
Abstract
Background
Mobile health apps have the potential to promote adherence to headache management through the use of evidence-based behavior change techniques (e.g., self-monitoring). While many headache management apps exist, the extent to which these apps include behavior change techniques remains unknown. Thus, the present study systematically evaluated the content and quality of commercially available headache management apps.
Methods
Headache apps were identified using a systematic search in the Apple App and Google Play stores. A total of 55 apps were evaluated using the taxonomy of behavior change techniques and app quality using the Mobile App Rating Scale.
Results
Headache management apps included 0–14 behavior change techniques (Mean [M] = 5.89) and 0–8 headache management behavior change techniques (M = 4.29). App quality ranged from 2.84–4.67 (M = 3.73) out of 5.00. Three apps, Migraine Trainer, Easeday: Headache & Migraine, and PainScale, included the highest number of overall and headache management behavior change techniques along with good quality scores.
Conclusions
While randomized controlled trials are necessary to determine the efficacy of individual headache apps, most existing apps include evidence-based headache management behavior change techniques. Headache apps often focus on either self-monitoring or stress management via relaxation training, suggesting that patients’ needs should be used to inform app selection.
Introduction
Recurrent headache, such as migraine, is a leading cause of disability that affects approximately 1 in 5 Americans (1). Effective headache management includes a combination of pharmacological therapy, biobehavioral interventions (e.g., relaxation, biofeedback), and adherence to healthy habits (e.g., adequate hydration, sufficient sleep, healthy diet, reducing caffeine consumption, and regular exercise) (2,3). Despite strong evidence for preventative, interdisciplinary care for headache management (4,5), effective treatments are underutilized due to significant barriers to care, including limited access to comprehensive health care, costs, and competing demands (e.g., school, work, childcare) (1.6–8).
Mobile health (mHealth) apps have the potential to provide several advantages for delivering interdisciplinary care for headache management including increased accessibility, enhanced patient-provider communication, support of headache management and education, symptom monitoring, and potential reductions in health care costs (9–12). Given that effective headache management requires a multimodal approach (13), mHealth apps have the potential to promote successful engagement in treatment. However, while many headache management apps are currently available, no guidelines exist on how patients and providers can identify high-quality, user-friendly, and evidence-based apps to best support their headache management needs.
Behavior change techniques (BCTs) are specific, evidence-based intervention components that are associated with increased treatment effectiveness, such as self-monitoring, goal-setting, and personalized feedback (14,15). This taxonomy includes 26 BCTs and has been used to systematically evaluate a number of technology-based self-management interventions across a number of chronic illness populations (16–20) as it provides a structure to reliably identify evidence-based techniques associated with treatment effectiveness (14). Given that mHealth apps have the potential to promote engagement in headache management through the use of BCTs, there is a critical need to understand the extent to which evidence-based behavior change components have been translated to headache management apps. The purpose of the current study is to systematically evaluate the content and quality of commercially available headache management apps using BCTs. Aims of this study include 1) systematically evaluate BCTs of free headache management apps available in the Apple App and the Google Play stores for both Apple iOS and Android devices, (2) evaluate the quality of headache management apps using a validated rating system (Mobile Application Rating System [MARS]) (21) and 3) provide recommendations for effective headache management apps based on BCTs and usability (Figure 1).
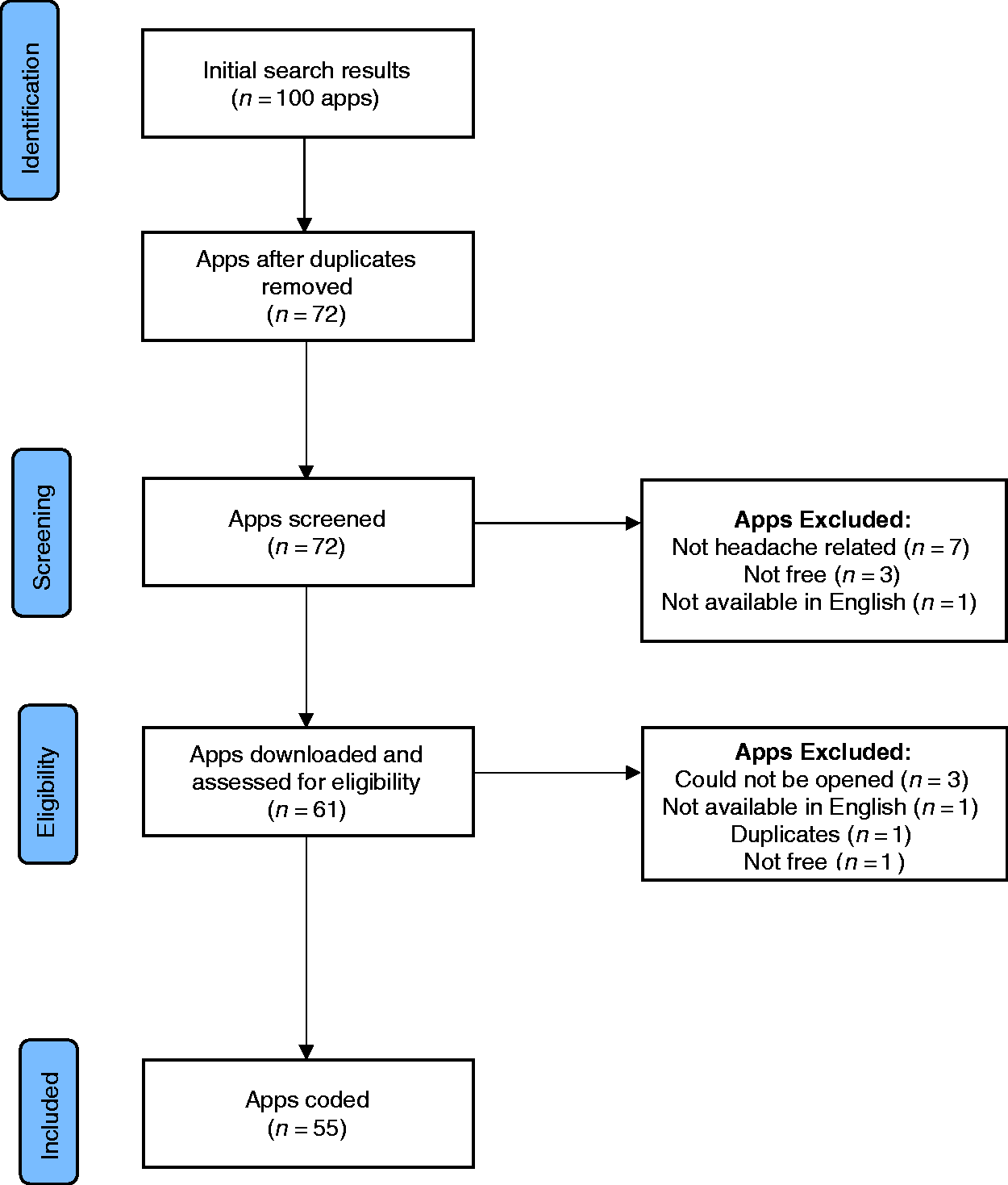
App search results.
Method
Identification of headache-specific BCTs and coding manual training
A review of the headache management literature was conducted to identify headache management BCTs. The search examined PubMed, PsycINFO, and Cochrane Library databases. Inclusion criteria included: 1) a sample of individuals with headache or migraine, 2) examination or review of interventions or BCTs for headache management, and 3) published in English. Dissertations, abstracts, and unpublished data were excluded from the review. Search terms included headache OR migraine AND “behavior change techniques” OR BCTs; headache OR migraine AND “behavior change.” See supplemental file for full search strategy and flow diagram of articles identified, screened, and included.
The first author reviewed abstract and full text articles from the search and abstracted information regarding evidence-based headache management BCTs. The reference sections of included articles were also reviewed to identify additional articles for inclusion. Results of the literature review identified 21 articles for inclusion with 19 intervention studies and 2 systematic reviews (see Supplemental Figure 1). Findings from this review were discussed with a team of experts in headache management BCTs to arrive at consensus.
Nine of the 26 BCTs have consistently demonstrated efficacy in improving headache outcomes and subsequently been recommended for use in headache management interventions (22–24). These nine BCTs are herein referred to as “headache management BCTs” and include: 1) behavior-health link, psychoeducation about the relationship between an identified behavior and the user’s health; 2) consequences, psychoeducation that includes informing the user of the likely outcome of engaging and not engaging in the target health behavior; 3) instruction, provides the user with information on how to perform the target health behavior or preparatory behaviors; 4) prompt intention formation, involves encouraging the user to set a general goal that moves them towards the target health behavior; 5) prompt specific goal setting, includes detailed planning of a specific goal (e.g., frequency, intensity, duration) and identification of a strategy to increase practice and mastery of the behavior change (e.g., where, when, how or with whom); 6) self-monitoring, the tracking of a behavior to promote accountability and identification of facilitators and barriers; 7) feedback, providing data about a tracked behavior or discrepancy about a goal; 8) social support/change, prompts the user to consider how others might change their behavior to support their behavior change goal; and 9) stress management, relaxation training to reduce tension, stress, and anxiety in order to facilitate achievement of their proposed goal. See Supplemental Table 1 for a brief description of all 26 BCTs and Abraham and Michie (14) for a thorough review of their taxonomy of BCTs along with each individual BCT.
Three raters received approximately six hours of training on the adapted Abraham and Michie (14) coding manual on BCTs for mHealth coding (see Ref. 25 for manual development). The senior author, who has extensive experience coding BCTs, led BCTs coding training sessions. Raters included doctorate level behavioral scientists with an existing understanding of BCTs. Initial training consisted of a review of BCTs to clarify differences between techniques. Raters then coded two commonly used mHealth apps. Coding required raters to first read and code the entire description of the app from the Apple App or Google Play stores. In line with previous studies that have utilized this protocol (19,21,25–27), raters downloaded and interacted with the app for a minimum of 10 minutes. Next, raters coded for the presence or absence of all 26 BCTs. Raters then met with the senior author to discuss discrepancies and reach consensus on BCT ratings. Finally, raters coded four headache or pain management apps using the same procedure.
Identification of mHealth apps for headache management
Four systematic searches were conducted to identify mHealth apps for headache management in December 2020. First, the term “headache” was searched for in the Apple App and Google Play stores. A list of the first 25 apps for each of the searches was recorded given that previous reviews have estimated that a typical consumer considers, at most, the first 25 results when searching for an app (19,25,26). The second term “migraine” was searched for in the Apple App and Google Play stores, and the first 25 apps from each of the searches was recorded. Apps were excluded if they (1) had an associated cost to download, (2) were not related to headache, or (3) were not in English. Apps from all of the searches were combined into a master list and duplicates were excluded. The free basic version of all apps were coded; any app features that required an in-app purchase were not coded.
Using BCTs and MARS to code headache management apps
Included apps were divided among three raters and each app was coded for the presence or absence of all 26 BCTs. Raters also completed quality ratings for each app using the Mobile App Rating Scale (MARS), a 23-item measure designed to assess the quality of mHealth apps across five domains: Engagement, Functionality, Aesthetics, Information, and Subjective Quality (21). Each domain contains between three and seven items rated on a 5-point scale ranging from 1 (Inadequate) to 5 (Excellent). The mean of item responses for each domain was calculated to obtain Engagement, Functionality, Aesthetics, Information, and Subjective Quality subscale scores. In addition, an overall quality score was calculated by taking the mean of items from the first four subscales.
Assessment of interrater reliability
To assess reliability of the coding system and rater agreement, 20% of the apps were randomly selected to be double coded using the BCT manual and the MARS (n = 12). Interrater reliability was calculated using percent agreement between coders on the 26 BCTs for the 12 apps that were double coded. Agreement between raters on the MARS was assessed by calculating the intraclass correlation coefficients (ICCs).
Results
Initial searches identified 100 apps related to “headache” and “migraine.” Of these, 39 apps were removed for the following reasons: 28 were duplicates, seven were not specific to headache, three had an associated cost, and one was non-English. Of the 61 apps that were downloaded, three apps were removed because they could not be opened/used and one was non-English. One additional duplicate was identified due to a slight variation in the app titles across devices. One app was removed because the free headache content was limited to a 29 second audio introduction. This resulted in 55 apps being downloaded and coded. Nineteen apps were available on both Android and iOS platforms while an additional 16 were only available on iOS and 20 on Android. Table 1 includes a complete list of included apps and the included BCTs in each app.
Behavioral Change Techniques (BCTs) Used in Coded Apps.

Note. “**” denotes pain management BCTs; the 3 BCTs not included in the table were not found in any of the apps reviewed.
Each of the apps utilized between 0 and 14 BCTs (MBCT = 5.89) and 0 and 8 headache management BCTs (i.e., behavior-health link, consequences, instruction, prompt intention formation, prompt specific goal setting, self-monitoring, feedback, social support/change, and stress management; MHABCT = 4.29). Twenty-four percent of the apps used at least six headache management BCTs while 45% used at least five headache management BCTs. The most commonly used BCTs were behavior-health link, feedback, self-monitoring, instruction, consequences, others’ approval, and prompt intention formation, all of which are headache management BCTs (except others’ approval).
The use of behavior-health link was found in 73% (n = 40) of the apps and provided information about the relationship between a behavior and health (e.g., psychoeducation on the relationship between hydration and headache). Self-monitoring and feedback allowed for digital tracking of headache frequency or use of a headache management intervention such as medication or relaxation and information regarding patterns in these data and were found in 69% (n = 38) and 73% (n = 40) of apps, respectively. The use of instruction was found in 67% (n = 37) of the apps and provided text, graphics, or videos to teach the user how to perform a headache management behavior such as progressive muscle relaxation. Sixty-seven percent (n = 37) of apps provided information on consequences or the pros/cons of engaging in a headache management behavior (e.g., engaging in relaxation can reduce headache severity or frequency). Prompt intention formation, which includes setting a general goal such as encouraging the use of relaxation as a daily practice, was found in 51% (n = 28) of the apps. The only commonly used BCTs that was not identified as a headache management BCT, others’ approval, was included in 53% (n = 29) of the apps and allowed the user to send data to a health care provider.
When examining specific apps, three apps had the most overall BCTs (i.e., PainScale [n = 14], Easeday: Headache & Migraine [n = 11], and Migraine Trainer [n = 10]) and the most headache management BCTs (i.e., PainScale [n = 8], Easeday: Headache & Migraine [n = 7], and Migraine Trainer [n = 7]). All three of these apps, PainScale, Easeday: Headache & Migraine, and Migraine Trainer, included the headache management BCTs of behavior-health link, consequences, prompt intention formation, instruction, self-monitoring, feedback, and stress management. PainScale also included social support/change (headache management BCT) which includes the provision of support or a “buddy” system for engaging in headache management skills and social comparison. PainScale and Migraine Trainer both included others’ approval, while Easeday: Headache & Migraine and Migraine Trainer included the use of provide contingent rewards and prompt practice BCTs.
The overall quality of headache management apps ranged from 2.84–4.67 (MMARSoverall = 3.73) out of 5.00. Seventeen apps had an overall quality score of 4 or higher and 16 additional apps had a MARS overall quality score between 3.50 and 3.99. Subscales scores ranged from 1.33 to 5.00 and can be found in Table 2.
Mean Scores for MARS Subscales.

Note. aThese apps were rated by multiple coders and their average scores on the MARS were used. MARS scores range from 1 (Inadequate) to 5 (Excellent). MARS descriptors bfor age: Children (under 12), Adolescents (13–17), Young Adults (18–25), Adults, General. c“App Store Ratings” are subjective user ratings found in the app store that range from 1 to 5 stars. Two apps randomly selected for double-coding are not included in the table because they were elminated after being downloaded due to limited free content and needing an access code to use.
Percent agreement was ≥90% for 20 of BCT classifications. Percent agreement was 83% for prompt barrier identification, instruction, and provide contingent rewards, 75% for prompt intention formation, and 58% for provide general information on behavior-health link and provide information on consequences. ICCs for the MARS scales were all in the good to excellent range: MARS A: Engagement = .94, MARS B: Functionality = .86, MARS C: Aesthetics = .89, MARS D: Information = .92, and MARS Overall App Quality = .92 (21).
Discussion
The current review fills a gap in the extant literature by providing an evaluation of the BCTs and quality of headache management apps, which can serve as a resource for health care providers for making informed recommendations to patients with headache. Fifty-five apps were evaluated with each app included having between 0 and 14 BCTs and 0 and 8 headache management BCTs and an overall MARS quality rating ranging from poor to excellent. The primary focus of the majority of apps was self-monitoring including headache characteristics (e.g., frequency, severity) along with associated symptoms, triggers, and self-management behaviors (e.g., PainScale; Migraine Buddy; Migraine Trainer) whereas, a minority of apps focused on stress management (e.g., relaxation training) (e.g., Easeday: Headache and Migraine; Breathescape). Despite the wide range of content and quality of headache apps, the findings provide promise regarding content and quality of several of the top-rated headache apps.
Nearly all of the commonly used BCTs were headache management BCTs (i.e., behavior-health link, self-monitoring, feedback, instruction, consequences, and prompt intention formation) suggesting that developers of headache management apps have integrated evidence-based headache management strategies into their apps. The translation of headache management BCTs into mHealth platforms shows promise for addressing access barriers as it provides a more accessible and lower cost alternative for delivering evidence-based headache management techniques. For instance, incorporating education and the associated consequences of stress management on headache severity, along with a platform to practice different forms of relaxation (e.g., diaphragmatic breathing, progressive muscle relaxation), allows patients to readily access this tool at the first sign of headache (e.g., Easeday: Headache and Migraine; Breathescape). Another advantage is the ability to self-monitor and receive feedback about headaches and associated symptoms and triggers in real time, which may help patients with identifying behavior patterns that increase their risk of having a headache (e.g., poor hydration and sleep habits) (e.g., PainScale; Migraine Buddy; Migraine Trainer). The only commonly used BCT that was not headache management specific was others’ approval, which most often included the ability to share self-monitoring data with others via email or other messaging platforms (e.g., PainScale; Migraine Buddy; Migraine Trainer). Initial evidence for the use of others’ approval in headache treatment suggests that sharing self-monitoring data with providers may help to inform treatment recommendations (28,29).
Several of the headache management BCTs have not yet been frequently incorporated in commercially available headache management apps (i.e., prompt specific goal-setting, social support/change, and stress management). Effective headache management is often challenging for patients to adhere to as it includes a multimodal treatment approach (e.g., biobehavioral intervention such as relaxation training and adherence to medication and healthy habits) (13). Because of the need for a multimodal treatment approach, it is important that patients understand the link and associated consequences between engagement in each of the headache management strategies and headache outcomes (behavior-health link, consequences) (e.g., Migraine Trainer; Curable), are able to set informed general goals to improve their health (prompt intention formation) (e.g., PainScale; Easeday: Headache and Migraine; Migraine Trainer), and have a system for tracking and receiving feedback about their progress (self-monitoring, feedback) (e.g., PainScale; Migraine Trainer). These skills, however, are more likely to lead to sustained behavior change when implemented alongside specific, measureable goals (specific goal setting) and with the support and accountability of others (social support/change) (e.g., PainScale) (30-33). One approach to implementing specific goal setting into future iterations of existing or new apps would be to have users set specific goals after identifying general goals. For instance, if a user identifies a general goal of “practice relaxation” the app could then prompt the user to identify the frequency (e.g., 5 times per week), duration (e.g., 10 minutes each day), location (e.g., in bed), timing (e.g., before going to sleep), along with how (e.g., using app with guided meditation) and with whom they intend to practice relaxation (14). Prompting the user to further define the behavior change goal and to identify specific, measureable steps for engaging in the behavior will help set the user up for success. Headache management apps could also be improved by providing a platform that facilitates opportunities for social support or psychoeducation on the benefits of having supportive relationships for self-management (30-32).
Stress management was another BCT that was not widely utilized, appearing in just one in four headache management apps (e.g., Easeday: Headache and Migraine; Breathescape; Woebot). Stress management, such as the use of relaxation skills (e.g., diaphragmatic breathing), is a central element of headache treatment that has been shown to be an efficacious evidence‐based intervention for patients with headaches (22,34). While stress management was not among the most commonly used BCTs, when it was included in an app it was often the primary focus of the app. Indeed, of the apps with the highest number of headache management BCTs (i.e., ≥six headache management BCTs), the majority of apps focused on either self-monitoring of headaches and headache management behaviors (73% of apps) or stress management in the context of relaxation training (18% of apps). Whereas, a small proportion (9% of apps) did not appear to have a specific focus and included elements of stress management, self-monitoring, as well as psychoeducation. While self-monitoring and stress-management are both evidence-based strategies used in traditional clinic-based headache treatment, these findings suggest that it will be beneficial for health care providers to carefully consider individual patient needs when recommending an app to support treatment and to select an app with a dual focus on stress management and self-monitoring or to select an app with the focus that is best for a particular patient. For example, a provider may recommend use of a stress management app for patients that are unable to attend clinic-based relaxation training due to access barriers (e.g., transportation, insurance). Conversely, a provider may recommend an app that focuses on self-monitoring and allows for sharing of these data (i.e., others’ approval) for patients that could benefit from increased accountability for adhering to their treatment or when additional data is needed to better understand associations between patient behavior patterns and headache outcomes (e.g., headache frequency, severity, onset).
Health care providers recognize the benefits of apps for supporting headache treatment with the “prescribability” of apps becoming an important topic of conversation among stakeholders (35,36). While randomized controlled trials (RCTs) are needed to examine the efficacy of headache management apps, and are necessary to determine true prescribability, identifying evidence-based BCTs available within headache management apps provides an interim validation process to aid providers and patients in making informed app selection decisions. Based on the current evaluation of BCTs and app quality, Migraine Trainer, Easeday: Headache and Migraine, and PainScale included the most headache management BCTs along with high quality ratings. Therefore, suggesting that these three apps incorporated the most behavioral strategies that have been shown to directly improve headache management and outcomes (28,29) and are likely to be engaging for user.
Migraine Trainer was developed specifically for patients with a diagnosis of migraine and utilized seven of the headache management BCTs. The app contains various features, including use of an individual migraine management plan, opportunities for self-monitoring, teaching of stress management skills, and psychoeducation. Migraine Trainer may be particularly useful for older adolescents and emerging adult populations as they begin to assume more responsibility of their migraine treatment because features such as the use of an individual migraine management plan could help guide and support engagement in their headache treatment. Easeday: Headache and Migraine, which included a total of seven headache management BCTs, was developed for a headache population and may be especially useful for patients seeking additional support with stress management in the form of relaxation training. While, both PainScale and Migraine Trainer included either psychoeducation or a brief introduction to relaxation training, Easeday: Headache and Migraine is unique in that it provided extensive training and opportunities for practicing relaxation skills. Specifically, the app includes use of biofeedback as well as numerous relaxation scripts and audio files for practice of diaphragmatic breathing, progressive muscle relaxation, and mindfulness. Finally, PainScale was developed for a general chronic pain population and included eight headache management BCTs. This app may be particularly useful for patients in need of a comprehensive daily dairy for self-monitoring headaches, symptoms, triggers, and self-management behaviors that can be synthesized and shared with a provider (12). PainScale may also be a good option for patients in need of additional social support.
The current study has a number of strengths, including use of a systematic search strategy and application of BCT taxonomy to characterize the content of commercially available headache app. Despite these strengths, there are several limitations. First, this systematic evaluation does not provide a comprehensive review of all headache management apps. The search strategy used captures only the most commonly downloaded apps (i.e., the first 25 apps from each of the four search terms) and excluded apps that were not available in English or had an associated cost to download. While it may be a concern that apps that were not included, particularly those with an affiliated cost that may include more BCTs and be of higher quality, if users are not accessing these apps the improved quality is of little consequence. However in consideration of this concern, we coded the pay-to-use apps identified through our initial search and found that these apps included fewer BCTs and lower MARS quality scores than the average free apps. Thus, suggesting that not only are the currently available pay-to-use headache management apps not accessible to all patients, but these apps also do not include more evidence-based strategies and are not of higher quality. Second, apps were not used for an extended period of time and no in-app purchases were made, therefore, it is possible that certain features (e.g., providing feedback about the user’s performance on goal after a week; features with an associated cost) may not have been apparent to coders. However, this approach aligns with previous studies utilizing this protocol and provides important information for making app recommendations (19,21,25–27). Third, coding of percent agreement was low for two BCTs (i.e., behavior-health link and provide information on consequences); however, consensus was reached for those in disagreement. Fourth, while our use of the MARS engagement subscale provides the most rigorous professional assessment of app engagement currently available (21), recent research highlights a need for more rigorous reporting standards regarding indicators of app user engagement (37). If established, future studies should reassess headache management apps using these standards. Finally, none of the apps included have been tested in RCTs, thus recommendations are not based on the efficacy of the app for improving headache outcomes. Future studies evaluating the effectiveness of headache management apps is a critical next step.
This review assessed the quality and use of BCTs in commercially available headache management apps and may be used as an initial guide for making app recommendations to support headache management behaviors. The proliferation and patient interest in using health apps to support disease management highlights the need for health care providers to be informed on the types of apps available and how they can be used to support and inform their patients individual treatment needs (38). Optimal headache management apps include the use of behavior-health link, consequences, instruction, prompt intention formation, self-monitoring, feedback, stress management, prompt specific goal setting, and social support/change. Currently available headache management apps that include many of these BCTs along with high quality ratings include Migraine Trainer, Easeday: Headache and Migraine, and PainScale. While all three of these apps included a high number of headache BCTs, each had a different focus, suggesting the providers should consider the unique needs of the patient when making recommendations. Providers are encouraged to familiarize themselves with these and other apps being utilized by their patients. Future studies should continue to reassess headache apps to provide updated recommendations and assess the efficacy of headache management apps in RCTs.
Article highlights
The majority of commercially available headache management apps include evidence-based headache management behavior change techniques. Migraine Trainer, Easeday: Headache and Migraine, and PainScale are commercially available headache management apps that include a high number of headache management behavior change techniques as well as high quality ratings. Headache management apps often had a particular focus (e.g., self-monitoring, relaxation training), suggesting that patients’ needs should be used to inform app selection. Studies are needed to continue to reassess headache management apps to provide updated recommendations and to assess the efficacy of headache management apps in randomized controlled trials.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024211053572 - Supplemental material for A systematic evaluation of primary headache management apps leveraging behavior change techniques
Supplemental material, sj-pdf-1-cep-10.1177_03331024211053572 for A systematic evaluation of primary headache management apps leveraging behavior change techniques by Amy E Noser, Kimberly L Klages, Kaitlyn L Gamwell, Caitlin N Brammer, Kevin A Hommel and Rachelle R Ramsey in Cephalalgia
Supplemental Material
sj-pdf-2-cep-10.1177_03331024211053572 - Supplemental material for A systematic evaluation of primary headache management apps leveraging behavior change techniques
Supplemental material, sj-pdf-2-cep-10.1177_03331024211053572 for A systematic evaluation of primary headache management apps leveraging behavior change techniques by Amy E Noser, Kimberly L Klages, Kaitlyn L Gamwell, Caitlin N Brammer, Kevin A Hommel and Rachelle R Ramsey in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health (grant number NICHD T32 HD 68223-7 and NHLBI K23 HL139992).The first and senior authors’ efforts for this work were supported by a training grant and a career development award (respectively) from the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.