
Abstract
Objectives
We conducted focus groups in people who had participated in mobile health (mHealth) studies of behavioral interventions for migraine to better understand: (a) Participant experience in the recruitment/enrollment process; (b) participant experience during the studies themselves; (c) ideas for improving participant experience for future studies.
Methods
We conducted four focus groups in people who had agreed to participate in one of three studies involving mHealth and behavioral therapy for migraine. Inclusion criteria were being age 18–80, owning a smartphone, and having four or more headache days per month. All participants met the International Classification of Headache Disorders third edition beta version criteria for migraine. Exclusion criteria were not speaking English and having had behavioral therapy for migraine in the past year. Focus groups were audio recorded, fully transcribed and coded using general thematic analysis.
Results
The 12 focus group participants had a mean age of 45 ± 15, a mean age of headache onset of 21 ± 13 and mean MIDAS disability score was 39 ± 56. Participants were women (100%), white (50%), Asian (33.3%) or members of other racial groups (16.7%). Certain themes emerged from each topic area. With regard to recruitment/enrollment (a), key themes were: (i) Participants joined their study out of an interest in research and/or a desire to try a new migraine treatment modality (behavioral therapy). (ii) Enrollment should be simple and study requirements should be carefully explained prior to enrollment. When asked about their experiences during the studies (b), the following themes emerged: (i) It is difficult to participate in study follow-up and compliance phone calls; (ii) participants prefer to choose from among various options for contact with the study team; (iii) there are barriers that limit app use related to migraine itself, as well as other barriers; (iv) completing diaries on a daily basis is challenging; (v) technical difficulties and uncertainties about app features limit use; (vi) being part of a research study promoted daily behavioral therapy use; (vii) progressive muscle relaxation (PMR) is enjoyable, and has a positive impact on life; (viii) behavioral therapy was a preferred treatment to reduce migraine pain. Ideas for improving study design or patient experience (c) included: (i) Increased opportunity to interact with other people with migraine would be beneficial; (ii) navigating the app and data entry should be easier; (iii) more varied methods for viewing the data and measures of adherence are needed; (iv) more information on and more varied behavioral treatment modalities would be preferred.
Conclusion
Though people with migraine are motivated to participate in mHealth and behavioral treatment studies, better communication up front about interventions as well as greater flexibility in interventions and follow-up methods are desired.
Introduction
Migraine affects over 36 million Americans and is the second most disabling condition worldwide (1). While behavioral therapies have demonstrated efficacy for migraine prevention (Level A evidence) (2), research has shown that there are barriers to patients accessing evidence-based behavioral therapies. Such barriers include the time it takes to attend behavioral therapy appointments and the cost of behavioral therapy. Mobile health platforms (mHealth) provide a patient-centered way to disseminate these treatments.
Guidelines provide expert-vetted information on the design of randomized behavioral clinical trials for headache disorders (3). Existing literature in pharmacologic treatments has typically focused on preferences related to balancing drug side effects and various efficacy targets. However, there is limited information published on migraine patients’ perspectives on migraine treatment study design including study implementation, recruitment, and data collection. Although relevant to all human subjects’ migraine treatment research, this topic is particularly germane to behavioral treatments disseminated through mHealth strategies, as patients are the key stakeholders for all stages of this research.
Patient engagement and patient-centered research are increasingly recognized as core components of effective research programs. The Patient-Centered Outcomes Research Institute (PCORI) was created as part of the Patient Protection and Affordable Care Act (2010) to fund patient-centered comparative effectiveness research. PCORI requires that the studies it funds address questions that are meaningful to patients and other stakeholders as well as measure outcomes that patients and other stakeholders find important. In addition, the Agency for Healthcare Research and Quality engages patients to help identify research areas, questions, and outcomes (4). The National Institutes of Health and funding agencies in the UK also work with patients and advocacy organizations to set research priorities (5,6).
The current study sought to describe migraine patients’ experiences during behavioral mHealth migraine treatment trials. These trials recruited participants from the settings in which migraine patients generally receive their care – the primary care setting, the neurology office and the emergency department – as research has found that the majority of people receive care for migraine outside of the neurology setting: 52.8% of all visits for migraine occurred in primary care settings, 23.2% in specialty outpatient settings, and 16.7% in emergency departments (EDs) (7). In fact, among women age 15–64, headache was the third leading cause of ED visits in every year from 2011 through 2015 and headache (ICD–9 code 784) and migraine (ICD–9 code 346) were leading end-of-visit physician-assigned diagnoses (8). Using the conceptual model on patient engagement and patient-centered research developed by Frank et al., we sought to examine (a) patients’ feedback on the recruitment process into such studies; (b) the patient experience during studies; (c) participant feedback in how they might consider study design features (9).
Methods
Participants
We conducted four focus groups with people with migraine meeting the International Classification of Headache Disorders third edition beta version (ICHD-3 beta) criteria (10). The participants were recruited from ongoing studies involving mHealth and behavioral therapy at an urban medical center. The participants had been recruited from three different ongoing feasibility/acceptability behavioral/mHealth trials taking place in the neurology, primary care and emergency departments of a large academic urban medical center. Inclusion criteria were: a) to be aged 18–80, b) to have a smartphone, c) to not have participated in behavioral therapy for migraine in the past year, d) to experience ≥ 4 headache days/month.
Recruitment for focus groups was stratified to include participants who had fully participated (66.66%) as well as those who had withdrawn from studies (33.33%), to ensure that a broad range of perspectives were included.
The behavioral intervention
The studies we evaluated had common design elements but recruited from different settings. Each study identified ICHD-3 migraine. Participants went through an informed consent process that included a description of study purpose and design. Once enrolled, participants were asked to complete a baseline questionnaire. They were asked to download the RELAXaHEAD app (11), modelled after the app used in the SMILE study, which examined smartphone based progressive muscle relaxation (PMR) for epilepsy patients (12,13) (it has the same PMR used in that study) and the Human Epilepsy Project (HEP) app (14). The RELAXaHEAD app is compatible with both the Apple iOS and Google Android systems. There is an ∼5-minute PMR session and an ∼15-minute PMR session embedded in the app. For the RELAXaHEAD app, modifications were based on input from migraine patients and headache specialists using methods described elsewhere (11). Our RELAXaHEAD app has back-end analytics built in to record the amount of time spent playing the PMR. Patients were asked to track their headache attacks, medication intake/side effects, and sleep on a daily basis in addition to completing two PMR sessions. Participants could also access a diary feature that allowed for free-text notations to add qualitative information about their headaches and triggers. There were reminders sent out by the app at a fixed time daily (they were supposed to have been delivered at the same time daily, but some phones allow the app reminder feature to be disabled). Participants were asked to use the app daily for 90 days; they were asked to enter diary data and to perform PMR using the app for 20 minutes/day.
Participants were shown how to use the app, and were then asked during the enrollment to input some data. Participants were given the rationale for PMR and were asked to practice it once in the office. The rationale was: “Relaxation will help you learn to control physical arousal and thus help prevent headaches. Research has shown that learning relaxation leads to fewer and less intense headaches for most migraine and tension-type headache patients so long as they regularly use and practice their skills” (15). Patients were instructed that PMR would walk them through a specific set of procedures to learn how to tense and release various muscle groups throughout the body. All participants completed a full PMR session during the enrollment. Also, some participants were given study cards about the different aspects of the study procedures.
Of note, at the onset of the study, patients were told that they would be contacted once a month for a brief follow-up. It was sometimes hard to call at the exact preferred times, but we made every effort to reach participants, making calls outside of business hours (evenings and weekends). Investigators could also monitor non-compliance. There were protocol changes made after some initial study participants enrolled; for example, compliance calls for every 3 days of missing data were not part of the original protocol.
Focus group procedures
Participants were invited to participate in the focus group as follows: As stated above, there were three mHealth-related studies using the RELAXaHEAD app. These studies differed from each other in that they recruited participants from different settings in which people with migraine present for care. In total, there were 21 participants invited from a study conducted of patients with migraine who had visited primary care, 39 participants invited from a study of patients with migraine who had visited the neurology office and 61 participants who were contacted from an ongoing emergency department study. The patients recruited from the primary care and neurology settings had been the initial participants to enroll in the RELAXaHEAD studies and complete the 6-month study period. In contrast, all 61 of the ED participants who had been enrolled in the ED mHealth study were invited to participate no matter whether or not the 6-month study period had passed. A research coordinator called the participants up to five times to invite them to participate. If they could not be reached, an email invitation was sent to them. Participants were compensated with $50–75 in the form of an Amazon gift card. All 61 patients recruited from the Emergency Department were contacted to participate in the focus group. Twenty-one of the enrolled primary care patients and 39 of the enrolled neurology patients were contacted.
Focus groups were conducted as follows (as detailed by the COREQ checklist): The groups were led by MTM, a Board-certified neurologist with subspecialty training in both headache medicine and behavioral neurology/neuropsychiatry by the United Council of Neurologic Subspecialties. She has prior experience leading focus groups and has trained under a qualitative specialist (16,17). Prior to the focus groups, she had not met any of the attendees with the exception of one who was coincidentally her patient (by the patient’s report to the group). She explained that as the PI, she was looking to improve the way in which research studies are done in the future and welcomed both positive and negative feedback in an effort to improve the patient experience in future studies. The focus groups were also attended by a research team member who transcribed and digitally recorded the session audio.
The semi-structured outline (Appendix 1) was used as a guide for leading the focus group and was developed based on the focus group template from focus groups on “helping women help themselves to improve heart health”, which were conducted by a qualitative expert Dr Victoria Dickson. She provided help on how to best structure such an outline.
At the beginning of each focus group, Dr. Minen introduced herself as a headache specialist and as the PI of the studies. She explained that the purpose of the focus groups was to learn about peoples’ experiences with the study and to gain ideas on how to improve the research experience. She asked for both positive and negative feedback. She also stated that all comments were confidential in that they should not be shared with others outside the room, and that the data from the focus groups would only be shared in aggregate form; there would be no identifying data published. No repeat interviews were carried out, and transcripts were not returned to participants for comment and/or correction.
The sessions were audio recorded, fully transcribed and coded using general thematic analysis using Atlas.ti 8 as follows: Two coders, KM and KS, were trained in coding by MTM. Each coder individually developed a list of codes for each focus group; the coders then met and resolved discrepancies. MTM provided direction on how to do this, and both coders, along with MTM, developed the themes and subthemes for the study. The coders felt that data saturation was reached after three focus groups were completed and the data was analyzed. They found consistency between the data and the findings.
Results
Participants’ demographics and headache and related characteristics.

Participants’ overall mean age was 45 ± 15, their mean age of headache onset was 21 ± 13 and their mean MIDAS disability score was 39 ± 56. Participants were women (100%), white (50%), Asian (33.3%) or members of other racial groups (16.7%). Only two (16.7%) had previously had behavioral therapy for migraine. The emergency department participants were asked if they had a physician in an office setting who treated their headaches; only one answered yes. The primary care participants were asked if they had a neurologist; all answered that they only had a primary care doctor. The codes can be found in the Supplemental Tables.
Participant experience in the recruitment/enrollment process.

Participant experience during our studies.

Ideas for improving participant experience for future studies.
Regarding the topic of recruitment/enrollment
One key theme was that patients wanted to participate because of an interest in the research or to help other migraine sufferers. Many patients expressed that they were initially excited to participate in an experimental study and, as one patient explained, what drew her into the study was some altruism: “I did want to contribute to the research, I did want to help myself and other people”.
Another key theme was that participants joined because of a desire to try a new migraine treatment modality (behavioral therapy) to reduce migraine pain. Many of the patients who joined the study were approached during a time when they were motivated to pursue treatment due to the severity of their migraines. One patient explained that “I was very excited about the idea because when I found out about the study I was having a lot of migraines, a lot of the time in the course of a month, and that’s what led me to go see a doctor to try to deal with it; rather than just band-aiding each headache, I wanted to really try to do something”. One of the appeals of behavioral therapy in particular was that it was non-pharmacologic – one patient explicitly stated that she wanted to “try to take a more holistic approach”.
Many participants were overall satisfied with the enrollment/recruitment process. However, it was felt that the enrollment should be simple and study requirements should be carefully explained prior to enrollment. One patient stated that “I felt like there were a lot of questions and we ended up sitting there for a really long time”. However, another issue during enrollment was that some patients felt liked they walked away without really understanding the requirements of the study and how to use the app. One patient said she was “not the kind of person who gleefully flips through the app and finds all the things” and thought that the person who enrolled her expected her to do just that. Another said that “I honestly don’t think I understood the responsibility that I was taking on when I enrolled in the study. The journaling, my responsibility beyond doing the relaxation things”.
Regarding the topic of migraine patient experience overall
While many patients were satisfied with the study design and thus there was a theme “agreed with the current study setup”, another theme emerged that some participants wanted the study to be less of a time commitment. The study was designed to be 6 months long with most studies having follow up calls post-enrollment after 48 hours, 1 month, 2 month, 3 months and 6 months. During the first 3 months, if a patient did not listen to the PMR or enter data into the app for three consecutive days, they were contacted by the study staff. Thus, participants recommended shortening the length of the study from 6 months to 3 months. As one patient said, “6 months is kind of scary”.
Another theme that emerged was difficulty in conducting follow ups/compliance calls via the phone. Some patients were not aware of the protocol in regard to compliance and were confused as to why or became stressed that they were receiving so many calls. One patient said that “I would get phone calls that I hadn’t recorded the information and I found it very stressful”. Oftentimes, these calls would be at inopportune times, which would lead to a lot of back and forth between the patient and study team. As one patient explained, “Phone calls would always have to be rescheduled because I would always be busy at the time”. One solution to this problem emerged as a theme to have more choices in the form of follow up/compliance contact. While some patients wanted to continue to be contacted via phone, others preferred text or email or even a follow up visit.
Many of the patients wanted the study protocol to be updated to include opportunities to interact with other migraine sufferers. One of the main reasons was because these patients feel that non-migraine sufferers do not understand the severity of their pain. One patient said that she enjoyed attending the focus group because “I like hearing other people’s stories; it is a little comforting to hear about other approaches or a shared experience”. All of these patients thought that in-person opportunities were best but acknowledged that it can be difficult to coordinate schedules; therefore, an online component could also be added.
Regarding the topic of the migraine patient experience in the studies
Another key theme was around barriers (both migraine as a barrier to using the app and non-migraine barriers to using the app) that inhibited app use. Migraine pain often limited a patient’s ability to engage with the app; one patient explained that she was frustrated because she was “having a lot of headaches at the time so my patience was limited. And it just seemed to me that each step along the way I ran into an additional obstacle”. Another patient said that it was difficult to speak on the phone whenever she had a migraine, which was why it was difficult to reach her for follow up/compliance calls. Barriers unrelated to migraine were also cited, such as discontinuing app use due to interruption in the normal schedule, other medical issues, or disinterest/forgetfulness. One patient said that she stopped using the app when she went on vacation because “I wasn’t going to take time out of my vacation, I could’ve been sitting on the beach doing it, I just wasn’t going to and then once I went back to work … I don’t have a good reason; I’d come home and do it for 5 minutes or 20 minutes but …”. Some/many participants also disliked using the phone so frequently or had concerns about sharing personal data through their mobile device.
Another theme that emerged was difficulty tracking information daily, with some participants stating that they only wanted to deal with pain days and did not want to track pain-free days. One patient explained that “I would rather do the work when I need to so I keep track of when I do have a migraine, I would write it down or do something to keep track and then I can report on that when I’m working with my doctor. But as far as doing something every single day, I would rather not do that. I would rather just deal with the pain days I think, than every single day”. One patient explained that she did not want to “spend that much time every day dealing with the fact that I am migraine sufferer”. Another patient said that “having to put information every day was tedious”, and “what started driving me crazy with the app was the journaling every day, just trying to keep track of it”. Others felt that app functionality made it difficult to complete all of the study requirements. One patient stated: “I found the program itself a little bit awkward and again I'm not technological, but it was sometimes hard to enter the information or to go from, you know, place to place or to go back, you know, if I needed to change some things so that was a little challenging for me”. App functionality also included instances when the app would drain the phone’s battery, or the app would freeze when opened.
However, some patients were interested in tracking information daily, particularly as it related to helping to identify their migraine triggers. One patient noted: “After the 5-minute meditation, I enter my sleep data, I put in all my medications, and I also start putting in notes because I am recovering from eating disorder. And I think it helps me because sometimes, if something triggers, I can go back and see what triggered my actions and what helps me. So, I’m putting in all the data so I can go back and review”.
The participants also discussed uncertainty about app features, where they did not know how to track all features on the app and were unaware of the help section or data report. For instance, one patient stated that “I didn’t understand what ‘medication side effect’ was, maybe cause the medicine that I am taking doesn’t give me side effects that I know of. Again, it feels like there was a lot of stuff”. They also noted that they sometimes ignored app notifications and were uncertain about these reminders because they felt that there were delivered inconsistently. One patient explained that the problem with the multitude of notifications was that “I get lots of notifications from different apps on my phones and I tend to generally swipe them all left and sort of ignore them”.
Many of the patients enjoyed doing the behavioral therapy and believed that it had a positive impact on their lives. One patient said she was “figuring out where the source of the headache was coming from, and this relaxation process definitely helped me do that”. Another noted that “I had a very positive experience. My migraines really decreased, to the point where I would only need the meds every two and half months, three months maybe”. Some patients noted that being a part of the research study promoted PMR use because they wanted to provide data for the study and help other migraine sufferers.
Some patients did not enjoy using the PMR, most frequently referencing the long PMR session, because they found it difficult to focus for the designated length of time; one patient said: “The 15-minute relaxation video was hard to sit through, I would start dozing off. I have trouble meditating and focusing so that could just be me, but that 5 minutes was kind of like enough”. Another noted that “It becomes particularly stressful to be there trying to force yourself to relax”. Others did not believe that the therapy would help alleviate their migraines, with one patient saying: “I think too much of me, is like; yeah, right. I get that maybe it would work but, yeah sure, it works for somebody out there, but not me”.
Regardless of whether a patient enjoyed the therapy or not, all of the patients said that they needed time in their schedules to complete the daily PMR. Patients were most often unable to do so because of family and work obligations as well as difficulty finding a quiet space. The patients who were most successful completed the PMR sessions at the same time each day. One patient said: “I think it would really work much better if we build it into our daily schedule every day and earlier in the day. At least for me, I think if I could do that before I sort of, you know, before I go and do all my variable stuff during the day, I have a morning routine. And if I could include that in the morning routine, I think that would help”.
Another barrier was that many patients stopped doing the PMR when their migraine attacks stopped. Some of the patients attributed the decrease in migraine frequency to the relaxation therapy. However, others found alternative therapies that worked better, and often quicker, for them. For instance, one patient explained that “I started this study on the exact same day that I started the Botox treatment. And the Botox was so effective after a certain period of time, I think like 3 weeks in, that I was just amazed. I started feeling like I didn’t have to rely as much on other abortive medications, or the actual headache study”.
Feedback for consideration of future mHealth/behavioral studies for migraine
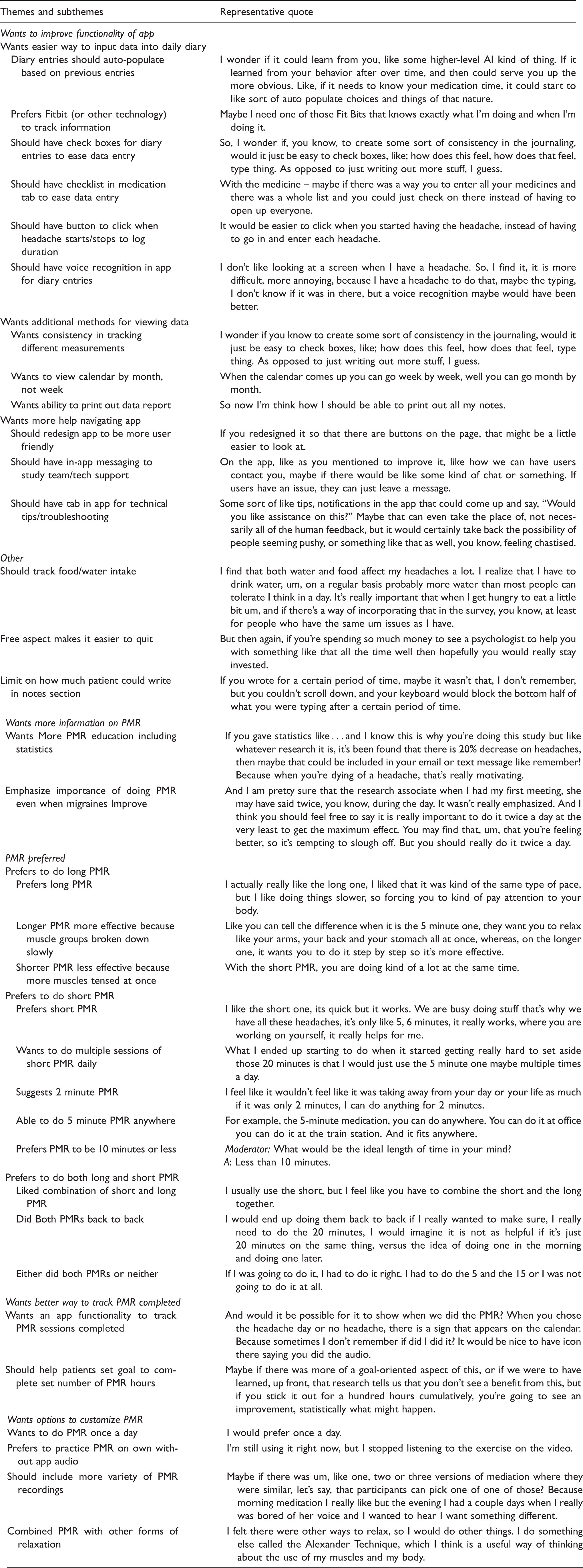
During each focus group, the participants suggested how the study could be improved based on their experiences. From an mHealth perspective, patients were most vocal about wanting to improve the functionality of the app (with regard to inputting data into the daily diary, viewing previously entered data, and navigating the app). One patient, who thought check boxes were the best way to capture this information, said: “So, I wonder if, you know, to create some sort of consistency in the journaling, would it just be easy to check boxes, like; how does this feel, how does that feel, type thing. As opposed to just writing out more stuff, I guess”. Patients had the most difficulty tracking their medications since there were multiple steps required to confirm whether or not a medication was taken; this issue led one patient to suggest, “With the medicine – maybe if there was a way [for] you to enter all your medicines and [if] there was a whole list and you could just check on there instead of having to open up every one”. More high-tech suggestions included voice recognition and auto-populating the diary based on previous entries.
Since it was difficult to track information daily, patients wanted more opportunities to reach out throughout the study with questions on how to navigate the app. One patient, who noted that she is not tech-savvy, suggested an optional in-person follow-up appointment after the initial enrollment. She explained that, for her learning style, “rather than a follow-up phone call, I think I would have done better with a follow-up visit so that I could have said, I don’t understand how to enter the medicine, or that I could have said why can’t I just enter it once if I’m taking the same drugs every night and every morning and for me, the opportunity to have a follow up visit a week later to have to opportunity to say: I don’t know how to do this, I don’t know how to do this, I don’t know how to do that, so then I could have the support, of you know, figuring out how to use the app better”. Another suggestion to help patients effectively use the app included an online chat through the app where patients could leave messages with their questions; a study team member would then respond directly through the app. One patient felt that the follow up/compliance calls, the time when most patient questions were answered, were very stressful; her solution was to include “some sort of like tips, notifications in the app that could come up and say, ‘Would you like assistance on this?’. Maybe that can even take the place of, not necessarily all of the human feedback, but it would certainly take back the possibility of people seeming pushy, or something like that as well, you know, feeling chastised”.
From a behavioral perspective, the majority of the patients had difficulty completing 20 minutes of PMR daily. Barriers included both their headaches as well as outside commitments. Most patients had an opinion on which PMR they preferred; for some patients, it was the short PMR, and they suggested doing multiple short sessions a day. One patient shared, “I remember thinking: I wish there was just a really quick one, just like 2 minutes. One, two, three, just go through the steps and listen to that and be done with it”. However, other patients preferred the long one, and several liked that there was variety in that they had both long and short PMR options in the app. Additionally, participants thought that the PMR recordings became repetitive after a few weeks and wanted options to customize the PMR in order to remain engaged; as a possible solution, one patient said: “Maybe if there was um, like one, two or three versions of meditation where they were similar, let’s say, that participants can pick one of one of those? Because morning meditation I really like but the evening I had a couple days when I really was bored of her voice and I wanted to hear I want something different”. Another barrier that inhibited patients from completing the daily PMR was if they forgot whether or not they had already done so that day. Therefore, patients wanted a better way to track PMR completed on the app; one patient suggested a note in the diary calendar when a session was completed.
Many of the patients also felt that they were not given enough instruction on the benefits of PMR and the difference between this therapy and meditation. They wanted more information given on PMR during enrollment and reinforced throughout the study. When the moderator of the focus group asked participants if they understood how behavioral therapy was different, a majority had trouble distinguishing the two. One patient suggested providing more statistics on the impact of PMR; she said: “If you gave statistics like … and I know this is why you’re doing this study but like whatever research it is, it’s been found that there is 20% decrease on headaches, then maybe that could be included in your email or text message like remember! Because when you’re dying of a headache, that’s really motivating”.
Discussion
This qualitative study of focus group participants previously enrolled in mHealth studies of behavioral interventions revealed several themes important for consideration of why people with migraine enroll in research studies as well as what should be considered when designing future studies. First, people enroll because they have an interest in research and/or a desire to try a new migraine treatment modality. Second, the enrollment process needs to be clear and simple, should be educational in that the purpose and any pre-existing data on the intervention be provided, and should include all study requirements in addition to expectations about compliance, barriers that might interfere with compliance, and study protocol steps in cases where compliance may be limited. Third, when designing these studies, participants prefer choice; this could be choice in how often and/or by what means follow-up or compliance calls are done, or even perhaps choice in which behavioral treatments might be done. Fourth, some people prefer to track their data daily and others do not prefer to perform daily tracking of their data. However, even if people do not like daily tracking, they may like reminders. Fifth, when using apps, the app functionality needs to be clear and any technological glitches minimized.
First, people with migraine enroll in migraine behavioral interventional studies out of an altruistic desire to improve general knowledge about migraine and treatment options for others with migraine, as well as a desire to try a new non-pharmacologic treatment modality. This is unsurprising and in line with prior research on migraine patients (18,19). This is consistent with prior qualitative research that has shown that people with migraine have difficulty adhering to abortive medications and are often interested in exploring options for managing their headaches that do not have adverse side effects.
Second, the recruitment/enrollment process needs to be simple and clear. For example, the recruitment process needs to clearly include educational information explaining the purpose or rationale of the study as well as any pre-existing evidence behind the intervention being study. In our studies, we waited until the enrollment process to give an in-depth description of the PMR rationale from the book by Smitherman et al. on headache treatments (15). Patients were instructed that PMR would walk them through a specific set of procedures to learn how to tense and release various muscle groups throughout the body. The Author Frank conceptualizes four factors common to all therapeutic experiences: Rapport, a healing setting, a treatment rationale, and a behavior in which the patient engages in order to heal (20). Aligned with this conceptualization, patients reported that the rationale was not sufficient in the current study procedures to convince them to engage in the healing behavior. Perhaps participants need to have the rationale explained early on in the recruitment process, not just in the enrollment process. It is possible that the literacy level of the educational material was too high. It is also possible that rapport was not established to support the treatment rationale in the settings from which patients were recruited. Finally, the theme of individualization continues to emerge throughout the focus groups; it is possible that the education materials were not sufficiently tailored to patient experiences, and therefore did not seem relevant to their lives and their disease. Future studies might need to address these factors.
The informed consent process might also be improved, as some focus group participants indicated that their consent may not have been fully informed, a common problem in all of medicine and medical research. Participants stated that they wanted clear information upfront on all of the study requirements. We had study cards explaining what participants should expect when enrolled in the study, but perhaps study cards such as brochures are not always accessed or safely kept for consultation at later dates. Future studies should ensure that relevant study procedures are easily accessible through study apps, so that patients may access the information at any time.
It is not surprising that some participants voiced that they were not fully aware of all of the study requirements. Informed consent documents are written, in part, as legal liability-limiting documents rather than understandable documents that let participants know exactly what to expect. Prior research shows that optimal informed consent procedures can be developed using focus group interviews with people in a target population, and that it is an iterative process to develop valid informed consents (21). Typically, prospective studies provide participants with written information about the planned study, but verbal information from a healthcare professional or researcher usually accompanies this. While the value of providing written information for informed consent is accepted, it has been found to be weak in its purpose – to truly inform participants about the research (22). This may be why other methods are sometimes used to inform study participants about the planned study (23). However, a systematic review showed that enhanced consent forms were among the most effective (24). Thus, future migraine research might use focus groups or other participatory methods to ensure that participants fully understand what is being asked of them.
In addition, since these were feasibility acceptability studies, as indicated in the methods section, there were protocol changes made after some initial study participants enrolled. At the onset of the study, patients were told that they would be contacted once a month for a brief follow-up. However, once the team realized that there were some compliance issues, patients that were non-compliant in filling out the daily diary or completing PMR were contacted after 3 days of missed data. Patients were unaware of the changes made to the protocol surrounding non-compliance, and in the focus group it became apparent that many patients felt that they were receiving too many calls, which caused them stress. Thus, to minimize compliance issues, patients should be advised from the start that compliance is an important component of the study. If patients are aware that they are being regularly tracked, they will expect to be contacted if non-compliant (25). For app-based studies, phone calls may be perceived as unnecessarily intrusive. Alternative messaging should be incorporated to monitor and improve compliance.
Our study results suggest that participants want to understand study requirements at the time of enrollment. In exploratory or pilot feasibility/acceptability studies, when protocol modifications are required, this can be challenging. The Medical Research Council’s 2000 framework for the development of complex interventions to improve health includes an exploratory trial design to address issues of optimization, acceptability and delivery of the interventions. This design permits “adaptation of the intervention, consideration of variants of the intervention, testing and refinement of delivery method or content, assessment of learning curves and implementation strategies and determining the counterfactual”. The National Center for Complementary and Integrative Health (NCCIH) also suggests the use of pilot studies to address questions of feasibility. Examples include “can the treatment(s) be delivered per protocol?” and “are the assessments too burdensome?”. Thus, in order to optimize the treatments and/or assessments, protocol changes may need to be made. A systematic review of guidance for exploratory studies found that there is little consistency in guidance regarding exploratory studies, and more specifically that there is some guidance that changes can be made for refining the intervention, but “guidance was not clear on what constituted minor versus major changes”. The authors stated that “an intervention continues to develop throughout an exploratory study, with distinctions made between ‘optimization/refinement’ (i.e. minor refinements to the intervention) versus ‘major changes’. However, the point at which changes become so substantial that movement back toward intervention development rather than forward to a full evaluation remains ambiguous”. Thus, likely on an individual study basis, researchers need to consider patient burden and patient expectation regarding the changes, and they need to consider to what extent participants should be or need to be informed of the changes.
Participants cited various types of barriers to comply with the studies, and such barriers can be divided into migraine-related barriers and non-migraine related barriers. Migraine-related barriers include not wanting to speak during an attack, thus limiting the ability to answer study related follow-up or compliance calls, not wanting to enter data during an attack, and more. The time frame for answering diaries must take into account the episodic nature of the attack and should permit the person with migraine to complete the information for a window of several hours to enhance compliance with the diary during and in between migraine attacks. Researchers should expect scheduled research visits or calls to be interrupted by unpredictable migraine attacks and should build in contingencies to ensure that rescheduling research contacts is not onerous for the participant. Also, strategies like suggesting darkened screens on phones might be helpful for people who have photophobia and want to limit screen time during attacks.
There were non-migraine related barriers as well. While the studies sought to deliver behavioral therapy via a mobile app in order to reduce the amount of time that patients needed to spend receiving treatment and eliminate the time needed to travel to and from appointments, many patients were still unable to complete the required 20 minutes of PMR daily due to outside commitments. A previous study examining the effect of CBT for pediatric migraine showed that 28% of patients approached refused to participate in behavioral therapy due to lack of time or potential stress, while only 2.8% refused to participate because they did not want to take medication (26). Many of these participants admitted that therapy was only a priority on the days when their headache attacks were severe, even though relaxation therapies are conceptualized as preventive treatment one uses daily to reduce the frequency of headache attacks. According to the Stage of Change Model, a patient must be ready and motivated in order to adhere to the study regime (27). Motivational interviewing might be an appropriate intervention to enhance motivation to change. Behavior change intervention studies should consider accepting only patients who reach the preparation or action stages of change during the enrollment visit into the study. If this is done in an effort to increase efficacy (at the expense of generalizability), steps might be taken during the recruitment process to ensure that enrolled patients are ready to make these changes. When the results are reported, there should be clear reporting of the inclusion and exclusion criteria so that readers understand the study population and any limitations regarding the generalizability.
Diary collection must be fast, easy, and unobtrusive. While some participants found the diary entries helpful for tracking headaches (2) and used the app to follow their migraine triggers (9), the majority of participants thought that this component of the study resulted in too many study requirements (13) and did not want to have to use the app daily (5). Others were unsure of how to use some of the tracking features (13), which limited their participation in the study. Thus, there are individual differences that patients report, and missing data may not be at random. While we did not ask participants about the extent of their missing diary data, difficulty in tracking daily symptoms was not limited to these studies. A previous study that used an application to track medication adherence among pediatric patients estimated that rates of error resulting in missing data ranged from 0 to 24% (28). Incentives for daily completion of diary entries must be enhanced to ensure compliance. Cues to complete the diary should be set for times the patient prefers, and reminders should occur at several points in time during the completion window.
Participants also shared ideas for how to improve app functionality. User engagement and app functionality are essential elements in smartphone diary usage. Prior research has already shown that there is limited use of apps, in that 21% of people who download an app will only use it once let alone for an extended period of time (29). In addition, there must be a way for participants to be able to report technological difficulties and thus there must be ways to troubleshoot any of these issues. In these studies, the participants could email or call the research team to report any issues and to troubleshoot, and any unresolved issues would then be reported to the app company. This was a similar process to that which was used in a recent pediatric headache diary study (28).
Prior studies also show that participants report wanting varied methods of communication with the study team. For example, for communicating study results to patients at the end of the clinical trial, most patients (80%) would like to receive this information in a letter, while others would like a presentation made by the investigator to a group of participants. On the other hand, some would like to hear about the results via a telephone call. Therefore, steps should be made to accommodate patients based on their preferences. In each instance, patients are seeking a more personalized approach (30). Our data indicate that methods of contacting the participants should be diverse and tailored to patient preferences. At the same time, we realize that choice limits the internal validity of studies. Thus, we want people to all be using the same protocol within given arms of a study. We need to consider study designs that allow for the individual differences in patients and different choices in treatment modality, without sacrificing internal validity. This is especially true because at the end of the study, if we do not have the data from participants because they were non-adherent or drop out, it affects the study’s internal validity.
In terms of the behavioral treatment itself, for those who did the PMR, they stated that the PMR exhibited a positive impact on the lives of many of the participants in a variety of ways, such as reducing headache frequency (3), determining the source of their headaches (10), or simply helping them focus (2). Patients that did not use the PMR regularly, and thus did not see these changes, often attributed their non-compliance to taking another medication that reduced their headaches (10), limited time to complete both PMRs daily (7), and redundancy of the therapy (3). A previous study examining electronic behavioral interventions for headaches shared similar problems with adherence and suggested having periodic booster sessions or involving the patient’s family in order to increase the potency of treatment (16). Patients also stated that they would have preferred to have more than two behavioral audio practices to maintain their interest. This is interesting, as most of the prior migraine behavioral treatment studies utilized a myriad of behavioral techniques, even if they were all grouped together as being cognitive behavioral therapy (31,32). Thus, patient preference in treatment selection is key. Even highly controlled studies of migraine behavioral therapy such as the study by Holroyd and colleagues included some treatment selection – participants could either choose cognitive stress management therapy or biofeedback for month 3 of the behavioral migraine management arm (31). Moreover, as stated in our prior qualitative research, “in everyday practice … there is significant patient choice about whether or when to engage in a certain migraine treatment plan”. This meta-synthesis on migraine management also revealed that patients want treatment choice (17).
Feedback received from the focus groups highlighted major barriers that patients face when they are enrolled in behavioral and mHealth studies, and the participants offered suggestions on how to improve upon the current study protocol. Several of the participants (4) expressed how excited they were to participate in this study when they were first approached. However, the majority of the patients who participated in these focus groups opted to withdraw or simply stopped using the RELAXaHEAD app on a consistent basis during the first three months of the trial.
Of all the feedback received, participants were most vocal about simplifying study requirements and providing more education on PMR. Evidence also indicates that a simplified and tailored medication regime correlates with better adherence (33). Since there were a number of daily steps involved in this study, including entering information and completing PMR, it was difficult for patients to keep track of what they had and had not done, which is why a more streamlined approach is necessary. Additionally, during enrollment, the study team should walk through the app with the patients and explain the theory behind PMR and why it is important to complete both sessions on a daily basis. Some patients requested statistics on the impact of PMR among participants of past studies; therefore, results from a previous study providing behavioral therapy via a mobile app, which showed that patients receiving PMR exhibited a decreased number of headache days compared to the control group (34), would be important information to motivate further participants.
Strengths of the study were that all participants met ICHD-3 criteria. A prior meta-synthesis of 10 articles on migraine patients’ preferences for treatment revealed that only two of 10 articles used the International Classification of Headache Disorders (ICHD) criteria (17). Moreover, this study includes more detailed demographic and headache data than prior qualitative studies. In the meta-synthesis, only one study reported race, few studies appeared to capture data based on the headache treatment clinical practice guidelines, and only three studies specified the number of migraine/headache days of those participating in the study. In fact, one study had participants with only one headache day a month (35) and another had participants with only 1–2 headache days/month (36). Only one had participants with four or more days a month, which is typically the average number of headache days a month in which patients are on preventive medications (37).
Limitations of the study were that the focus groups took place at one large academic urban medical center and thus the participants may not be representative of the national population. Despite the study being in a very diverse city, few participants in the focus groups were under-represented (50% were white, 33.3% were Asian); only 16.7% were black and from other races. Due to modest sample size, results are not fully generalizable, and we cannot evaluate differences by race and ethnicity. In addition, the modalities discussed (mHealth tools) and behavioral techniques were limited to just one smartphone application (RELAXaHEAD) and to one behavioral modality (PMR). Another potential limitation was that the focus groups were led by a headache neurologist who was also the principal investigator of the study. The investment of the facilitator in the research, the unequal power relationship between the facilitator and participants and social desirability effects may bias the results. Finally, while we believe focus groups were good mechanisms to spark conversation and allowed participants to feed off of others’ answers to provide feedback, the methodology of focus groups may limit findings that a one-on-one interview uncovers and can lead to the loss of certain voices within the group (38).
Future work should continue to involve people with migraine, through participatory action research, community-based participatory research, and the whole spectrum of community engagement. Future work should also try to include participants who are representative of those who experience migraine, including diverse racial/ethnic backgrounds sometimes under-represented in research. In addition, inclusion of participants with the common comorbidities of migraine, such as depression and anxiety, might improve generalizability of findings and broaden the targets of digital health solutions in persons with migraine; these approaches are also important because depression might affect reward learning and anxiety may affect working memory (39). Early findings with the RELAXaHEAD app suggest that depression is associated with reduced adherence to both PMR and the diary, while anxiety was positively associated with adherence to both (34).
Conclusion
People with migraine are motivated to participate in mHealth and behavioral treatment studies to try new treatment modalities and/or further the knowledge in the field of migraine medicine. In general, they are receptive to non-pharmacologic treatments. They have different preferences for lengths of daily behavioral treatments, and they have differing opinions on how to best track their symptoms. They also want individualized ways to be contacted by study teams to meet their specific circumstances. There is a need for continued patient engagement/patient centered research as we continue to develop new treatments in the field of headache medicine, so that we can learn the best ways patients can integrate various study interventions into their daily routines to optimize adherence and best test efficacy.
Clinical implications
People with migraine are motivated to participate in mHealth and behavioral treatment studies. People with migraine want greater flexibility and choice in study interventions and modes of follow-up. There is a need for continued patient engagement/patient centered research as we continue to develop new treatments in the field of headache medicine. There is a need to learn the best ways in which patients can integrate various study interventions into their daily routines to optimize adherence and best test efficacy.
Supplemental Material
CEP888230 Supplemental material - Supplemental material for Focus group findings on the migraine patient experience during research studies and ideas for future investigations
Supplemental material, CEP888230 Supplemental material for Focus group findings on the migraine patient experience during research studies and ideas for future investigations by Mia T Minen, Kaitlyn Morio, Kathryn Berlin Schaubhut, Scott W Powers, Richard B Lipton and Elizabeth Seng in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by a NIH K23 from NCCIH [K23AT009706] and from a pilot grant from the NYU Center for Healthcare Innovation and Delivery Science.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.