
Abstract
Background
Paragangliomas are rare neuroendocrine tumors, especially in the bladder. Although many paragangliomas are non-functional, functioning paragangliomas present with many non-specific signs and symptoms, such as hypertension and headache, complicating their diagnosis. Here, we report a case of micturition-induced severe headache associated with a bladder paraganglioma.
Conclusion
This case elucidates the association between micturition-triggered headaches and bladder paragangliomas. The presence of a post-micturition severe headache should suggest the possibility of a bladder paraganglioma.
Introduction
Functioning paragangliomas, the extra-adrenal counterparts of pheochromocytomas, are rare catecholamine-producing tumors that arise from the ganglia along the sympathetic and parasympathetic chains (1). A significant characteristic of these tumors is excessive catecholamine secretion on becoming functional (2). This excess catecholamine secretion is the main cause of numerous non-specific clinical manifestations, such as hypertension, palpitations, headache, and sweating (3). The anatomical location of the tumor also contributes to its distinct symptoms (2), such as painless hematuria (4) and low back pain (5). Since these are rare tumors, many clinicians may never encounter them. Thus, when a patient presents with a headache induced by micturition, even neurologists with expertise in headaches may not consider a bladder paraganglioma as an etiological factor if they have never encountered similar cases before. This lack of familiarity can prolong diagnosis and interfere with optimized patient management. Fortunately, advances in imaging techniques and biochemical testing have made it easier to arrive at the appropriate diagnosis as long as a tumor is suspected. Therefore, physicians need to remain aware of these tumors and confirm their presence when confronted with corresponding symptoms (2).
Case description
In March 2021, a 57-year-old woman visited our outpatient headache clinic complaining of a 1-day history of intermittent fixed headache. At presentation, she reported that these headaches had occurred four times. Each time, the headache started from the left side of the nose and then gradually extended to the whole forehead and the parietal and occipital regions, where it persisted for 5–10 minutes each time. The patient scored her pain as 7 (out of 10) on a standard visual analog scale (VAS), without any associated symptoms. She denied any medical history except mild head trauma without loss-of-consciousness at age 12. Her cranial MRI showed unremarkable outcomes, thus, the physician at our clinic first considered the possibility of Sluder’s syndrome, and the patient was administered oral gabapentin. However, after three days of treatment, her pain did not improve. She returned to our clinic and was admitted to the neurology ward. On admission, her headaches worsened, occurred approximately 2–4 times daily, and her VAS score reached 10. Considering her pain only lasted 5–10 minutes, we did not provide any acute treatment for immediate pain relief, and the patient was administered oral pregabalin (75 mg, twice per day) for pain prophylaxis. Unfortunately, the patient did not respond to pregabalin, and her pain did not improve. A lumbar puncture was performed, revealing cerebrospinal fluid pressure to be within-normal-limits (80 mmH2O). Meanwhile, her laboratory results showed elevated cerebrospinal fluid protein levels (765.87 mg/L), leading us to consider the possibility of intracranial inflammation. Methylprednisolone sodium succinate was administered via an intravenous fluid drip. Despite receiving a 1-week steroid hormone treatment, she continued to experience severe headaches without improvement. The patient complained that her pain occurred after she got out of bed. Therefore, considering her cerebrospinal fluid pressure (80 mmH2O, the lower threshold of the reference range), we considered the possibility of an intracranial hypotension headache and started a fluid infusion instead of a steroid hormone drip. Afterward, her pain did not improve after 3 days’ treatment, the headaches emerged more frequently than before. When we were confused about the diagnosis, a family member noted that the pain occurred each time after micturition. This critical clue indicated that the pain originated from the urinary tract. A subsequent ultrasound examination of the urinary tract revealed a bladder wall mass. Based on our observations of hypertensive attacks (190/110 mmHg) only during headaches, the absence of any history of hypertension, and the unremarkable results of a general physical examination, we considered the possibility that a functioning bladder paraganglioma was releasing excessive catecholamine and causing blood pressure elevation. However, to our surprise, there was no significant elevation of catecholamine levels in the blood and 24 hour-urine laboratory examination; nevertheless, because the blood sample was not collected during a headache, this may have been a false-negative result. The signs and symptoms, combined with the urinary tract ultrasound examination results, still suggested a bladder paraganglioma. The patient was then transferred to the urology ward and underwent surgery. A mass was visualized within the bladder wall during cystoscopy (Figure 1). During the operation, her blood pressure was significantly elevated when the mass was touched. The mass was completely removed during surgery. The resected mass measured 2.4 cm × 2.2 cm × 1.8 cm, and a pathological examination confirmed our diagnosis (Figure 2). After removal of the bladder paraganglioma, micturition no longer triggered headaches. The patient reported no micturition-related headaches during her follow-up examinations. However, since paragangliomas are associated with the risk of recurrence, the patient has been advised to undergo long-term follow-up.

An obvious mass was directly located on the bladder wall under cystoscopic examination.
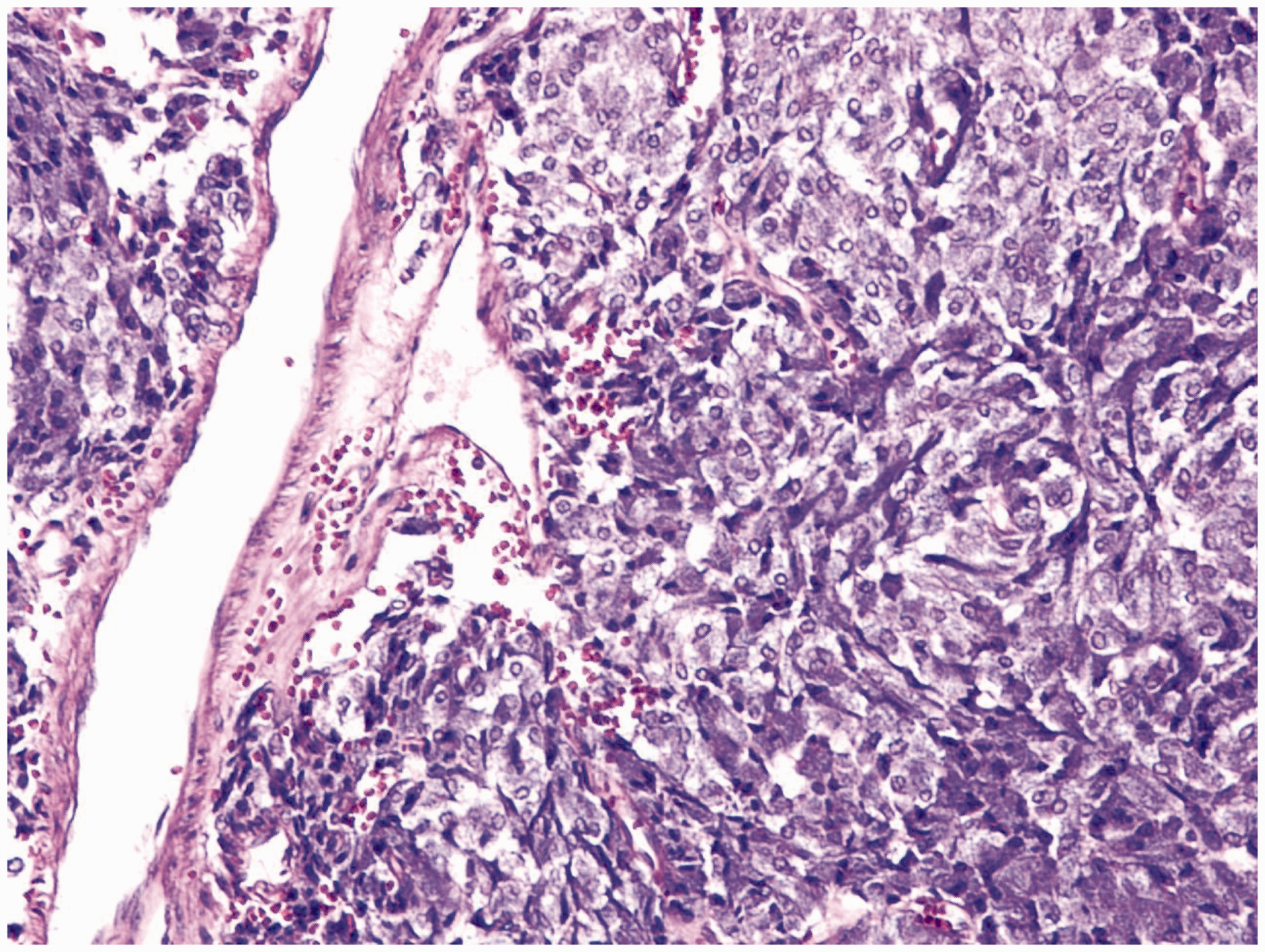
Histopathologic study of the mass showed tumor cells growing in a nested, zellballen pattern, consistent with the typical histopathological findings for paragangliomas. (x200)
Discussion
To our knowledge, micturition is a rare trigger for severe headaches. The findings associated with this case provide some insight into bladder paragangliomas. Micturition-triggered headaches associated with bladder paraganglioma have been reported in limited literature. In these reports, the headaches were accompanied by symptoms such as painless hematuria (4), abdominal pain (6), and micturition syncope (7). Headache is also a common symptom of tumors located outside the bladder; however, in these cases, it is not triggered by micturition and is often the result of a hypertensive crisis (8). Thus, clinicians should remain cautious about this tumor when headache and hypertension occur simultaneously. We assumed that the severe headache for our patient was due to hypersecretion of catecholamines upon stimulation of the paraganglioma by micturition, caused rapid elevation of her blood pressure, resulting in a severe headache. Surgical removal of the tumor was a priority for our patient and resulted in a full recovery. Additionally, our clinic physician first considered the possibility of Sluder’s syndrome because the pain began along the left side of her nose, which is a unique feature of this syndrome (i.e., the pain normally begins at the nose and then extends to other regions including the forehead and occiput). However, no literature has linked Sluder’s syndrome and paragangliomas. Thus, we are unsure whether they have an association, and future studies should confirm or disprove this potential relationship.
The first case of bladder paraganglioma was described by Zimmerman et al. in 1953 (9). These tumors are highly prevalent in young adult females, with the common symptoms and signs being hypertension and hematuria (10). The pathogenic factors underlying bladder paragangliomas remain unclear and may be related to certain gene mutations (11). Although some patients show a full recovery after complete tumor resection, some experience recurrence, metastases, or even death from the tumor. For recurrent or metastatic tumors, chemotherapy, target therapy, or radiation therapy is suggested based on the personal situation after surgical resection of all visible tumors. Even though these tumors rarely recur or metastasize, long-term follow-up is advisable.
Two major lessons can be taken away from this case. First, both clinicians and the patient failed to recognize that the headache was rapidly induced by micturition. This delayed diagnosis and resulted in improper management. Clinicians should always ask probing questions to help patients recognize headache triggers as soon as possible when faced with an unusual headache, since trigger recognition is critical to the final diagnosis for unusual headaches. Second, due to our limited knowledge about paragangliomas, we did not recognize that the collection of intravenous blood for catecholamine testing was best performed during the actual pain attacks. The outcomes of biochemical testing are less convincing otherwise. Since catecholamines are usually released intermittently and not continuously, the collection of blood samples for biochemical testing is better performed when hypertension or the symptoms occur to avoid false-negative results. Moreover, a previous report stated that increased plasma metanephrine levels had an average sensitivity of 97% and specificity of 93% across 15 studies (12). This idiosyncrasy appears to play an essential role in the diagnosis of paragangliomas (2).
Here, we demonstrate that micturition can trigger severe headaches in patients with bladder paragangliomas. In these cases, tumor resection can provide relief. For these patients, a low-risk surgical approach should be prioritized. Due to the limited literature on micturition-induced severe headaches associated with bladder paragangliomas, we believe that our study will be helpful to clinicians when they encounter similar situations.
Clinical Implications
Severe headache triggered by micturition has been tightly associated with bladder paragangliomas. Removal of a bladder paraganglioma can completely eliminate the headache-related symptoms.
Footnotes
Acknowledgments
We would like to thank Shuxiao Zhao (Department of Urology, the First Affiliated Hospital of Guangxi University of Chinese Medicine) for providing the cystoscopy image and Hua Tang for providing the pathology image (Department of Pathology, the First Affiliated Hospital of Guangxi University of Chinese Medicine).
Consent
Written consent was obtained from the patient for publication of this case report and any accompanying images.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.