
Abstract
Objectives
To compare medication use and health resource utilization between migraineurs with evidence of opioid use at emergency department visit versus no opioid use at emergency department visit, and to examine predictors of opioid use among migraineurs at emergency department visits.
Methods
This was a retrospective study using REACHnet electronic health records (December 2013 to April 2017) from Baylor Scott & White Health Plan. The index date was defined as the first migraine-related emergency department visit after ≥6 months of enrollment. Adult patients with a migraine diagnosis and ≥6 months of continuous enrollment before and after their index dates were included. Descriptive statistics and bivariate analyses were used to compare medication use and health resource utilization between opioid users and non-opioid users. Multivariable logistic regression was used to examine predictors of opioid use at emergency department visits.
Results
A total of 788 migraineurs met eligibility criteria. Over one-third (n = 283, 35.9%) received ≥1 opioid medication during their index date emergency department visit. Morphine (n = 103, 13.1%) and hydromorphone (n = 85, 10.8%) were the most frequently used opioids. Opioid users had more hospitalizations and emergency department visits during their pre-index period (both p < 0.05). Significant (p < 0.05) predictors of opioid use at emergency department visits included past migraine-related opioid use (2–4 prescriptions, Odds Ratio = 1.66; 5–9 prescriptions, Odds Ratio = 2.12; ≥10 prescriptions, Odds Ratio = 4.43), past non-migraine-related opioid use (≥10 prescriptions, Odds Ratio = 1.93), past emergency department visits (1–3 visits, Odds Ratio = 1.84), age (45–64 years, Odds Ratio = 1.45), and sleep disorder (Odds Ratio = 1.43), controlling for covariates.
Conclusion
Opioids were commonly given to migraineurs at emergency departments. Previous opioid use, health resource utilization, age, and specific comorbidities might be used to identify migraineurs with a high risk of opioid use.
Keywords
Introduction
Migraine is a chronic neurological disorder characterized by recurring headache attacks on one side of the head (1). The prevalence of migraine in the overall US population is about 15%, which has remained stable over the past decades (2–8). Higher prevalence rates were observed among females, White (compared to Black and Asian), and middle-age populations (2–9). Common acute treatments of migraine include acetaminophen, antiemetics, triptans, nonsteroidal anti-inflammatory drugs (NSAIDs), and some ergots per guideline recommendations (10,11).
Migraine can be progressive in patients who are exposed to certain risk factors, among which medication overuse is an important contributor to the chronification of migraine, especially the overuse of opioids and barbiturates (12–14). In addition, guidelines note that preventive medications can help reduce migraine severity and control disease progression (15). According to the American Migraine Prevalence and Prevention (AMPP) study, about 38.8% of patients would benefit from taking preventive medications. However, only 12.4% of patients actually used migraine prophylaxis (16).
Migraine headache can lead to high resource use. According to a study based on the 2014 National Hospital Ambulatory Medical Care Survey (NHAMCS), “headache” was the fifth leading cause of emergency department (ED) visits in the US (8). In addition, the AMPP study reported that migraine accounted for 95% of all headache-related ED visits in a year (17).
Although several previous studies have reported a potential positive association between opioid use and migraine progression, this relationship has not been clearly quantified in a well-defined study cohort. In addition, there is limited research on opioid use among migraine patients specifically in emergency settings. It is important to understand the predictors for migraine patients who receive opioids at ED visits, which might assist in early treatment management. To address this gap in the literature, this study: a) described opioid and non-opioid medication use among migraine patients who presented to the ED; b) described and compared demographics, clinical characteristics, past health resource utilization (HRU), and past opioid use among opioid users and non-opioid users who presented to the ED with a diagnosis of migraine; and c) identified predictors for opioid receipt at ED visits as a function of demographics, clinical characteristics, previous HRU, previous opioid use, and previous preventive medication use.
Methods
Data source
This retrospective analysis used electronic health record (EHR) data from the Baylor Scott & White Health Plan (BSWHP) (18) between December 2013 and April 2017 obtained via The Research Action for Health Network (REACHnet) (19). This dataset contains multiple tables including encounters, prescriptions, diagnoses, and demographics for patients from Central Texas who received health services at BSWHP facilities. This study was approved by the Institutional Review Board from the University of Texas at Austin.
Sample selection
Patients were included if they met the following criteria: a) ≥18 years of age; b) had at least one migraine-related (International Classification of Diseases, Ninth Revision (ICD-9): 346.xx or ICD-10: G43.xxx) ED visit between June 2014 and October 2016; and c) had ≥6 months of continuous enrollment before and after the index date ED visit. The index date was defined as the first migraine-related ED visit date after at least six months of continuous enrollment. Note: patients may have had migraine-related ED visits during the pre-index 6 months, but the index ED visit date was chosen so that there was enough time to calculate baseline variable measures.
Selected patients were then categorized into an “opioid user” or “non-opioid user” group based on whether or not they received any opioids during their index date ED visit. Patients who received combination drugs that contained opioids were categorized as an opioid user.
Study variables
Demographic variables in this study included gender, race, and age, measured as of the index date. Race was grouped into White, Black, and Other categories.
Comorbidities that meet at least one of the following criteria were identified: a) Having been reported to be associated with migraine in the literature; b) usually involved with opioid use; c) often involved with emergency service usage. Each type of comorbidity was assessed as a binary variable (presence or absence of that diagnosis). Appendix A summarizes the identified comorbidities and their diagnosis codes.
Previous ED visits, ambulatory visits, and hospitalizations were defined as the number of that type of visit during the 6-month pre-index period based on the EHR encounter data.
Index date ‘opioid use’ was a binary variable representing whether or not the patient was administered any opioids during the index date ED visit. Previous opioid use was defined as the number of opioid prescriptions during the 6-month pre-index period. Previous opioid use was also categorized into different levels based on the number of prescriptions. In addition to opioids, acute medication use at the index dates were also described, including antiemetics, non-opioid analgesics (including NSAIDs), antiepileptics, triptans, ergots, corticosteroids, antihistamines, and others as summarized in the 2015 guideline for acute treatments of migraine by the American Academy of Neurology (AAN) and the American Headache Society (AHS) (see Appendix B) (11).
Previous preventive medication was considered as a binary variable, with “1” meaning the patient had at least one preventive medication during the 6-month pre-index period and “0” meaning they did not. Classification of preventive medication was based on the joint guidelines for migraine prevention in adults from AHS and AAN released in 2012 (see Appendix C) (15).
Statistical analyses
Descriptive statistics were used to summarize medication use at the index ED visits. Bivariate analyses, including t-tests, Chi-square tests, and Wilcoxon Mann-Whitney U tests were used to compare demographics, clinical characteristics, HRU, and previous opioid use between opioid users and non-opioid users. Multivariable logistic regression was used to examine the risk factors for opioid use at index ED visits. A stepwise method was used for selecting the variables in order to avoid redundant predictors. The probabilities to enter and remove from the model were both set at 0.15.
Data analyses were performed using SAS 9.4. For all statistical tests, a p-value of <0.05 was considered, a priori, to be statistically significant.
Results
Patients selection
A total of 12,945 adult patients with at least one migraine-related (ICD-9 346.xx or ICD-10 G43.xxx) or headache-related (ICD-9 784.0 or ICD-10 R51) ED visit between December 2013 and April 2017 were identified in the BSWHP EHR dataset. Among these, 788 patients ultimately met the inclusion criteria. Figure 1 presents the flow chart for patient attrition.

Sample selection.
Patient characteristics
Table 1 shows the demographic and clinical characteristics for the total study cohort as well as by opioid use groups. The average age of the study cohort was 44.5 (SD = 14.6) years old, and a majority were female (85.9%) and white (76.1%). There were no significant differences between index date opioid users and non-opioid users in age, gender, or race.
Demographics and clinical characteristics.

aBased on Chi-square test except for age (t-test). Significant results are highlighted in bold.
bAt least one cell has expected counts less than 5, so p-value from Fisher’s Exact Test was used.
The study cohort generally had a high burden of comorbid conditions. More than half of the patients had a diagnosis for anxiety (52.8%), depression (50.4%), and hypertension (51.0%). Other common comorbidities included chronic pain (47.5%), back pain (44.8%), headache (33.6%), and tobacco use disorder (33.6%). Compared to non-opioid users at the index date, opioid users were more likely to have a diagnosis for anxiety (58.0% vs. 49.9%, p = 0.03), back pain (50.9% vs. 41.4%, p = 0.01), chronic pain (55.1% vs. 43.2%, p = 0.001), and sleep disorder (35.7% vs. 24.4%, p = 0.007).
Baseline health resource utilization
Table 2 summarizes health resource utilization for the study cohort within the 6-month baseline period. During the pre-index period, about two-thirds (n = 477, 60.5%) of the patients had one or more migraine-related ED visits and 4.9% (n = 39) had three or more migraine-related ED visits. In addition, more than one-third (n = 285, 36.2%) of the patients had one or more migraine-related ambulatory visits, and about one-fifth (n = 163, 20.7%) of the patients had one or more migraine-related hospitalizations. For all-cause utilization, the majority of the patients had at least one ED visit (n = 650, 82.5%) and at least one ambulatory visit (n = 704, 89.3%). More than a quarter of the patients (n = 227, 28.8%) had at least one all-cause hospitalization.
Health resource utilization in 6-month pre-index period, n = 788.
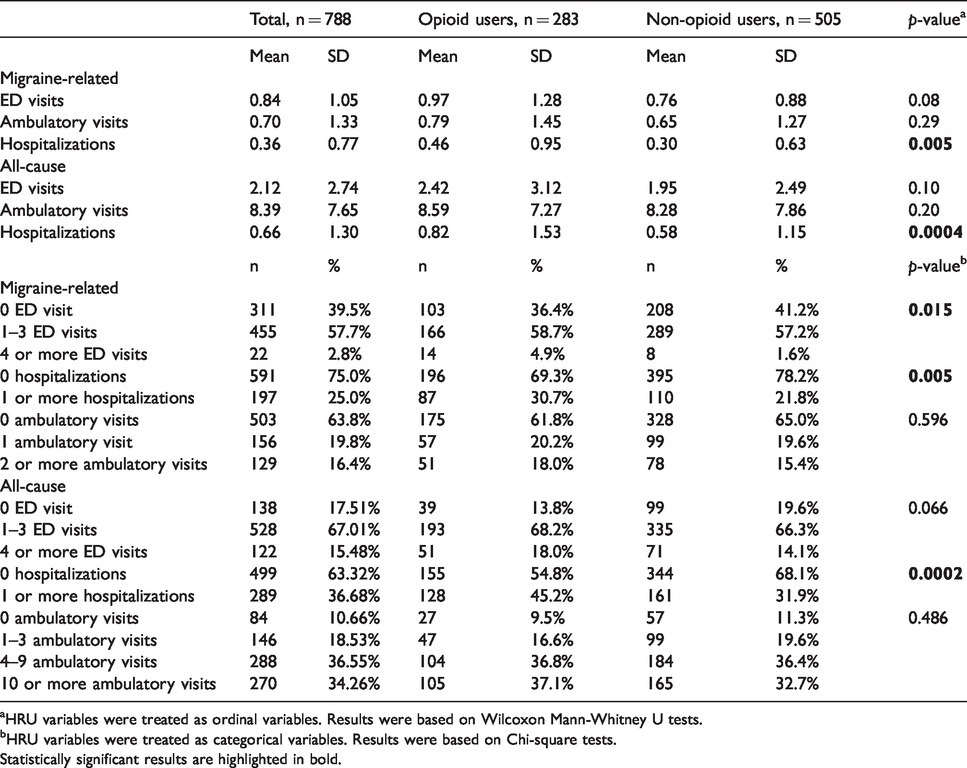
aHRU variables were treated as ordinal variables. Results were based on Wilcoxon Mann-Whitney U tests.
bHRU variables were treated as categorical variables. Results were based on Chi-square tests.Statistically significant results are highlighted in bold.
Compared to non-opioid users, opioid users had significantly (p < 0.05) more migraine-related ED visits, more migraine-related hospitalizations, and more all-cause hospitalizations during the 6-month pre-index period (Table 2).
Medication use at ED visits
Opioid and non-opioid medication use during index date ED visits are summarized in Tables 3 and 4. Prescriptions written to be filled at a pharmacy after the ED visit are summarized in Table 5. A total of 671 of 788 patients (85.2%) received ≥1 medication during their index date ED visits. More than one third (n = 283, 35.9%) of the patients received ≥1 opioid medication, and more than half (n = 464, 58.9%) received ≥1 non-opioid acute medications (including patients who received both). Morphine (13.1%) and hydromorphone (10.8%) were the two most commonly administered opioids during the index ED visit, followed by fentanyl (9.0%), hydrocodone (5.8%), and butorphanol (1.6%). In addition, some patients were given prescriptions to be filled at a pharmacy after their ED visit. Nearly half of the patients (n = 370, 47.0%) had take-home prescriptions, among which 118 (15.0%) patients had ≥1 opioid prescription.
Commonly used drug classes during index date ED visits.

*614 of 788 patients had at least one medication at ED visit.
Opioid use during index date ED visits.

Prescriptions written to be filled at a pharmacy after index date ED visits.

*370 of 788 patients had at least one prescription written to be filled at a pharmacy.
As for non-opioid acute medications, antiemetics were the most commonly used medication during the index date ED visit (n = 292, 37.1%), followed by non-opioid analgesics (n = 246, 31.2%), antihistamines (n = 153, 19.4%), and corticosteroids (n = 74, 9.4%).
Baseline opioid use
Previous opioid use during the 6-month pre-index period is summarized in Table 6. The median number of all-cause opioid prescriptions used previously was 3.0, and the median number of migraine-related opioid prescriptions used previously was 1.0. Over one-third (n = 296, 37.6%) of the patients had more than one migraine-related opioid prescription during the pre-index period. For all-cause opioid use, nearly two thirds (n = 514, 65.2%) of the patients had more than one opioid prescription in the previous 6 months.
Opioid use in 6-month pre-index period, n = 788.
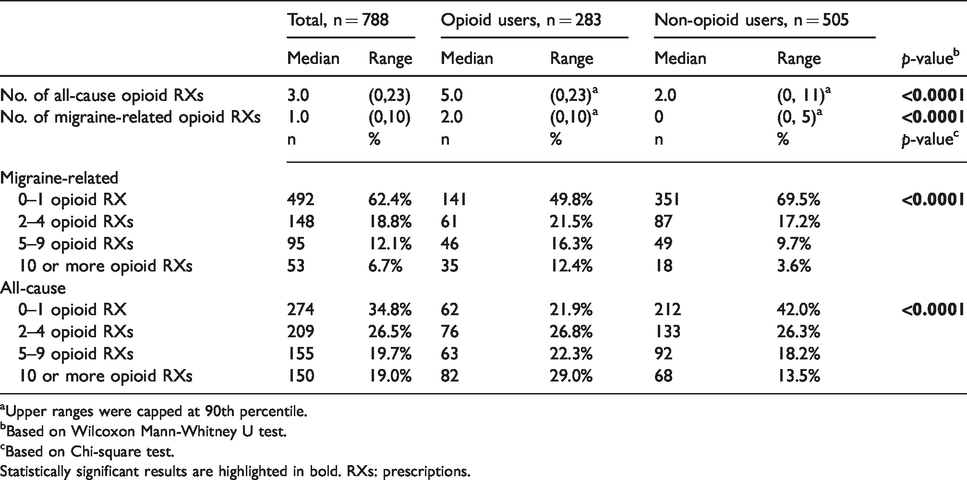
aUpper ranges were capped at 90th percentile.
bBased on Wilcoxon Mann-Whitney U test.
cBased on Chi-square test.Statistically significant results are highlighted in bold. RXs: prescriptions.
Compared to non-opioid users, opioid users at the index date had significantly (p < 0.0001) higher past opioid use, for both migraine-related and all-cause use (Table 6).
Predictors of opioid use at ED visits
The results of the multivariable logistic regression using stepwise selection are presented in Table 7. The overall model was statistically significant based on the likelihood ratio test (χ2 = 73.67, degree of freedom (df) = 14, p < 0.0001). Significant predictors of index date opioid use included previous migraine-related opioid use, previous non-migraine-related opioid use, previous all-cause ED visits, age, a diagnosis for sleep disorder, and a diagnosis for arrhythmia. Specifically, compared to patients who had no more than one migraine-related opioid prescription during the baseline period, patients with 2–4 prescriptions had 1.66 times the odds of receiving opioids at their index date ED visit (OR = 1.66, 95% CI = 1.11–2.47, p = 0.014), controlling for other listed variables. Similarly, patients with 5–9 prescriptions had 2.12 times the odds of receiving opioids at their index date ED visit (OR = 2.12, 95% CI = 1.31–3.45, p = 0.002), controlling for other listed variables. And patients with 10 or more prescriptions had 4.43 times the odds of receiving opioids at their index date ED visit (OR = 4.43, 95% CI = 2.27–8.64, p < 0.0001), controlling for other listed variables. Compared to patients without any previous ED visits, patients with 1–3 previous all-cause ED visits were 84% more likely to receive opioids during their index date ED visit (OR = 1.84, 95% CI = 1.17–2.91, p = 0.009), while holding other variables constant. As for age, compared to patients aged between 18 and 44 years old, patients who were 45 to 64 years old were 45% more likely to receive opioids at their index date ED visit (OR = 1.45, 95% CI = 1.02–2.05, p = 0.038), while holding other variables constant. In addition, patients with a diagnosis for sleep disorder were 43% more likely to receive opioids at their index date ED visit compared to patients without a sleep disorder diagnosis (OR = 1.43, 95% CI = 1.01–2.01, p = 0.041). The only significant variable that was negatively associated with index date opioid use was a diagnosis for cardiac arrhythmia. To be more specific, patients with a diagnosis for cardiac arrhythmia were 47% less likely to receive opioids during their index ED visit compared to patients without a cardiac arrhythmia diagnosis (OR = 0.53, 95% CI = 0.34–0.84, p = 0.006).
Multivariable logistic regression model with stepwise selection for risk factors of opioid use during index date ED visits, n = 788.

aReference group is 0–1 non-migraine-related pre-index opioid RXs.
bReference group is 0–1 migraine-related pre-index opioid RXs.
cReference group is 0 all-cause pre-index ED visits.
dReference group is age 18–44.
eReference group is patients who did not have a diagnosis for acute myocardial infarction.
fReference group is patients who did not have a diagnosis for sleep disorder.
gReference group is patients who did not have a diagnosis for cardiac arrhythmia.
hReference group is patients who did not have a diagnosis for stroke.Statistically significant results are highlighted in bold. RXs: prescriptions.
Discussion
Research incorporating real-world evidence on treatment patterns and health resource utilization among migraine patients presenting to emergency departments can provide insight into identifying high-risk populations and optimizing treatment decisions. This study used a well-defined study cohort to comprehensively describe the clinical characteristics, HRU, and medication use among migraine patients during ED visits. In addition, to the best knowledge of the authors, this study is one of the first that simultaneously examined multiple potential predictors for opioid use among migraineurs at emergency settings.
Demographics and clinical characteristics
The study cohort had an average age of 44.5 (SD = 14.6) years, and the majority were female (85.9%). Similarly, previous studies reported that migraine was more prevalent in middle-aged populations than other age groups, and, compared to men, women were three times more likely to have a migraine diagnosis (2,4–6).
In terms of clinical characteristics, consistent with previous findings, this study found that migraine patients were more likely to suffer from anxiety and depression than people who do not have migraine. To be more specific, 52.8% of the patients in this study cohort had a diagnosis for anxiety compared to 18.1% in the general population, and 50.4% of the patients had a diagnosis for depression compared to 6.7% in the general population. Similarly, in 2015, the American Migraine Foundation announced that more than half of migraineurs (50–60%) had anxiety (20). And it was noted by the Anxiety and Depression Association of America (ADAA) that about 40% of migraineurs had depression (21). The underlying biological mechanism between migraine and mental disorders requires further investigation but, generally, it was believed to be a bidirectional relationship influenced by both genetic and environmental factors such as stress and alcohol (22–24).
In addition to mental disorders, this study found that more than half (51.0%) of the patients had a hypertension diagnosis in contrast with a prevalence rate of 29% in the general population (25). Moreover, a small proportion of patients were diagnosed with stroke (2.3%) and acute myocardial infarction (1.0%). Some previous studies had proposed multiple explanations for the relationship between migraine and cardiovascular diseases (CVD). One possible explanation is that the decrease of endothelial progenitor cells in migraineurs indicates a reduction in migratory capacity and a higher cellular senescence than in other people (26).
Lastly, this study found that more than one quarter (28.4%) of the patients had a sleep disorder diagnosis. This result is expected given the fact that the underlying mechanisms between migraine and sleep disorders have been extensively explored in the literature (27,28).
Health resource utilization
As for migraine-related ED visits, about three-fifths (60.5%) of the study cohort had one or more visits in the 6-month pre-index period, and 2.8% of the total patients had more than three ED visits. Compared to index date non-opioid users, opioid users had significantly more migraine-related ED visits (Table 2). There are limited studies on migraine treatment at emergency departments, but the high utilization of EDs among migraine patients has been reported in the AMPP study, which found that migraineurs accounted for the majority (95.1%) of all the headache-related ED visits (17).
As for hospitalizations, approximately one-fifth (20.7%) of the study cohort had one or more migraine-related hospitalizations, and 28.2% of the cohort had one or more all-cause hospitalizations. Compared to non-opioid users, opioid users had significantly more hospitalizations (Table 2). The high use of inpatient visits has been reported by one study from AHRQ (Agency for Healthcare Research and Quality), which indicated that migraineurs accounted for 63.1% of the hospitalizations with headache disorder as the first diagnosis (29). A 2018 study (44) on healthcare utilization among migraine patients using Truven data found that 8.6% of migraine patients had at least one all-cause hospitalization compared to 2.9% in the matched non-migraine group in the past 12 months. Our results show higher hospitalization use than this study. One possible explanation is that the patients in our study represent a selection of more severe or otherwise more disabled patients. This can be indicated by comparing the patient comorbidity profile of the two studies (44).
Opioid and other medication use
Consistent with some previous studies, frequent use of opioids during ED visits was also found in this study. More than one third (35.9%) of the study cohort received opioids (combinations included) during their index date. In addition, 15% of patients had opioid prescriptions to be filled at a pharmacy after index ED visits. Similarly, Young et al. conducted a multicenter study in 2015 and reported that 35.8% of the ED visits among migraineurs resulted in opioid prescriptions (30). Another study, which was conducted by Friedman et al. using 2010 NHAMCS data, found that opioids were used in nearly three fifths (59%) of the migraine-related ED visits (31). The higher usage of opioids in that study compared to our study has three possible explanations. First, according to a CDC report, the general opioid prescribing rates in America were highest from 2010 to 2012; as more and more providers realize the risk of opioid overdose, opioid prescribing has decreased since then (32). Second, the 2014 guidelines clearly point out that opioids should be avoided for acute treatment of migraine (11). Moreover, this study enrolled patients from Texas, which on average has a lower level of prescription opioid usage than the overall US rates represented by the NHAMCS data (33). Despite these differences, our results indicate that opioid use among migraine patients at EDs remains high and further actions are needed to ensure guidelines are followed in practice.
In terms of opioid types, morphine, hydromorphone, and fentanyl were found to be the three most commonly used opioids in this study. Similar results have been found in other studies (30,31). One possible reason is that these three types of opioids are less toxic and can provide more rapid pain control than other opioid options (43), and physicians are more comfortable or familiar with using them.
The high use of opioids could be influenced by multiple factors. Possible explanations include: a) Some patients might believe opioids are helpful in pain relief and insist on using them; b) Physician prescribing behavior should also be taken into consideration. Physicians in the ED might have less incentive to say “no” to requests for opioids. c) Patients might have concerns or a history of adverse effects or poor response to other acute medications; d) Some physicians might not be familiar with alternative acute medications, or there is a lack of consistency in the ED protocols; e) This could also imply that there is a lack of evidence on effective acute medications specifically for ED settings.
In terms of medications other than opioids, antiemetics and non-opioid analgesics were shown to be most commonly administered, used by 37.1% and 31.2% of the study cohort respectively. Similarly, Young et al. found that these two drug classes were the most frequently used acute treatments for migraineurs at EDs, with 33.3% and 23.6% of all the prescriptions being antiemetics and non-opioid analgesics respectively (30).
Antihistamines were found to be used by nearly 20% of the migraine patients during their ED visits. This is likely to happen because diphenhydramine and promethazine were categorized as antihistamines in this study. These two medications are commonly used in combination with other medications (including opioids) for the treatment of migraine. Similar results have been found in the 2010 NHAMCS study (31), which reported that promethazine was used in 33% of the migraine ED visits.
Surprisingly, we found only three patients (0.4%) received triptans during their index ED visits, and four patients (0.5%) had triptans prescribed to take home after index ED visits. Similarly, the 2010 NHAMCS study (31) also found the use of triptans was uncommon, administered in 7% of all the ED visits. According to the guidelines (11), triptans are “effective” acute treatments. For patients presenting to the ED, sumatriptan is best studied and “should be offered” based on the ED-specific guidelines by Orr et al. (10), although with conflicting results. One possible reason for low triptan use is that triptans have been shown to be more effective in patients with early migraine attacks and are less effective in patients with moderate to severe migraines (40). In addition, contradictions to the use of triptans are common, including cardiovascular diseases, uncontrolled hypertension, and pregnancy (40,41). Moreover, ED-based clinical trials found that about 50% of the patients experienced adverse effects after using subcutaneous sumatriptan (42). Last, but not least, some patients might have a history of poor response to triptans, which also makes physicians less likely to prescribe triptans for these patients. Due to common side effects, lack of ED-based evidence on efficacy and safety, and concern of contradictions, some physicians believe that triptans are of limited use for migraine patients presenting to the ED (41).
Another interesting finding is that some patients did not get any pain medications (opioids or non-opioid analgesics) during migraine-related ED visits. Potential explanations include: a) Patients were identified as at risk of drug-seeking behavior and physicians decided not to prescribe any pain medications; b) the EHR dataset used in this study included a list of diagnoses for an encounter, but not in a specific order. This means that we selected the ED visit with a diagnosis of migraine but the patient might have other diagnoses at that same visit, and we do not know which diagnosis is primary. Thus, there is a possibility that a patient was mainly treated for a non-pain-related condition and did not receive pain medication; c) the ED visit was transferred into hospitalization and was classified as an inpatient visit in this study, so some patients might be given pain treatments after they moved to inpatient settings.
Preventive medications were found to be used by 39.5% of the study cohort during the 6-month pre-index period, and the proportion of patients who received preventive medications with a Level A recommendation (15) (including divalproex sodium, sodium valproate, topiramate, metoprolol, propranolol, timolol, and frovatriptan) was less than one quarter of all patients (23.7%). Preventive medication use was not significantly related to index date opioid use after controlling for other risk factors. One thing to note is that these results included coincident users (used preventive medications for disease other than migraine such as depression and hypertension) and adherence rates were not measured. Thus, it is very likely that the real proportion of patients who took preventive medications on a regular basis was lower. The AMPP study estimated that as many as 38% of migraineurs need preventive medication whereas only 12.4% were currently users (16). Our study supports the fact that prophylactic medications were not commonly used by migraineurs as recommended by the guidelines.
Predictors for receiving opioids at the ED
This study is one of the first to explore and quantify the relationship between opioid use among migraineurs and multiple predictors of use specifically at emergency settings, including past opioid use, past preventive medication use, past HRU, baseline clinical characteristics, and demographics. After controlling for all other variables (Table 7), past opioid use was found to be a strong predictor of index date opioid use, and the strength of this association increased as the frequency of opioid use in the past increased.
In addition, this study found that past HRU is a potential driver for future opioid use. Specifically, patients who had one to three past ED visits were 1.8 times more likely to be given opioids during index ED visits than patients who had no past ED visits. Consistently, the AMPP study, which was a nationwide survey study, also reported a positive relationship between opioid use and HRU (34).
As for comorbidities, some previous studies have found an association between sleep disorder and opioid use in patients with chronic pain (35,36). A similar positive relationship was found in this study, and this association remained significant after controlling many other factors (Table 7). Additional evidence from future research is needed to support the generalizability of this result. Interestingly, this study identified a negative association between cardiac arrhythmia and opioid use. One possible explanation is that physicians were cautious when using opioids on patients with irregular heart rhythms, given that a negative impact of opioids on heart rhythms had been found in the literature (37,38).
Although a valid EHR dataset from real-world settings was used, this study is subject to several limitations. Firstly, although associations were demonstrated, casual relationships cannot be established given the retrospective nature of this study, and variables of interest were limited by the availability of the dataset. Secondly, patients might not use medications as prescribed, especially for the take-home prescriptions. Thirdly, HRU may be underreported, as services received outside BSWHP systems were not captured. Fourthly, the dataset used in this study only included patients from Central Texas where a majority of the population is White. Thus, results from this study might not be generalizable to patients in other racial groups, living in other regions, or enrolled in different health plans. Next, the way of identifying comorbidities in this study might lead to under or over-ascertainment (39). Moreover, opioid use was not quantified in terms of morphine milligram equivalence (MMEs), which means the dosage of opioid use was not captured. Moreover, although multiple risk factors for opioid use were identified in this study, it is important to note that these results could be biased by physicians’ beliefs or prescribing habits versus patient characteristics. In addition, this study applied multiple statistical tests simultaneously, which raised the probability of making a type I error. Last, but not least, logistic regression models with many variables usually require a larger sample size, and there is a potential lack of power to evaluate some predictors included in the analysis.
Conclusion
In this retrospective study of migraine patients, opioids were found to be one of the most common medications given at emergency settings, used by more than one third of migraineurs. Overall, the health resource utilization for migraine patients was high and more than half had diagnoses for mental disorders and hypertension. Predictors of opioid use at the index ED visit include past opioid use, past ED visits, and some comorbidities (e.g. sleep disorder). Future studies may evaluate the generalizability of these findings in a more diverse population (e.g. pediatric or elderly), in different regions or cultures (e.g. South America or Asia), as well as explore additional factors such as a patient’s health behavior, adherence to prophylactic medication, and disease severity. In addition, with the availability of emerging treatments, including ubrogepant, rimegepant, and lasmiditan for acute treatments as well as erenumab, fremanezumab, galcanezumab, and eptinezumab for preventive treatments, the study results might be expected to change with more current data. This study supports the need for treatment optimization at emergency settings and may provide insights into identifying migraineurs with a high potential of opioid use.
Article highlights
The five most frequently used medications for migraine patients presenting to the emergency departments (EDs) were antiemetics, opioids, non-opioid analgesics, antihistamines, and corticosteroids. More than one third (35.9%) of the migraine patients received opioid medications during their migraine-related ED visits and 15% of patients had opioid prescriptions written during the ED visit to be filled at a pharmacy, indicating a gap between guideline recommendations and real practice. Previous opioid use (both migraine-related and non-migraine-related), previous ED visits, age, and diagnosis of sleep disorder might help identify migraine patients with high risk of opioid use.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.