
Abstract
Background
To evaluate the prevalence, predictive factors and clinical characteristics of cough headache in our respiratory clinic and to investigate the coexistence between cough headache, migraine and tension-type headache.
Method
We consecutively investigated patients referred to our respiratory clinic with complaints of cough and selected patients with cough headaches to complete a structured interview and examination.
Results
Six hundred and seventy-nine patients with cough were studied and 122 patients were diagnosed with cough headache. The prevalence of cough headache was 18.0% in these coughing patients. According to multivariate analysis, being of an age between 31–50 years was a risk factor for cough headache (OR 2.0). Cough headache was associated with cough severity: Compared with the mild group, the moderate group (OR 2.3) and the severe group (OR 3.3) were more vulnerable to cough headache. Headache severity had a positive correlation with cough severity (ρ = 0.301, p = 0.028), age (ρ = 0.199, p = 0.029), and headache duration (ρ = 0.242, p = 0.008). In cough headache patients, 30.3% had tension-type headache and 10.7% had migraine in the preceding year.
Conclusions
Cough headache is not rare in respiratory clinics and the characteristics are somewhat different from those in headache clinics. An age of between 31–50 years and cough severity were risk factors for cough headache. Headache severity was related to cough severity, age and headache duration.
Background
Cough headache (CH) is generally considered a rare condition (1–3). It is defined as a headache only precipitated by coughing or other Valsalva maneuvers (1,4). Rasmussen and Olesen estimated that the lifetime prevalence of CH in the general population is 1% (5). The prevalence of CH in neurological departments ranges from 0.4% to 1.2% (6–8). However, one study from Turkey reported that 19.3% of patients with cough had CH in a chest clinic (9). The epidemiology data are still very limited and, so far, cough headache has not been studied in mainland China.
Cough headache can be further divided into primary and symptomatic cough headache. Primary cough headache (PCH) is characterized as sudden onset and usually affects males > 40 years old, is often bilateral with a posterior location, and lasts from seconds to 2 h. About 2/3 patients with PCH report associated symptoms, such as nausea and vertigo (1,3). However, the distinction between primary and symptomatic cough headache is debatable, due to the unknown mechanism of CH (1,10), and there have been few studies on cough headache since ICHD-3-beta was released.
Migraine and tension-type headache (TTH) are two of the most common primary headache disorders worldwide (11). Migraine and TTH can be aggravated by cough (1,12). In rare cases, it has been reported that cough or other Valsalva maneuvers can be a potential trigger of migraine and TTH (12,13). Nevertheless, the relationship between cough headache and migraine or TTH is unclear and little attention has been paid to the comorbidity of the three types of headache.
The aim of this study was to evaluate the prevalence, predictive factors, and clinical characteristics of cough headache in our respiratory clinic and to investigate the coexistence between cough headache, migraine and TTH.
Methods
Procedure
We studied consecutive patients with complaints of cough who visited the respiratory clinic of Chinese PLA General Hospital from 1 January 2016 to 31 December 2016. A respiratory specialist determined the cough etiology of all patients according to the history, physical examination, laboratory test and chest imaging and then completed the structured interview. We employed the cough severity score (CSS) to evaluate the intensity and frequency of cough (14). It is a two-part scale referring to cough symptoms during the day and night (15). The Chinese edition of this scale was recommended in the national cough guideline by the Chinese Society of Respiratory Diseases and has been used in some studies (16,17). The CSS is shown in Table 1. Total score (both day and night) was calculated and grades 0–3 were accepted as mild, grades 4–7 were defined as moderate and grades 8–10 were accepted as a severe cough.
Cough severity score.

The same neurologist obtained demographics and completed the headache profiles if the patient had a cough headache. The diagnosis of CH must fit the criterion of occurring only in association with coughing. Headaches that could be better accounted for by another ICHD-3 beta diagnosis were excluded. Demographic questions covered age, gender, ethnicity (Han versus non-Han), and marital status (unmarried versus married/divorced), habitation (urban versus rural), educational level (under or above high school). Tobacco use, alcohol use and body mass index (BMI) were also documented. Headache profiles included age at headache onset, relationship between cough and headache, cough duration, headache location, quality, intensity, other triggers, and headache duration and accompanying symptoms. Among Valsalva-like headache triggers, we used the word “transient exertion” to define sudden and short-lasting, spontaneous or unintentional straining and effortful action in daily life. Numerical rating scale (NRS) was used to evaluate the intensity of headache (18). Grades 1–3 were considered as mild, grades 4–6 were regarded as moderate and grades 7–10 were severe. In addition, all patients underwent a detailed neurological examination by the neurologist.
Meanwhile, migraine and TTH were examined through a structured questionnaire that included the same items used in a Chinese national epidemiology study (19); these items were validated for headache assessment and diagnosis in the general population (20).
Ethics
The study protocol was approved by the Ethics Committee of the Chinese PLA General Hospital, Beijing (registration number: S2015-085-01). Participants had to sign informed consent before participating.
Statistics
Data were processed using Excel 2013 and analyzed using SPSS 22.0. Descriptive statistics were offered as the mean ± standard deviation (SD) or percentages. Median values were presented if the parameters were not normally distributed. Wilcoxon signed rank test was used to determine the difference of CSS according to different coughing etiologies. For categorical data, Chi-square tests were used to compare the difference between groups. Multivariate logistic regression identified an odds ratios (ORs) with 95% confidence intervals (CIs) for having cough headache, according to demographic and clinical characteristics of cough of the sample. Spearman correlation analysis was used to assess the relationship between two ranked variables. All calculated p-values were two-tailed and statistical significance was set at p < 0.05.
Results
Among 713 consecutive patients with cough, 34 patients refused to cooperate. The response rate was 95.2%. Overall, 679 respondents (241 males, 438 females) participated in this study. The median age of the patients was 42 years (range 14–86 years). The median duration of cough was 3 weeks (ranging from 0.2–1560 weeks).
The causes of cough were respiratory tract infection (52.6%), asthma (23.7%), chronic pharyngitis (13.2%), chronic bronchitis (5.0%) and other miscellaneous etiologies (7.2%). Kruskal Wallis test was conducted and showed that there was difference of CSS among these coughing etiologies(p = 0.007). Further, the major two disease (infection and asthma) which totally constituted 76.3% of all etiologies revealed no difference in CSS by Mann-Whitney test (p = 0.174).
Among 679 patients with cough, 17 patients (2.5%) had persistent headache along with their airway infection; they were excluded from the cough headache category. One hundred and twenty-two patients were diagnosed with cough headache. The prevalence of CH in coughing patients was 18.0% and increased gradually with age (≤30: 10.1%; 31–50: 18.8%; >50: 20.8%). Further, the prevalence of females (19.9%) had no difference to that of males (14.5%) (p = 0.083).
Univariate analysis of demographic data, cough characteristics, personal habits between the CH group and non-CH group were conducted. Results are shown in Table 2. The prevalence of cough headache was significantly different in age group (p = 0.04), but this is not so for other demographic data (sex, ethnicity, educational level, marital status, living area, all p > 0.05). We found that the patients with CH differed significantly from non-CH patients in cough severity score (p = 0.000). While personal habits (smoking and alcohol), BMI, cough course and cough etiology showed no difference (all p > 0.05).
The characteristics comparisons between cough headache and non-cough headache.

Multivariate logistic regression (Table 3) rejected sex, smoking, alcohol use, cough course, cough etiologies and BMI as risk factors for CH (p > 0.05). Age between 31–50 years compared with age < 30 years remained an independent risk factor for CH, as did cough severity score: Compared with the mild group, the risk for CH increased in the moderate group and severe group.
Multivariable adjusted odds ratios (95% confidence interval) for CH.
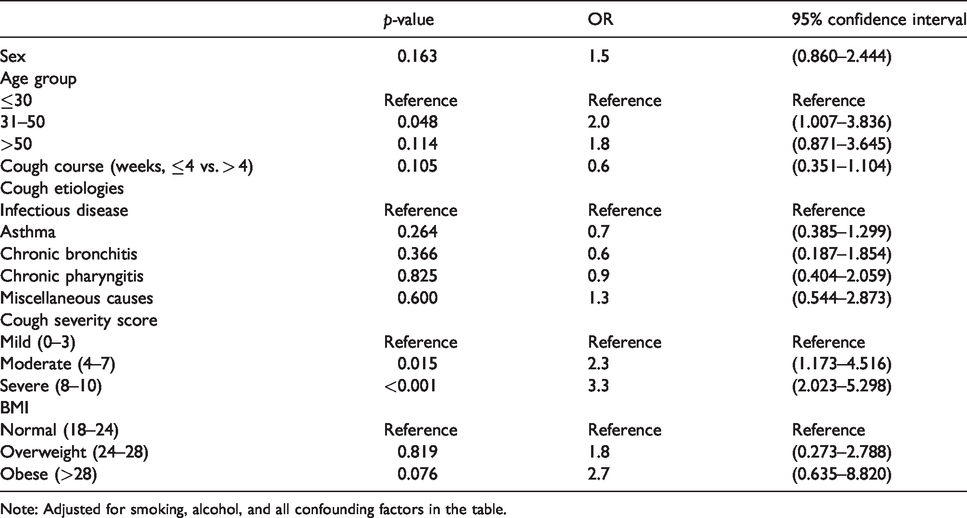
Note: Adjusted for smoking, alcohol, and all confounding factors in the table.
In total, 122 cases of cough headache were included in our study. According to the CH diagnostic criteria of ICHD-3, 122 patients fulfilled criterion A and criterion B. Two patients did not present as “sudden onset”, so 120 patients (98.4%) fulfilled criterion C. Three patients had a headache duration longer than 2 h, so 119 patients (97.5%) fulfilled criterion D. One hundred and twenty-two patients did not have any neurological deficits, positive signs, or headache features leading to other headache categories. Thus, 122 patients were consistent with criterion E. In all, 117 patients (95.9%) were regarded as fulfilling all ICHD-3 criteria for CH.
Among the 122 CH patients, 35 were males (28.7%) and 87 were females (71.3%). The median age of these patients was 41 years (range 17–77 years). The causes of cough were infection (51.6%), asthma (23.8%), chronic pharyngitis (10.7%), chronic bronchitis (4.1%), and other miscellaneous etiologies (9.8%).
The detailed characteristics of the patients’ headaches are summarized in Table 4. Overall, 105 patients(86.1%)had bilateral headache localization. A duration of headache of over 2 h was seen in three patients (2.5%) (7 h, 12 h, and 12 h, respectively). One hundred and twenty patients (98.4%) said that their headache reached a peak in several seconds. The other two patients reported that their peaking times were dozens of seconds and several minutes (about 3–5 min). Cough was the only trigger in 72.5% of patients, the other 27.5% of patients had more than one headache trigger, including transient exertion as the most common trigger followed by bending down and sneezing. Notably, associated features, such as migrainous symptoms (vomiting, photophobia and phonophobia, etc.) and autonomic symptoms were uncommon. Dizziness was the most common associated symptom. All patients reported that their headache could be relieved spontaneously after termination of their cough. Eighteen patients (14.8%) found massage in the pain area could mitigate their headache. None of the patients had positive neurological signs. Only 11 patients (9.0%) volunteered to receive a brain MRI scan during our study and the results showed no abnormalities.
The clinical characteristics of patients with CH.

In order to assess the relationship between the severity of headache and headache-related factors in CH patients, Spearman correlation analysis was performed (Table 5). According to the results, NRS has a significantly positive correlation with CSS (ρ = 0.301, p = 0.028), age (ρ = 0.199, p = 0.029) and headache duration (ρ = 0.242, p = 0.008). While cough course (ρ = 0.155, p = 0.091) and peak time of pain did not revealed correlation with NRS.
Correlation between NRS and other related factors.

In our survey, 50 patients (41.0%) had primary headaches in the preceding year in addition to CH. Among them, 37 patients (30.3%) were diagnosed as having tension-type headache and 13 patients (10.7%) had migraine.
Discussion
To the best of our knowledge, this is the first hospital-based cross-sectional survey on CH in mainland China. We found that the prevalence of CH in our respiratory clinic is 18.0%. Our result is similar to only one previous study conducted in a chest clinic, which showed the prevalence of CH is 19.3% (9). The lifetime prevalence based on a general population is 1% in Denmark (5). As for CH in headache clinics, the prevalence was estimated to be 1.2% by Chen et al. (6) and 0.4% by Pascual (7). We suggested that cough headache may be encountered more commonly in a pulmonary clinic than in a headache subspecialty clinic. With the chief complaint of headache, these patients who visited headache clinics may manifest more serious symptoms and various signs (8,21), whereas in our study, 77.8% of CH patients had headache intensity in a mild or moderate form and 100% of patients had negative neurological signs, leading to their low urge to attend headache clinics.
We found a trend that CH prevalence was elevated along with age, and the median age of CH patients was 41 years. This may partially confirm that CH predominantly affects patients older than 40 years of age (1). Pascual even reported the mean age of CH onset as 60 years (8,21). Some studies found males were in the majority in CH patients (3,4,6,9). While in our study, females accounted for 71.3%. This may be attributed to the baseline characteristics of our study population (of the 679 respondents, 438 were females). Further, according to our analysis, the prevalence of CH showed no difference between males and females and sex was not a risk factor for CH.
Infection, one of the cough etiologies, was not a risk factor for CH in our study. However, the study from Turkey showed that when an upper respiratory tract infection was added, the frequency of headaches increased (9). Raskin reviewed a series of CH cases and noted that headaches often arose during lower respiratory tract infections accompanied by cough (22). These previous studies might not clearly distinguish CH from a headache assumed to be attributed to systemic infection, whereas our study showed 2.5% of cough patients had headaches that might be attributed to systemic infections. In our study, these patients manifested as having persistent headache along with their infection. Fevers or generalized muscular soreness were often noticed. Cough served more likely as an aggravator rather than a precipitator for their headaches and we precluded them from CH. The relationship between infection and CH needs further exploration.
Multivariate analysis also revealed that being of age 31–50 years was an independent risk factor for CH in comparison to being <30 years. The reason for this phenomenon is unclear and more studies are required. Interestingly, our studies showed the prevalence of CH increased with age, whereas the risk of CH did not increase with age >50 years compared with age < 30 years. Many literatures have proved that the average pain threshold is significantly increased in older individuals compared to younger individuals (23), which may explain age >50 years not being a risk factor for CH. The reason for our age subgroup setting (<30 years, 31–50 years, >50 years) was mainly because there was only one patient < 20 years old in the CH group, which may cause statistical error during analysis. Further, considering China’s retirement policy (24,25) and the average age of menopause for Chinese females, 50 years old could be the watershed of a Chinese person’s life. Age 50 years is also defined as the “red flag” for headache diagnosis (26).
Our study found cough severity was a predictor for CH. In particular when severe cough was compared to mild cough, headache risk increased by approximately three times. The result was consistent with the Turkey study (9). Although the underlying mechanism of CH remains unknown, some studies proposed that an increase in intra-thoracic and intra-abdominal pressure by cough could bring about a transient increase of intracranial pressure (ICP) with the existence of bilateral internal jugular vein valves incompetence, which could further precipitate the headache (27–29). Hence, we inferred that headache only occurs when cough is severe enough to trigger a significant increase of ICP by retrograde blood flow of the internal jugular vein.
CH usually subsided in a few seconds to several minutes and typically lasted less than 2 h (1) . However, in our study, three patients had a headache duration longer than 2 h (7 h, 12 h, and 12 h). This finding has also been reported by another study that indicated some patients with CH may experience a persistent dull headache lasting for hours (30). The presumed “postdrome of CH” may be noteworthy in future studies. In all, 98.4% of CH patients reached their headache peaks in several seconds. Therefore, from our experience, temporal relation and sudden onset were the core elements of CH diagnosis. The headache was mostly bilateral (86.1%) and often located in a temporal region (49.2%) in our series. The result was similar to the Turkey study (9), but other studies demonstrated that pain predominantly existed in the posterior area (6,8,21). In the Spanish case series, approximately 60% of CH was symptomatic (mainly posterior fossa-related abnormalities) and Rocío et al. proposed that pain in the occipital area might be a clue for the differential diagnosis of primary versus secondary CH (8,31). However, the Taiwan study found that occipital location showed no difference between the primary group and secondary group (6). Based on these findings, headache locations seemed to be variedly distributed and were not a distinctive hallmark in CH or symptomatic CH. The quality of headache was variable and was described as explosive, throbbing, pressing, and electric in most patients (2,3,8,9). Our study showed dull pain (55.7%) was the most common type, followed by throbbing pain (18.0%). Unlike the Taiwan study, which was based on a headache clinic that showed the intensity of headaches was mostly severe (67.6%) (6), our patients’ headaches were mainly mild (31.1%) and moderate (46.7%). This may indicate that only when headache was intense enough would the patients visit headache clinics. Associated symptoms were only present in 36.8% of the patients in our study. The top two symptoms were dizziness (19.7%) and nausea (9.8%). Similar to other studies (4,6,32,33), vomiting, photophobia, phonophobia, and autonomic symptoms were very uncommon. Apart from cough as a trigger, other triggers including sudden postural movements (56%), weightlifting (39%), laughing (33%), and defecating (22%) were reported by Pascual et al. (8). The Taiwan study found straining from stool was the most common trigger (41%) (6), while our study differed from previous studies in that the top three triggers were transient exertion (16.4%), bending down (15.6%) and sneezing (14.8%). By and large, our patients showed fewer Valsalva-like triggers and this may be another discrepancy between CH in a headache clinic and a respiratory clinic. The reason was unclear, but it may suggest that CH encountered in a respiratory clinic tends to be simpler and easily overlooked.
MRI or other brain imaging was considered to be essential for CH diagnosis in order to exclude potential etiologies, especially posterior fossa lesions like Chiari Malformation I. However, only 11 patients (9.0%) underwent brain MRI scan during our study. The possible reasons could be the expensive costs, relatively mild headache intensity, absence of neurological deficits and physical signs. Their unwillingness to do excessive examination in the context of respiratory clinics aroused our reflection on the necessity for and indications of an MRI scan. Some recent findings merit attention: Firstly, even if CM-I was detected, routine MRI was inadequate to assure the association between CH and CM-I (10,34,35). Secondly, 37–40% of cough headache found in CM-I patients improved at follow-up and most asymptomatic individuals with CM-I remained asymptomatic (93.3%) according to a systematic review (36). Thirdly, the underlying mechanism of CH was unclear and current research may imply that both PCH and symptomatic CH are related to paroxysmal increases in intracranial pressure (10). An ethnic factor should also be noted: In the Taiwan study, 89.2% of CH patients revealed no associated brain lesions, while Pascual reported that 58.8% of CH patients were diagnosed as having secondary CH in Spain (6,8). We thought that follow-up study may offer clues to distinguish the real “symptomatic CH”. Based on the illness and condition of patients, a “watch and wait” approach could be an alternative for brain imaging in pulmonary clinics.
Although CH can often spontaneously remit, 14.8% of our patients reported massage can relieve their headache. One recent study noted that an ocular compression maneuver can abort cough-induced headache (37). This procedure might be regarded as a potential treatment because CH often presents as short-lived pain and can be simply prevented by avoiding coughing in some cases. Especially in our study, an overwhelming majority of CH patients did not ask for drug therapies. Our study confirmed the conclusion in the Turkey study that the severity of the headache was correlated with the intensity of the cough (9). This result may reinforce the theory that CH was induced by transient elevation of intracranial pressure. We postulated that as the ICP elevated, the intensity of headache increased. Meanwhile, we found age and headache duration were also associated with headache intensity. The underlying mechanism was not so clear and more studies are required.
In all, 41.0% of CH patients had primary headaches in the preceding year. We found 30.3% of CH patients were also diagnosed with tension-type headache (TTH) and 10.7% of CH patients had migraine. The rate of TTH (30.3%) is higher than the prevalence in the general population in Mainland China (10.8%), and the rate of migraine (10.7%) is close to the prevalence of migraine in the general population (9.3%) according to data from a previous nationwide population-based study conducted using the same screening questionnaire (19). CH in our study is similar to TTH to some extent: CH is usually bilateral and has dull pain with mild and moderate intensity. Associated symptoms are limited and sometimes massage can relieve the pain. Furthermore, the action of a cough or Valsalva maneuver can cause neck and pericranial muscle contraction and tension (1,38). Research on the relation between CH and TTH as well as migraine is lacking, therefore comorbidity research on these primary headaches will be expected in the future.
This is the first survey on CH in mainland China as far as we know. The strengths of this study are its relatively large sample size and focus on CH from a respiratory clinic perspective. However, there are some limitations. First, not all patients received a brain MRI scan; thus, we cannot strictly distinguish whether CH is primary or symptomatic. Follow-up study may offer clues to distinguish whether CH is primary or symptomatic. Nevertheless, we did not do this work for various reasons. Second, the study was conducted in the year 2016, hence we were unable to use the newest ICHD-3 edition. Third, interpretation and generalization of our results should be performed with caution because the study was conducted in a single respiratory clinic.
Conclusion
Cough headache is not rare in respiratory clinics and is different from CH reported in headache clinics in some aspects. An age of 31–50 years and cough severity are risk factors for CH. The severity of headache has a positive relation with cough severity, age and headache duration. About 1/3 of our CH patients also had TTH.
Clinical implications
Cough headache is not rare in respiratory clinics. An age of 31–50 years and cough severity are independent risk factors for CH. The characteristics of CH in respiratory clinics are different from those in headache clinics.
Footnotes
List of abbreviations
CH: cough headache; TTH: tension-type headache; PCH: primary cough headache; CSS: cough severity score; BMI: body mass index; NRS: numerical rating scale; ORs: odds ratios; CIs: confidence intervals; ICHD-3 beta: International Classification of Headache Disorders, 3rd edition (beta version); ICP: intracranial pressure; CM-I: Chiari malformation type I.
Acknowledgements
We thank Dr Ping An, who discussed some details of this article with us.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of the Chinese PLA General Hospital, Beijing. Participants had to sign informed consent before participating.
Author contributions
YM was responsible for reviewing the literature, completing the survey, data analysis and writing the manuscript. XZ was responsible for the examination and diagnosis of our patients as a respiratory specialist. YW co-organized this survey. ZD served as headache specialist for consultation. SY was the principal investigator who was responsible for study design, data analysis and interpretation, and revision of the manuscript. As the corresponding author, SY had full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors read and approved the final manuscript.
Availability of data and materials
All data and materials in this article can be found in our neurology department.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grants 81671077, 81600952, 81771180, 81771200, 81901134 and 81901145), Beijing Natural Science Foundation Essential Research Project Z170002.