, we recorded 300 consecutive SSEP before (T0), during (T1), and after (T2) simultaneous pattern-reversal visual stimulation with the black-and-white checkerboard (Figure 1). The recording sessions were separated by 5 min of rest.

Schematic representation of study protocol. Three hundred consecutive somatosensory evoked potentials (SSEPs), elicited by electrical stimulation of the right median nerve, were performed before (T0), during (T1), and 5 min (T2) after simultaneous visual stimulation with a black-and-white checkerboard pattern generated on a TV monitor with a 3.1 reversal rate per second. The reversal of the checkerboard is synchronised with the electric stimulus sent to the wrist.
Statistical analysis
All recordings were processed offline by a single investigator. Data were analysed using Statistica for Windows v8.0 (StatSoft Inc., Tulsa, USA). A sample size calculation based on a preliminary analysis of initial nine HV and nine patients with MO showed that, for a power of 0.80 and an alpha error of 0.05, 19 subjects per group (standardised effect size of 0.679 in HV and 0.668 in MO) were needed to disclose a significant difference in the habituation slope between two dependent SSEP recordings (T0 vs. T1). A Kolmogorov–Smirnov test confirmed the Gaussian distribution for latencies and amplitudes of each SSEP component. Two separate repeated measures analysis of variance (RM-ANOVA) were performed to analyse the effect on N20-P25 SSEP block amplitudes and on the slope of the linear regression line of amplitudes over the two blocks of 100 averaged traces, with “time” (three levels: T0, T1, T2) and “group” (two levels: HV, MO) as independent variables. We verified the assumption of sphericity by using the Mauchly Sphericity Test and, in the case of violation, Greenhouse–Geisser (G–G) epsilon (ε) adjustment was used. In RM-ANOVA, the effect size was quantified using partial eta-squared (partial η2). Post-hoc analysis was performed using Tukey’s test. Pearson’s correlation test was used to search for correlations between first block N20-P25 amplitude, habituation and clinical features of migraine (duration of migraine history, mean monthly attack frequency, mean monthly attack duration, number of days since the last migraine attack, headache severity). p-values inferior to 0.05 were considered statistically significant.
Results
Low-frequency (LF) SSEP
SSEP recordings from all participants yielded analysable data. Before the simultaneous visual stimulation, grand-average SSEP N9, N13, N20, P25, and N33 latencies and amplitudes did not differ between groups (all p > 0.07).
The RM-ANOVA model using block N20-P25 SSEP amplitude as dependent variable showed no significant effect for the variable “group” (F1,108 = 1.12, p = 0.292), “time” (F2,108 = 0.14, p = 0.871), “group” × “time” (F2.108 = 0.01, p = 0.989), block (F1,108 = 0.57, p = 0.452), and “block” × “time” (F2,108 = 0.79, p = 0.457), but a significant “block” דgroup” (F1,108 = 10.41, p = 0.002) and “block” דgroup” × “time” (F2,108 = 9.35, p < 0.001) interaction (Table 2).
Reports of the results of the RM-ANOVA analyses, with partial eta-squared biased estimator of the variance and observed power.

Subsequently, we analysed the change of SSEP amplitudes over the two blocks of 100 responses to study the repetition effect; that is, the habituation (Figure 2(a),(b)). RM-ANOVA using N20-P25 amplitude slope as the dependent variable showed a non-significant effect for the variables “group” (F 1,36 = 1.83, p = 0.185) and “time” (F 1,72 = 0.08, p = 0.924), but a significant effect for the interaction “group” × “time” (F 2,72 = 10.64, p < 0.0001) (Mauchley sphericity test: p = 0.352, partial η = 0.228, op = 0.987). Post-hoc analysis revealed that linear trends of baseline (T0) N20-P25 SSEP amplitudes were decremental; that is, habituated normally, in HV (−0, 34658 μV/block), while they were incremental; that is, lacked habituation, in MO patients (+0, 382319

(a) Amplitudes of the SSEP N20-P25 component (mean ± SEM) over the two sequential blocks of 100 responses and (b) slope of the linear regression line of amplitudes over the two blocks of 100 responses at T0 (before), T1 (during) and T2 (after visual pattern-reversal stimulation) in healthy volunteers (HV, blue) and migraine without aura patients (MO, orange).
During the bi-modal stimulation (T1), the N20-P25 SSEP slope changed significantly to become positive in HV (−0.34658 at T0 vs. 0.191304
At T2; that is, 5 min after the visual pattern-reversal stimulation, the changes observed at T1 had disappeared and all responses were not different anymore from those recorded at T0 (Figure 2(a),(b)). No correlations were found between neurophysiological parameters and clinical migraine features.
HFO
ANOVA disclosed no significant differences in latencies of the negative oscillatory maximum for early and late bursts of somatosensory HFO, either between groups or between timepoints of recordings in migraine patients.
The RM-ANOVA model using amplitude of the early HFO burst as dependent variable showed a non-significant effect for the variable “group” (F1,36 = 1.24, p = 0.273) and “time” (F2,72 = 0.39, p = 0.676), but a significant “group” × “time” (F2,72 = 11.32, p < 0.0001) interaction effect. On post-hoc analysis, the maximal amplitude of the early HFO burst at T0 was significantly smaller in MO patients than in HV (p = 0.023) (Figure 3(a)).

Maximal amplitude (mean + SEM) of early (a) and late (b) SSEP high-frequency oscillations (HFO) at T0 (before), T1 (during) and T2 (after pattern-reversal visual stimulation) in healthy volunteers (HV, blue) and migraine without aura patients (MO, orange).
During bimodal stimulation in HV, early HFO amplitude tended to be smaller than before the visual stimulation (p = 0.07). By contrast, in MO patients, bimodal stimulation significantly increased early HFO amplitude (p = 0.004), which returned to the pre-stimulation values 5 min later at T2 (Figure 3(a)).
RM-ANOVA with amplitude of the late HFO burst as dependent variable disclosed no significant effect for the variables “group” (F1,36 = 0.493, p = 0.487) and “time” (F2,72 = 0.678, p = 0.511), or for the interaction “group” × “time” (F2,72 = 0.060, p = 0.942) (Figure 3(b)). No correlations were found between neurophysiological parameters and clinical migraine features.
Discussion
The main results of the present study can be summarised as follows: i) simultaneous bimodal somato-visual stimulation does not significantly change the pre-activation level of the somato-sensory cortex as indexed by the amplitude of the first SSEP block, but this amplitude tends to increase in interictal MO patients and to decrease in HV; ii) simultaneous visual stimulation significantly changes SSEP habituation in opposite directions in MO patients (increase) and HV (decrease), and this effect does not outlast the stimulation; iii) the bimodal stimulation induces in migraine patients, but not in HV, a significant amplitude increase of the early burst of SSEP high frequency oscillations, which reflect thalamocortical activity.
In accordance with previous findings, we confirm that migraineurs have between attacks a lack of habituation to repetitive unimodal somatosensory stimuli (20,21) and lower activation of thalamocortical loops (18,19) compared to healthy controls. The mechanisms underlying these abnormalities are not yet fully understood, but we and others have shown that dysfunctions in brainstem control of thalamic circuits (22), in intracortical lateral inhibitory circuits (23), and in the mechanisms of synaptic plasticity (24) may play a role. Complementary to these previous studies based on unimodal sensory stimuli, the present study adds evidence that processing of bimodal sensory stimulation also differs between MO patients and healthy subjects, which may help to understand more comprehensively the mechanisms behind the abnormal sensory processing in migraine between attacks.
It has been shown that the primary somatosensory cortex (S1) is not only responsible for processing the somatic sensory stimuli, but also for encoding and storing visual information during working memory, suggesting a potential bimodal contribution to memory (25). In fact, when one interferes with S1 activity by applying single pulses of transcranial magnetic stimulation (TMS) during a visuo-tactile cross-modal stimulation, performance in the execution of a visuo-tactile task is altered (26). By contrast, when S1 excitability is increased via high-frequency repetitive TMS, visual-tactile performance is significantly enhanced (27). This and other studies suggest that S1 is part of a larger system encoding visual memory in relation to interaction between the body and its environment. In addition, an EEG study showed that contralateral somatosensory delayed activity, a function of working memory, selectively increases during body-related visual stimuli and in proportion to the number of repetitions (28). Habituation of cortical responses to sensory stimuli we assessed in our study is considered a basic form of learning and memory; it offers insight into the short- and long-term depression/potentiation adaptive plastic mechanisms at the synaptic level and into the related changes in cortical excitability or pre-activation levels (24,29). Interestingly, since associative long-term potentiation – another form of a learning process – can be induced in S1 by pairing visual and tactile stimuli, it was argued that cross-modal mechanisms promote visual-induced associative synaptic plasticity in the parietal cortex (30).
In accordance with the above-mentioned studies, the simultaneous somato-visual stimulation did not change the basal cortical activation level in HV, but induced a delayed increment of SSEP amplitude; that is, a loss of habituation. On the contrary, in MO patients recorded between attacks, who at baseline already had a deficient habituation, the bimodal stimulation caused an amplitude decrement between the first and second blocks of SSEP; that is, habituation. We speculate that the different effects of simultaneous visuo-somatosensory stimulation in migraine could reflect an abnormal mechanism of visual-dependent synaptic plasticity in the parietal cortex, which probably regulates the learning phenomenon of habituation. Moreover, we suggest that the response difference between the two subject groups is due to a lower level of thalamo-cortical activation at baseline in MO patients than in HV.
In parallel to the changes in LF-SSEP, bimodal stimulation in MO patients significantly increased early SSEP HFO that were lower at baseline compared to HV but reached an amplitude comparable to that of HV during the visual stimulation. This contrasted with the absence of a significant change in HFO, and thus thalamocortical activity, in HV. Both habituation and thalamocortical activity returned to basal levels 5 min after the bimodal stimulation in both groups. The fact that the bimodal stimulation significantly modified cortical LF-SSEP but had no effect on the cortical (late) component of HFO supports the assumption that the generators for these two cortical activities are different (31).
Taken together, these results suggests that multisensory integration is impaired in migraine without aura between attacks because of malfunctioning thalamo-cortical networks. Animal experiments have shown that early convergence of diverse sensory inputs occurs at the level of the thalamus, although with some inter-modality differences. Increased sensory evoked activity between the ventroposteromedial nucleus (VPM) and S1, but not between the dorsal lateral geniculate nucleus and V1, was observed immediately after simultaneous visual and somatosensory stimuli (32–34). Neurons responding to stimuli of different modalities were also identified in the medulla oblongata (35) and the thalamic reticular nucleus (36), both structures in close relationship with dorsal thalamic nuclei and thalamocortical circuits.
At the cortical level, although multisensory integration is the result of both excitatory glutamatergic cells and inhibitory neurons (37), the former seem to prevail (34). Since glutamate is the most important excitatory neurotransmitter in thalamocortical loops (38), we propose that the increase in thalamocortical activity observed in migraine patients during bimodal stimulation results in an increased activation of inhibitory circuits that determine a progressive decrease of the cortical response to repeated stimuli; that is, habituation. On the contrary, in healthy subjects where thalamocortical activity and thus glutamatergic tone are already maximal at the baseline, the bimodal stimulation triggers a homeostatic mechanism that aims at reducing the excitatory tone and hence allows an increase of cortical responses (39). This mechanism could occur at the level of the brainstem, of the thalamic and/or reticular nuclei that control the dorsal thalamic nuclei.
Since, as mentioned above, the process of multisensory integration also depends in part on the integrity of inhibitory neurons (37), we cannot exclude that in HVs concomitant stimulation might induce a progressive transient somatosensory non-inhibition leading to an increase in the initial response; that is, a habituation deficit. In patients, on the other hand, where an initial deficit of cortical inhibitory mechanisms may exist (40), progressive paradoxical inhibitory responses occur, resulting in normal habituation of the SSEP. Similar paradoxical responses to external modulatory interventions have previously been observed in migraineurs in both the visual (41) and sensorimotor systems (42,43).
Abnormalities in sensory integration processes were reported previously in migraine, although with sensory modalities and stimulation paradigms different from ours. Ambrosini et al. (44) studied intensity-dependence of auditory-evoked cortical potentials (IDAP) during continuous flash-light stimulation. While during visual stimulation the IDAP amplitude-stimulus function (ASF) slope significantly decreased in healthy subjects, there was no effect in the total group of migraine patients. However, when patients with a normal ASF slope at baseline were compared to those who had a steeper ASF slope, the light stimulation significantly decreased the ASF slope in the latter (called “reducers”) but increased it in the former (“augmenters”), suggesting that its effect depends on the cortical activation level at baseline (44). If one accepts that increased intensity dependence of auditory potentials is mediated chiefly by a deficient habituation of the responses to the high intensity stimuli (45), our results would be in line with those found in the “reducers” subgroup. Using a sound-induced flash illusion paradigm, reduced or abolished perception of multiple flashes was found in migraine with aura patients, especially during an attack (46). This could not be modulated by inhibitory neurostimulation of the visual cortex, which led the authors to postulate a subcortical contribution (47). Abnormalities in multisensory integration were also detected in migraine by pairing somatosensory with motor stimuli using the paired associative stimulation or short-latency afferent inhibition techniques (43,48,49), in one study as a function of thalamocortical activity (43).
Finally, we must note as a limitation of the study not to have analysed visual evoked potentials simultaneously with SSEPs, at least during the concomitant stimulation. This would probably have allowed a more accurate interpretation of the results.
Conclusions
Confirming clinical observations (6) and neuroimaging studies (15), our electrophysiological results show that abnormal sensory processing in migraine is not limited to one sensory modality but also involves multisensory integration. Further studies are necessary to determine for which and for how many sensory modalities this multisensory integration is most impaired in migraine. In addition, studies using bimodal stimulation are needed in different phases of the migraine cycle, such as during an attack and in chronic migraine, since this offers a unique opportunity to investigate defensive strategies against multisensory overload under conditions when baseline habituation and thalamocortical activation have returned to normal levels (50) while multisensory hypersensitivity is clinically obvious. Finally, it would be highly interesting to investigate whether repetitive daily bimodal stimulation, by normalising thalamo-cortical network activity, could induce durable brain changes and reduce migraine attack frequency, as already observed with bimodal auditory stimulation in tinnitus, another functional brain disorder (51).
Article highlights
Bimodal somato-visual stimulation significantly reduced SSEP habituation and tended to reduce thalamocortical activation in heathy volunteers. The same stimulation significantly increased SSEP habituation and thalamocortical activation in migraine interictally. These data suggest that abnormal sensory processing in migraine is not limited to one sensory modality but also involves multisensory integration.
Footnotes
Acknowledgments
The contribution of the G.B. Bietti Foundation in this paper was supported by the Italian Ministry of Health and Fondazione Roma.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.