
Abstract
Background
Although the European Medicines Agency and the US Food and Drug Administration have cleared several devices that use neuromodulation to provide clinical benefits in the acute or preventive treatment of migraine, the Clinical Trials Committee of the International Headache Society has not developed guidelines specifically for clinical trials of neuromodulation devices. In recognition of the distinct needs and challenges associated with their assessment in controlled trials, the Committee provides these recommendations for optimizing the design and conduct of controlled trials of neuromodulation devices for the acute and/or preventive treatment of migraine.
Methods
An international group of headache scientists and clinicians with expertise in neuromodulation evaluated clinical trials involving neuromodulation devices that have been published since 2000. The Clinical Trials Committee incorporated findings from this expert analysis into a new guideline for clinical trials of neuromodulation devices for the treatment of migraine.
Results
Key terms were defined and recommendations provided relative to the assessment of neuromodulation devices for acute treatment in adults, preventive treatment in adults, and acute and preventive treatment in children and adolescents. Ethical and administrative responsibilities were outlined, and a bibliography of previous research involving neuromodulation devices was created.
Conclusions
Adoption of these recommendations will improve the quality of evidence regarding this important area in migraine treatment.
Introduction
The Clinical Trials Committee of the International Headache Society has a long-standing history developing guidelines for clinical trials of primary headache disorders, including migraine. Current publications that provide guidance for clinical trials on drugs in adults with migraine include those for the acute treatment of migraine and the preventive treatment of chronic and episodic migraine (1–3). Guidelines are also available for children and adolescents for the preventive treatment of migraine (4).
Recent years have witnessed an increasing interest in and testing of neuromodulation devices for the therapeutic approach of primary headaches, particularly migraine and cluster headache. The European Medicines Agency and US Food and Drug Administration have recently cleared several devices based on the principles of neuromodulation for the acute or preventive treatment of migraine. Both agencies have established processes for the evaluation and clearance of medical devices (5,6), and the evidence-based expansion of the neuromodulatory class of treatments is a promising development for clinicians and their patients with migraine. However, because the supporting data required for clearance depends on the classification of the device being considered for clearance (7,8), clinical trials evaluating them use different designs, trial populations, and efficacy outcomes (9), which complicates the interpretation of results and limits their translational utility.
The device-specific methodological challenges and inconsistency of evidence supporting the efficacy and safety of neuromodulation devices in migraine has heightened the need for guidance. Based on findings from a subject matter expert review of clinical trials published in the past 20 years (Table e-1 and Table e-2 in the Supplementary Material), as well as recommendations from existing guidelines for clinical trials for acute and preventive treatments of migraine (1–4), this guideline proposes standardized approaches to the assessment of neuromodulation devices intended for the acute and preventive treatment of migraine for adults and children/adolescents. To facilitate consultation, its recommendations are presented mostly in tabular format.
1. Definitions
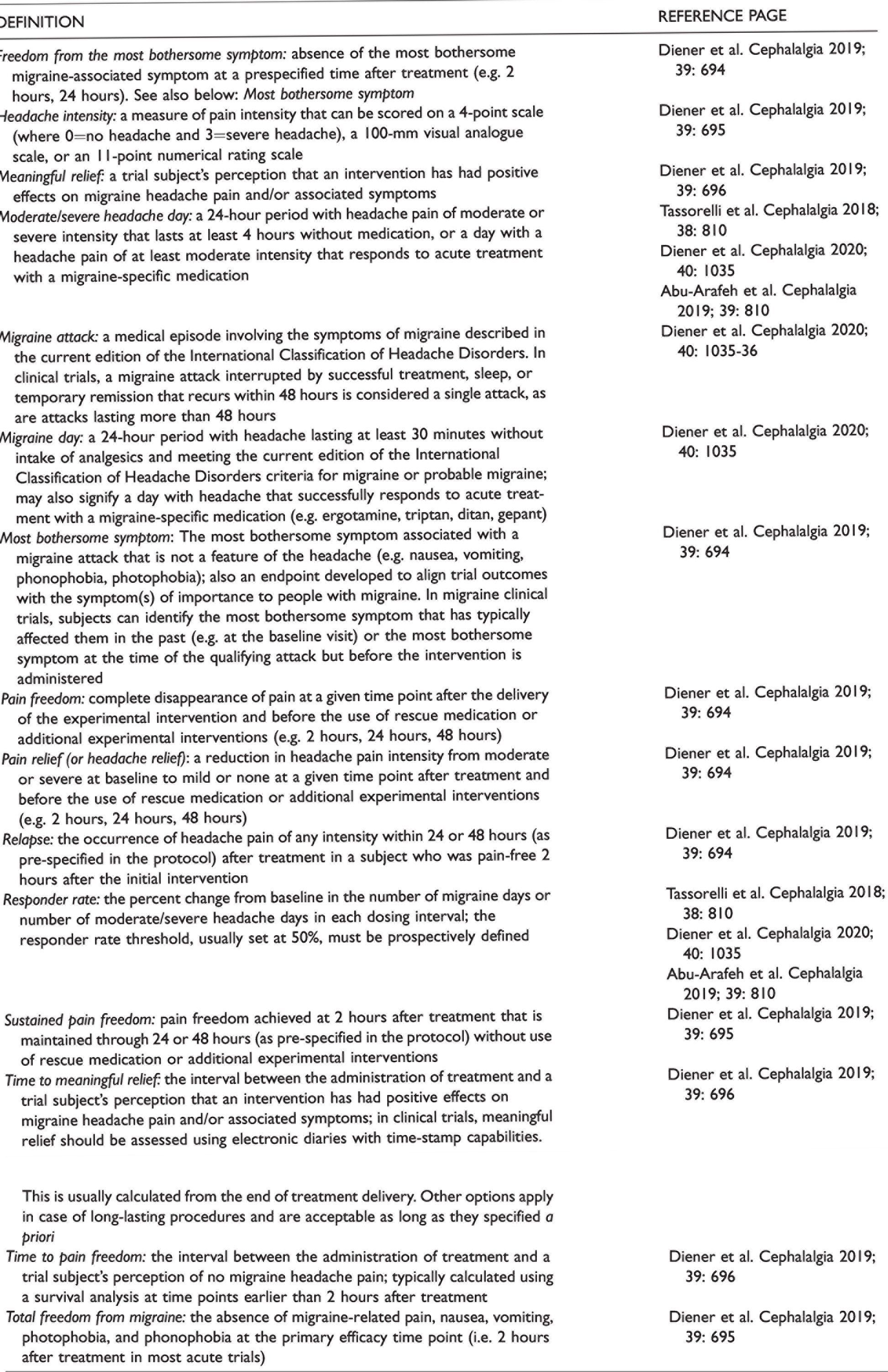
Please also see Table 1 for the full list of definitions of terms used in this manuscript.
Definition of terms used in the manuscript.
1.1 Medical device
The European Union (5) defines a “medical device” as any instrument, apparatus, appliance, software, implant, reagent, material, or other article intended by the manufacturer to be used, alone or in combination, for human beings for one or more of the following specific medical purposes:
Diagnosis, prevention, monitoring, prediction, prognosis, treatment, or alleviation of disease Diagnosis, monitoring, treatment, alleviation of, or compensation for, an injury or disability Investigation, replacement, or modification of the anatomy or of a physiological or pathological process or state
The authorised purposes of a medical device also include providing information by means of in vitro examination of specimens derived from the human body that does not achieve its principal intended action by pharmacological, immunological, or metabolic means, in or on the human body, but which may be assisted in its function by such means (5).
1.2 Neuromodulation device
A neuromodulation device is defined as any medical device that modulates the activity of the brain, the spinal cord, or peripheral nerves by means of electricity, magnetic fields, or other device-mediated modalities to either inhibit or facilitate neural impulses to achieve a clinical benefit for patients. This definition excludes devices for delivering medications, as their principal mode of action is associated with the drug, not the device. Trials using devices for drug delivery should follow the guidelines for clinical trials of pharmaceuticals (1–4).
2. General recommendations
General recommendations for clinical trials of neuromodulation devices for the treatment of migraine.

ICHD, International Classification of Headache Disorders.
aRecommendations coincide with current recommendations for clinical trials of pharmaceuticals; for more information, refer to Diener et al., 2019; Tassorelli et al., 2018; Diener et al., 2020; Abu-Arafeh et al., 2019 (1–4).
Concurrent and non-concurrent controls for clinical trials of neuromodulation devices for the treatment of migraine. Adapted from reference 13.

2.1 Trials for the acute treatment of migraine in adults
Recommendations for trials of neuromodulation devices in the acute treatment of migraine in adults are shown in Table 4. Most of these recommendations align with the guidelines for controlled trials of acute treatment of migraine attacks in adults (1). Refer to that publication (1) for more information regarding specific items in Table 4.
Recommendations for clinical trials of neuromodulation devices for the acute treatment of migraine in adults.

aRecommendations coincide with current recommendations for clinical trials of pharmaceuticals; for more information, refer to Diener et al. 2019 (1).
For the measurement and reporting of adverse events please refer to Table 2.
2.2 Trials for the preventive treatment of migraine in adults
Recommendations for trials of neuromodulation devices in the preventive treatment of migraine in adults are presented in Table 5. Unlike clinical trials of medications for the preventive treatment of migraine, which use different designs to evaluate subjects with episodic migraine and chronic migraine (2,3), clinical trials of neuromodulation devices can combine these populations (Table 2). This consideration is based on the fact that episodic and chronic migraine differ in terms of comorbidity, need for concomitant medications and use of acute medications, but the potential of neuromodulation devices to interfere with concomitant treatments or associated comorbidities is very limited. Refer to those guidelines (2,3) for more information regarding the categories discussed below.
Recommendations for clinical trials of neuromodulation devices for the preventive treatment of migraine in adults.

aRecommendations coincide with current recommendations for clinical trials of pharmaceuticals; for more information, refer to Tassorelli et al., 2018 and Diener et al., 2020 (2, 3).
bIf not used as the primary endpoint.
For the measurement and reporting of adverse events please refer to Table 2.
2.3 Trials for the preventive treatment of migraine in children and adolescents
Recommendations for clinical trials of neuromodulation devices in the treatment of migraine in children and adolescents are shown in Table 6. As with the recommendations for adult populations, these recommendations largely align with current guidance for clinical trials of pharmaceuticals in children and adolescents with migraine (4). Refer to that guideline for more information regarding the recommendations in Table 6.
Considerations for clinical trials of neuromodulation devices in children and adolescents.

aRecommendations coincide with current recommendations for clinical trials of pharmaceuticals; for more information, refer to Abu-Arafeh et al., 2019 (4).For the measurement and reporting of adverse events please refer to Table 2.
3. Steering committee
Neuromodulation devices for the treatment of patients with migraine tend to be developed by researchers who may not have expertise in the field. For trials sponsored by industry, a Steering Committee that includes academics with an expertise in Headache Medicine, biostatisticians, and (if appropriate) company representatives should be formed. For investigator-initiated trials (i.e. developed and sponsored by independent investigators or academics), a Steering Committee is unnecessary. Whether or not a committee is formed, investigators and sponsors are responsible for all aspects of a clinical trial, including conception; design; operational execution; data handling; data analysis and interpretation; subsequent reporting and publication; and compliance with all local laws and regulations.
4. Independent data safety monitoring board
An independent data safety monitoring board and predefined stopping rules for futility or safety are recommended in case of prior knowledge or strong suspicion that a device under consideration has the potential to harm patients (e.g. when serious side effects were reported in proof-of-concept studies). Independent interim analysis by the data safety monitoring board should be considered for assessment of the pre-defined stopping rules.
5. Trial registration
Prior to the initiation of a trial, registration is necessary at clinicaltrials.gov, clinicaltrialsregister.eu, anzctr.org.au, or a similar regional or national official database.
6. Publication
A publication committee should be formed prior to the start of the trial. Before a trial is initiated, investigators and sponsors (if applicable) should agree upon timelines for publication; ideally, estimated publication dates be included in the protocol. All research results — primary and secondary endpoints and all safety data, either positive or negative — must be published in manuscript form; at the time of trial initiation or at the end of recruitment, a design paper with baseline data may be published. Authorship should be based on the recommendations of the International Committee of Medical Journal Editors (21).
7. Ethics
All clinical trials must follow standardized ethical and safety guidelines, and they must be approved through appropriate Institutional Review Boards or Ethics Committees. In trials involving children and adolescents, participants must provide informed assent, and parents or guardians must provide informed consent. Trials must be conducted in accordance with the Declaration of Helsinki (22) and Guideline for Good Clinical Practice (15), and they must follow the rules of local regulatory authorities (5,6).
8. Conflicts of interest
To maintain the credibility of a trial, authors must declare their conflicts of interest in trial-related publications. A conflict of interest exists whenever professional judgment concerning a primary interest (e.g. subject wellbeing or the validity of research) may be influenced by a secondary interest (e.g. financial relationship to a trial sponsor). Financial relationships that represent potential conflicts of interest include employment, consultancies, research grants, fees and honoraria, patents, royalties, stock or share ownership, and paid expert testimony. Note that conflicts of interest extend to an investigator’s immediate family (i.e. partner and children). Investigators should avoid entering into agreements with sponsors, both for-profit and non-profit, that restrict access to study data, limit its analysis and interpretation, or interfere with the independent preparation and publication of manuscripts.
9. Post-approval registries
The IHS recommends post-approval product registries (i.e. prospective open-label observational studies) to evaluate the use of newly-cleared devices in clinical practice. Registries generate real-world data on long-term efficacy, tolerability, and safety. They also measure compliance and adherence. Registries may also yield insights about individuals with migraine who have coexistent or comorbid conditions (e.g. chronic pain syndromes, cardiovascular disease) that disqualified them from clinical trials.
10. Health technology assessment
Health technology assessments seek to provide policy makers with information on the clinical and economic value of health technologies (including medical devices) and organizational systems used in health care to inform their reimbursement or coverage decisions (23,24). The assessment of medical devices poses different challenges from those of pharmaceuticals. Compared with medications, randomized controlled trials of devices are often more difficult, and outcomes depend heavily on the training and experience of investigators, clinical trial personnel, and subjects; these challenges can be exacerbated by product modifications, which are rare with medications but relatively frequent with devices (24). Health technology assessments can be performed by transnational agencies, but they are often delegated to national or local agencies that use different process and protocols (25,26). The IHS recently published an official position statement intended to facilitate and standardize the conduct of health technology assessments of medications and neuromodulation devices approved and/or cleared for the acute and preventive treatment of migraine (27).
11. Methods used for the development of these guidelines
These guidelines represent an activity of the Clinical Trials Committee of the IHS. The initial work was performed by an international working group of experts on migraine and neuromodulation devices that was assisted by a small group of junior headache researchers. The process used to develop the guideline involved:
Reaching consensus on a definition of neuromodulation device Evaluating the designs and endpoints of clinical trials conducted to test the efficacy of neuromodulation devices in the acute or preventive treatment of migraine in the past 20 years (Table e-1 and Table e-2 in the Supplementary Material) Preparing and revising multiple versions of the recommendations until all members of the working group could support them Soliciting and incorporating feedback on the expert analysis from:
○Stakeholders that included pharmaceutical and neuromodulation device manufacturers and patient associations ○IHS members, who had access via the IHS website Obtaining the final approval of the IHS Board of Trustees
Clinical Implications
Neuromodulation devices are emergent in the migraine armamentarium, with several devices recently approved in the Europe and the United States for acute and/or preventive treatment The absence of a trial guideline that recognized the distinct approach to treatment of migraine used by neuromodulation devices limited understanding of their therapeutic potential These recommendations for the assessment of neuromodulation devices in the acute and preventive treatment of migraine will facilitate research and help to clarify their optimal role in clinical practice
Supplemental Material
sj-pdf-1-cep-10.1177_03331024211010413 - Supplemental material for Guidelines of the International Headache Society for clinical trials with neuromodulation devices for the treatment of migraine
Supplemental material, sj-pdf-1-cep-10.1177_03331024211010413 for Guidelines of the International Headache Society for clinical trials with neuromodulation devices for the treatment of migraine by Cristina Tassorelli, Hans-Christoph Diener, Stephen D Silberstein, David W Dodick, Peter J Goadsby, Rigmor H Jensen, Delphine Magis, Patricia Pozo-Rosich, Hsiangkuo Yuan, Daniele Martinelli, Thomas van den Hoek, Marie Deen, Messoud Ashina and Gisela M Terwindt in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.