
Abstract
Introduction
YouTube is the most widely used video hosting website in the world; however, the quality and reliability of information is unknown. The aim of this study is to evaluate the content and distribution of the most popular videos on YouTube about migraine.
Methods
We searched for migraine-related videos on the online video hosting resource YouTube (http://youtube.com/). Two authors screened the titles and video descriptions independently for all videos with a view count of ≥ 10,000 views. For each video we recorded descriptive data, the source/author and the primary purpose/content.
Results
We identified 351 eligible videos. In total, there was more than 3 days of content viewed more than 163 million times. Only 9% of these videos were authored by healthcare professionals. The majority (44%) of videos focused on complementary and alternative medicine.
Discussion
YouTube provides a wide array of easily accessible information on migraine, ranging from authoritative sources to potentially questionable content. If used uncritically, this may result in inadequate clinical management. Peer-reviewed information on migraine mechanisms and treatment is needed to provide the best available evidence for the public and patients. Ideally, a professional society or foundation such as the International Headache Society would develop, curate, and distribute content.
Introduction
Migraine is the leading cause of years lived with disability among individuals between 15–49 years (1). While the high prevalence of migraine suggests that there is readily available health information on the subject, migraine literacy appears to be poor (2). Furthermore, migraine continues to be poorly understood, underdiagnosed and undertreated (3–5).
In both America and Europe, health information is one of the most frequently searched topics on the internet (6–8). More than 50% of North Americans access health information online on a monthly basis, and many patients view the internet as a valuable and reliable source of health-related information and consult it before seeking a professional diagnosis (9,10). While there are undoubtedly many benefits to easily accessible health information, the possibility of misinformation leading to unfortunate actions or psychological distress is a concern. The available information is also very diverse as everyone, including non-health care providers, can easily share their opinions online. Patients seeking information are in general not trained to evaluate medical information, and clinicians should be mindful of potential misunderstandings.
YouTube is the most widely used video hosting website in the world and it is the second most popular website in the world after Google. It has over a billion users and a large part of its traffic originates directly from search engines and social media networks such as Facebook (11). The diversity of content on YouTube very much reflects that everyone can upload videos, which may lead to the dissemination of questionable content.
The aim is to evaluate the content and distribution of the most popular videos on YouTube about migraine.
Methods
Search strategy
We conducted a review of the most popular migraine-related videos on the online video hosting resource YouTube (http://www.youtube.com) (Figure 1). We used the Mozilla Firefox browser (Mozilla Foundation) with all tracking cookies deleted and the “Private Window” function enabled. These two factors make the browser appear as a naive user. We conducted the search on 21 August 2019, using the search term “migraine”, and sorted the videos by view-count. Two authors (HS, TPD) screened the titles and video descriptions independently for all videos with a view count of ≥ 10,000 views. The rationale for a cut-off of ≥ 10,000 views is that most people doing an online search will look no further than the first three pages generated (12). We resolved any disagreement by consensus between the authors and included a third author (MA) if necessary. We excluded videos considered irrelevant to migraine, which had poor audio-visual quality, or were duplicates.

Overview of the screening and inclusion process.
Video analysis
We viewed all screened videos in their entirety. For each video we recorded descriptive data, the source and the primary purpose.
For descriptive data, we recorded the following parameters: (i) Title; (ii) Publication date; (iii) Number of views; (iv) Duration of the video; (v) Number of “likes”; (vi) Number of “dislikes”; (vii) Number of comments.
For source, we used the following categories: (i) Healthcare professional; (ii) Non-medical professional; (iii) Patients; (iv) Pharmaceutical industry; (v) Non-governmental/Non-profit organization; (vi) Healthcare institution; (vii) University institution; (viii) Other. The category “Other” as source is further subdivided into categories by how the authors of the videos identify themselves. If there was no clear description of the author, we subcategorized the source of the video as “Unknown”. If there was a description of the video channel but no clear definition of the author, we subcategorized the source of the video as “Unclear”.
Regarding primary purpose, we categorized according to the following groups: (i) Complementary and alternative medicine (CAM); (ii) Education; (iii) Entertainment and news; (iv) Politics; (v) Advertisement; (vi) Personal; (vii) Other. The category “Complementary and alternative medicine” is further subdivided into type of practitioner/intervention as defined by the video author. We subcategorized as “Unknown” if the intervention is not described.
We assessed the technical quality of videos; that is, video and sound. In each, the grade ranges from 1 to 3 where 1 is poor, 2 is fair and 3 is good. For the video quality, grade 1 represents unclear or blurry visuals that are difficult to understand. Grade 2 represents a standard video quality of less than 1080p resolution, but with clear visuals and standard text clarity typical of homemade videos. Grade 3 represents at least 1080p resolution with sharp and clear text and visuals with professional effects. For the audio quality, grade 1 represents no audio. Grade 2 represents difficulty in understanding the speech and disrupting background noise. Grade 3 represents no trouble understanding the spoken words and music (13).
We evaluated the interaction with the videos based on the interaction index defined as

Statistical analysis
We collected the data in an Excel spreadsheet in Microsoft Excel (Microsoft). We used Microsoft Excel for analysis of the frequency of source and purpose. We used the SPSS software (SPSS version 26; SPSS Inc.) for descriptive data analyses; that is, mean, median, range, and sum.
Ethics statement
The study did not require the approval of a scientific ethics committee as the data is publicly available.
Data availability statement
Any data not published within this article for this study is available by request from any qualified investigator.
Results
The initial search strategy resulted in 607 videos. After applying our cutoff of ≥ 10,000 views, we identified 393 videos, two of which were duplicates. The remaining 391 videos were screened and 40 of them were excluded as they were unrelated to migraine. That left 351 videos to be viewed in their entirety and none of them were excluded. Thus, the final study dataset included 351 videos.
The accumulated duration of the videos is 4790:16 minutes. In total, the videos have been viewed 163,692,743 times, have been commented on 173,148 times, have 1,709,411 “likes”, and 73,154 “dislikes”. The YouTube video quality in terms of video and audio quality had a mean score of 2.3 and 2.9, respectively. We did not formally assess validity as there is no accepted standard criterion for YouTube video quality. A complete overview of the descriptive data is presented in Table 1.
Descriptive data of the videos.

Most of the videos, 207/351 (59%), had “Other” as source. This was followed by “Non-medical professional”, 37/351 (11%); “Healthcare professional”, 33/351 (9%); and “Patients”, 26/351 (7%) (Figure 2). “Healthcare professional” consisted of 26 (79%) medical doctors, four (12%) nurses, one (3%) psychologist, one (3%) dentist, and one (3%) optometrist. The category “Other” is further subdivided and presented in Table 2.

The distribution of migraine-related videos according to source.
The subcategories of the source “Other”.

For the purpose of the videos, “Complementary and alternative medicine” accounted for 156/351 (44%). This was followed by “Education”, 84/351; (24%) and “Entertainment and news”, 66/351 (19%) (Figure 3). The category “Complementary and alternative medicine” under purpose is further subdivided into type of practitioner/intervention (Table 3).
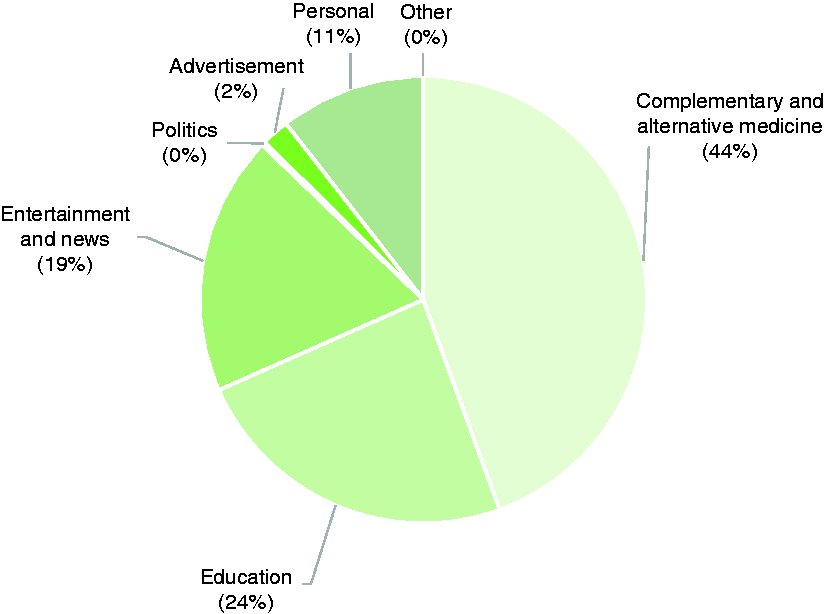
The distribution of migraine-related videos according to purpose.
Complementary and alternative medicine according to content.

Most of the videos with “Healthcare professional” as source, were primarily videos about “Education”, covering 27/33 (82%). The rest of the videos with “Healthcare professional” as source was about “Complementary and alternative medicine, 5/33 (15%) and “Entertainment and news”, 1/33 (3%).
We calculated the mean, median and range of the interaction index for source. We excluded seven videos as the number of “likes” and “dislikes” were hidden; thus, the interaction index could not be calculated for these videos. This included 1/33 (3.03%) videos of “Healthcare professional”, 2/7 (28.57%) videos of “Pharmaceutical industry”, 1/2 (50%) videos of “University Institution” and 3/207 (1.449%) videos of “Other”. The mean interaction index for “Healthcare professional” is 1.29 (median: 0.53; range: 0.07–5.78); for “Non-medical professional” is 1.05 (median: 0.72; range: 0.09–3.22); for “Patients”, is 1.34 (median 1.11; range: 0.13–5.09); for “Pharmaceutical industry” is 0.31 (median: 0.08; range: 0.01–0.8); for “Non-governmental organization/Non-profit organization” is 1.12 (median: 0.73; range: 0.03–4.61); for “Healthcare institution” is 0.57 (median: 0.37; range: 0.002–2.10); for University institution is 0.59 (median: 0.59; range: 0.59–0.59); and for “Other” is 1.14 (median: 0.73; range: 0.011–11.84).
Discussion
This study demonstrates that YouTube has a large amount of content related to migraine that is readily available to patients and others. Most of the videos were distributed by “Other” and the majority of the purpose/content of the videos was related to “Complementary and alternative medicine”.
The results of the study have implications for patients as well as healthcare professionals. Patients searching online for information about migraine have a tremendous amount of information to evaluate. We identified more than 3 days of content on YouTube alone and the videos have been viewed more than 163 million times (Table 1). While we cannot rule out that this number may be influenced by persons viewing the same videos several times, or the opposite, that people stop watching the videos before it ends, we believe we can safely assume that this does reflect a great interest in video material about migraine. However, while educational videos do exist on YouTube, most of the content is related to complementary and alternative medicine (Figure 3). Most of the content of complementary and alternative medicine is related to general and non-evidence-based solutions including diets and music therapy.
Furthermore, only about one-fourth of the videos in total have been distributed by healthcare professionals, university institutions, and healthcare institutions (Figure 2). Without a clinical background to evaluate the videos, most patients will be unable to determine the veracity, reliability, or safety of the information shared. A possible explanation for why videos about complementary and alternative medicine (CAM) are the most viewed is that health consumers highly value this approach (14). More than 60% of the global population uses some form of traditional medicine and the global CAM market size is estimated to be worth approximately USD 60 billion and is expected to grow to more than USD 210 billion by 2026 (15). It is also possible that a substantial proportion of patients may not have adequate health insurance and rely to a greater extent on CAM. It should also be kept in mind that alternative medicine does not require a prescription, which may increase the amount of direct consumer marketing. A third (and unfortunate) explanation could be the high cost associated with pharmacological or device treatments even for those with health insurance, or patient dissatisfaction with conventional health care providers and allopathic treatments (9,16). A fourth explanation could be inadequate physician-patient communication and information about the cause and treatment of migraine (3,16).
The category “Other” accounts for the majority of sources (Table 2) and reflects a broad diversity of authors with very different backgrounds. This contributes to the fact that patients using the internet cannot be guaranteed that the content of these videos has valid information as every person is able to upload videos on YouTube. As for healthcare professionals, most of the authors are medical doctors, followed by nurses, which shows an interest in YouTube as a source of patient-oriented information among some healthcare providers. This demonstrates the potential for video-sharing websites to be a source of scientifically accurate and evidence-based healthcare-provided information that could lead to informed decisions by patients.
The interaction index calculated for the source shows that the category “Patients” has the highest mean in interaction index at 1.34 followed by “Healthcare professional”, with a mean at 1.29 and “Other”, with a mean of 1.14. The lowest mean in interaction index at 0.31 accounted for “Pharmaceutical industry”. Videos of single individuals rather than groups or organizations have a higher mean in interaction index except for “Non-governmental organizations/Non-profit organization”. This may again reflect that patients prioritize anecdotal information for treatment choices (14).
The vast interest in migraine-related videos reported by number of views documented by our study demonstrates the potential of YouTube as an educational and clinical platform for migraine education and treatment. This should be viewed in the context that the majority of health-related internet searches by patients are for specific conditions and primarily carried out to manage their own healthcare independently and/or to decide whether they need professional help (9). Online video platforms such as YouTube are widely used and accessible and therefore potentially useful as an educational tool for learning or teaching. Furthermore, these videos may be used for reassurance to confirm detailed information provided by a healthcare professional during a clinical encounter (9).
Study limitations
The major limitation is that this is a cross-sectional study, while the content on YouTube is constantly being updated. However, all studies investigating online content will have this limitation. Another limitation of this review relates to the search strategy. The search term “migraine” excludes the majority of videos in other languages, whose content may differ from the videos we analysed. Furthermore, we cannot exclude regional differences in a Google search, though we believe the use of English search terms will limit potential differences. Furthermore, the geographical coverage of the videos is not provided.
Conclusion
Online consumer health information is widely popular but non-curated or vetted by healthcare professionals. People searching YouTube for information on migraine will encounter a wide array of information, ranging from authoritative sources to potentially questionable content. Our study shows that the most viewed videos on YouTube was related to non-evidence-based treatments, which ultimately may result in inadequate clinical management. The medical community should aim to distribute peer-reviewed information on migraine as a disease and clinical management using this and other media platforms. Professional societies and medical foundations that provide content vetted by experts are ideally situated to develop and disseminate such content. To begin with, we suggest that we should aim to address the most popular migraine-related topics in an alliance between headache experts and patient organizations.
Public health relevance
People searching YouTube for information on migraine will encounter a tremendous amount and diverse array of information with questionable content. Peer-reviewed information on migraine mechanisms and treatment is needed to provide the best available evidence for the public and patients. Ideally, a professional society or foundation such as the International Headache Society would develop, curate, and distribute content.
Footnotes
Acknowledgements
We thank the Lundbeck Foundation.
Author contributions
HS drafted the original manuscript; TPD conceptualized and drafted the original manuscript; JMH conceptualized and revised the manuscript for intellectual content; DWD conceptualized and revised the manuscript for intellectual content; MA conceptualized and revised the manuscript for intellectual content. Co‐investigators: None
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HS, TPD, and JMH report no disclosures. DWD reports the following conflicts: Personal fees: Amgen, AEON, Association of Translational Medicine, University Health Network, Daniel Edelman Inc., Autonomic Technologies, Axsome, Aural Analytics, Allergan, Alder BioPharmaceuticals, Biohaven, Charleston Laboratories, Clexio, Dr Reddy's Laboratories/Promius, Electrocore LLC, Eli Lilly, eNeura, Neurolief, Novartis, Ipsen, Impel, Satsuma, Supernus, Sun Pharma (India), Theranica, Teva, Vedanta, WL Gore, Nocira, PSL Group Services, University of British Columbia, XoC, Zosano, ZP Opco, Foresite Capital, Oppenheimer; Upjohn (Division of Pfizer), Pieris, Revance, Equinox, Salvia, Amzak Health. Speaking fees: Eli Lilly, Novartis Canada, Amgen. Speakers Bureaus: None. CME fees or royalty payments: HealthLogix, Medicom Worldwide, MedLogix Communications, Mednet, Miller Medical, PeerView, WebMD Health/Medscape, Chameleon, Academy for Continued Healthcare Learning, Universal Meeting Management, Haymarket, Global Scientific Communications, Global Life Sciences, Global Access Meetings, UpToDate (Elsevier), Oxford University Press, Cambridge University Press, Wolters Kluwer Health; Stock options: Precon Health, Aural Analytics, Healint, Theranica, Second Opinion/Mobile Health, Epien, Nocira, Matterhorn/Ontologics, King-Devick Technologies; Consulting without fee: Aural Analytics, Healint, Second Opinion/Mobile Health, Epien; Board of Directors: Epien, Matterhorn/Ontologics, King-Devick Technologies. Patent: 17189376.1-1466:vTitle: Botulinum Toxin Dosage Regimen for Chronic Migraine Prophylaxis, without fee; Research funding: American Migraine Foundation, US Department of Defense, PCORI, Henry Jackson Foundation; Professional society fees or reimbursement for travel: American Academy of Neurology, American Brain Foundation, American Headache Society, American Migraine Foundation, International Headache Society, Canadian Headache Society.
MA reports personal fees from Allergan, Amgen, Alder, Eli Lilly, Novartis and Teva; participated in clinical trials as the principal investigator for Alder, Amgen, ElectroCore, Novartis and Teva trials. MA has no ownership interest and does not own stocks of any pharmaceutical company; serves as associated editor of Cephalalgia, Headache, and co-editor of the Journal of Headache and Pain; and is the President of the International Headache Society and General Secretary of the European Headache Federation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Unrestricted research grant from the Lundbeck Foundation.