
Abstract
Background
Headache disorders comprise the three most prevalent medical disorders globally and contribute almost 20% to the total burden of neurologic illness. Although the experience of a recurrent headache disorder tends to be highly individualized, patient preferences tend to be a low priority in guidelines for the management of patients with headache.
Methods
In September 2017, the first Global Patient Advocacy Summit was convened, bringing together patients, patient advocates, patient advocacy organizations, healthcare professionals, pharmaceutical manufacturers, scientists, and regulatory agencies to advance issues of importance to patients affected by headache worldwide.
Results
Presentations and discussion covered multiple issues, such as improving access to appropriate medical care; incorporating the insights of independent patient advocates and advocacy organizations; leveraging the insights, experience and influence of leading health and neurological organizations; and raising awareness of the role of regulatory agencies in disease advocacy. Attendees agreed that it is important to understand and promote the global, regional, and local interests of people with headache disorders, as well as challenge the pervasive stigma associated with headache. They also agreed that those with severe, recurrent, or disabling headache disorders should have reliable access to competent medical care; healthcare professionals should have access to adequate training in Headache Medicine; global benchmarks should be established for accurate diagnosis and the use of evidence-based treatments in patients with headache; and that information is needed about consultation, diagnosis, and treatment of headache, particularly in regard to patient preferences.
Conclusion
Based on the group’s consensus around these issues, a series of statements was developed, and they are collectively presented herein as the Vancouver Declaration on Global Headache Patient Advocacy 2018.
Introduction
The World Health Organization estimates that the three most prevalent neurologic disorders worldwide are tension-type headache (1.5 billion), migraine (958.8 million), and medication overuse headache (58.5 million) (1). Collectively, these three disorders contribute approximately 17% to the global burden of neurologic diseases, with migraine the second most disabling disease overall (1,2). Cluster headache, often considered the most painful of the primary headache disorders (3–6), is associated with disability in 80% of patients (7), yet patients with this condition often wait several years and consult multiple healthcare professionals before receiving an accurate diagnosis (8,9). There are multiple therapeutic options with proven efficacy for most patients with any of the primary headache disorders, but access to practitioners with training in Headache Medicine is limited, diagnostic accuracy is inconsistent, and the use of evidence-based treatments is suboptimal (8–11).
In clinical practice, the management of chronic diseases such as migraine and cluster headache is challenging because of the highly variable acceptance, adherence, preferences, and response to treatment among patients (12). Moreover, the assessment of outcomes, processes, and other dimensions of care that matter most to patients remains limited (13). Thus, while the patient experience of a recurrent headache condition tends to be highly individualized and dynamic over time (14), evidence-based approaches are impersonal, rely on probabilities that are based on population responses, have static goals that may not align with patient preferences, and may underestimate the value patients place on nonmedical interventions, such as access to patient support groups (12,15). A review of clinical practice guidelines from a variety of disciplines found that less than 5% of the text and references dealt with patient preferences (16); the proportions are similarly low (<5%) in multiple guidelines for the treatment of primary headache disorders (17–23). The lack of prominence given to patient concerns in headache guidelines may help to explain why medical professionals tend to underestimate the high value patients place on nonpharmacologic aspects of therapy, such as answering questions about their condition, educating them about their illness, and teaching them how to treat and prevent attacks (24). What matters most to patients often is missed. The low priority assigned to patient preferences may also contribute to the sizeable proportion (∼33%) of patients with headache who report dissatisfaction with treatment (25,26). Despite the limited attention they are given in guidelines, understanding the factors that influence patients’ preferences increases the ability to choose appropriate therapy (27), and patients can help to identify and rank outcomes not previously deemed clinically relevant by researchers, clinicians, pharmaceutical manufacturers, and regulatory agencies (12).
In September 2017, as a formal recognition that patient perspectives on stigma, disease awareness, and the management of headache disorders should be obtained directly from patients and their advocates, the first Global Patient Advocacy Summit was convened in Vancouver, Canada. Hosted and organized by the International Headache Society and moderated by its then-President, David Dodick, the Global Patient Advocacy Summit brought together patient leaders, patient advocacy organizations, leading health, neurological and pain organizations, healthcare professionals, pharmaceutical manufacturers, scientists, and regulatory agency representatives from around the world with the goal of understanding and advancing issues that are important to headache patients. The topics presented and discussed included improving access to appropriate medical care; incorporating the insights of independent patient advocates and advocacy organizations from around the world; leveraging the experience and influence of leading health and neurological organizations; and raising awareness of the role of regulatory agencies in disease advocacy. The main outcomes of the Summit included general agreement that:
It is important to understand and promote the global, regional, and local interests of people with headache disorders, as well as challenge their pervasive stigma All patients affected by headache should have reliable access to competent medical care All healthcare professionals should have access to adequate training in Headache Medicine A global benchmark should be established to ensure that all patients affected by headache receive an accurate diagnosis and evidence-based treatments Information is needed about consultation, diagnosis, treatment of headache, and patient-reported outcomes (e.g. quality of life, satisfaction with treatment). Vancouver Declaration 2018 consensus statements and advocacy needs.
In addition, it was agreed that the group would develop and promote a series of consensus statements (Table 1) that reflect the priorities of Summit participants and set advocacy goals for the future. These consensus statements, and brief discussions of each, are presented below.
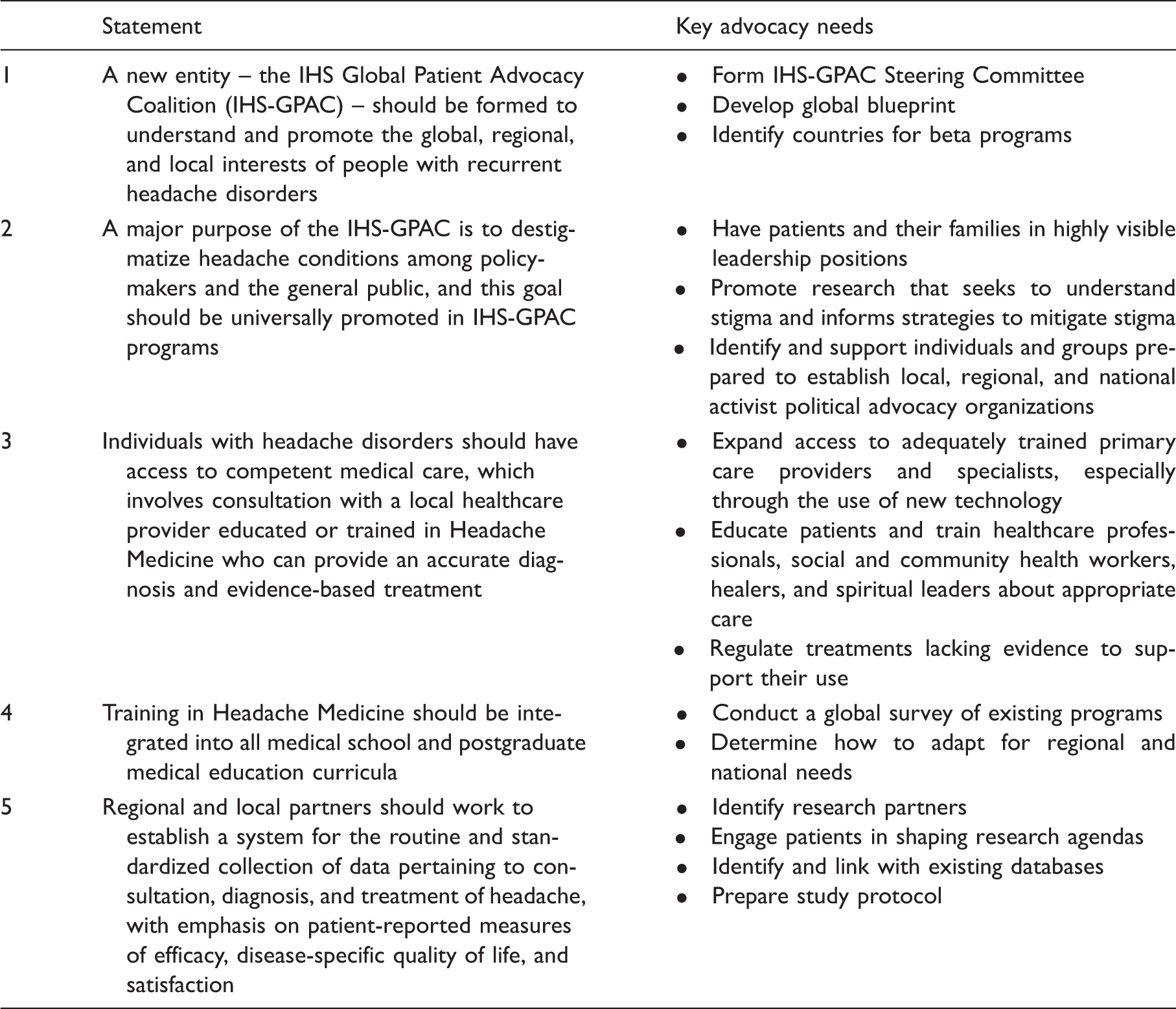
1. A new entity – the International Headache Society Global Patient Advocacy Coalition (IHS-GPAC) – should be formed to understand and promote the global, regional, and local interests of people with recurrent headache disorders
In other disease states, such as stroke (28–30), the establishment and periodic revision of global benchmarks has been helpful in improving the level of care and focusing attention on the priorities of patients. Participants at the Summit agreed to emulate this approach and form a Global Patient Advocacy Coalition (IHS-GPAC) that involves a wide range of stakeholders, including patient organizations and advocates, national and global health, neurological, pain and headache societies, regulatory agencies, and pharmaceutical manufacturers present at the Summit, as well as Health Technology Assessors and payers. It was proposed that the overall approach for the IHS-GPAC should be to create a centralized strategy that provides the vision and advocacy tools to country affiliates; develop impactful country specific strategies and tactics; measure progress and share best practices; and adapt success stories from global collaborators to local environments and needs. The initial objectives of the IHS-GPAC should be to establish an administrative structure and work to develop a global strategic blueprint for headache advocacy that can be implemented by regional and national partners. Summit participants agreed that IHS-GPAC messaging should be simple and relatable, perhaps drawing inspiration from previously successful advocacy initiatives (e.g. AIDS = rights; breast cancer = women; autism = family).
Initiatives administered under the auspices of the IHS-GPAC should adopt the best practices of advocacy initiatives developed by the American Academy of Neurology, the World Health Organization, the World Federation of Neurology, and the Alliance for Headache Disorders Advocacy, as well as the successful efforts of patient organizations (e.g. Migraine Association of Ireland, European Headache Alliance, American Migraine Foundation) and individual advocates. The organizational and operating strategies of the World Health Organization – in which global efforts are directed at providing normative guidance, regional initiatives focus on the delivery of services and public goods, and supporting countries tailor the guidance and services within the relevant context of respective Member States to create actual changes – may be a useful model. As the World Health Organization is endeavoring whole-of-system, whole-of-government, whole-of-society approaches so as to fit in the new context of the Sustainable Development Goals, engagement of stakeholders is critical, including partnership with local patient groups that gather and share information, provide day-to-day interaction, and support and serve as “laboratories” for pilot programs and ideas. Whenever possible, work at the regional and national levels should include collaborations with representatives from ministries of health, regulatory agencies, manufacturers, and payers, who should be viewed as partners in promoting patient interests in the policymaking process, in clinical research, and in unsupervised settings.
2. A major purpose of the IHS-GPAC is to destigmatize headache conditions among policymakers and the general public, and this goal should be universally promoted in IHS-GPAC programs
The stigma of headache is directly responsible for needless suffering among patients and caregivers, as well as for the perennial lack of resources that shortchanges headache research and restricts access to optimal care worldwide. Evidence suggests that patients with headache have been stigmatized by healthcare professionals who view them as drug seekers with a nonserious disease; family and friends who fail to appreciate their suffering; educators, employers, and insurers who believe headache should not lead to performance decrements or absence; and policymakers who consistently underfund research into treatments that might benefit them (31). As a result, the IHS-GPAC should work to educate and reassure patients that having a headache condition is not a cause for shame or isolation, but an important connection with others in a similar situation, as well as with a powerful global network of advocates that consistently promotes their long-term interests while meeting their immediate needs by helping them manage their illness successfully. People with recurrent headache disorders, especially those from underserved communities, should feel adequately empowered not only to acknowledge their illness publicly, but also to demand equitable access to the best therapies available. At the same time, policymakers should be consistently reminded that the effects of headache disorders are widespread, profound, and worthy of consistent and meaningful support.
The concept of stigma should be incorporated into IHS-GPAC programming whenever possible, with the understanding that the manifestations, magnitude, and deleterious consequences of stigmatizing attitudes towards individuals with disabling headache disorders may differ markedly between societies. To maximize the chances of success, IHS-GPAC initiatives should have patients and their families in highly visible leadership positions, with the precise roles for healthcare professionals, regulators, payers, government officials, healthcare technology assesment organizations, professional societies, advocacy organizations, and industry determined by the dynamics of local situations and the goals of individual programs. Further, IHS-GPAC should promote research that seeks to understand and define cultural differences in stigmatization of people with headache disorders, inform strategies that will successfully mitigate stigma, and, ultimately, lead to improved delivery of care. IHS-GPAC must also recognize that structural stigma towards individuals with headache disorders is often manifest in governmental and institutional policies, and in business practices that codify and formalize discrimination, deny appropriate health care, limit research, and restrict opportunities that lead to fulfilling careers and lives. Accordingly, the IHS-GPAC should identify and support individuals and groups prepared to establish local, regional, and national activist political advocacy organizations working to counter structural stigma towards individuals with headache disorders.
3. Individuals with headache disorders should have access to competent medical care, which involves consultation with a local healthcare provider educated or trained in Headache Medicine who can provide an accurate diagnosis and evidence-based treatment
A shortage of neurologists in general, and of specialists in Headache Medicine in particular, is a serious and growing problem in the United States (32), in Europe (33–36), and in the vast majority of developing nations (37,38), leaving many people with primary headache disorders underdiagnosed and receiving suboptimal care (39,40). A survey done by the European Headache Alliance showed that patients affected by headache in France, Germany, Ireland, Italy, Netherlands, Spain, Sweden, and the United Kingdom commonly encounter delays of several years before being correctly diagnosed, confirming other research (8,9), and many remain dissatisfied with the management of their condition, citing poor response to treatment and the difficulty of accessing and communicating with healthcare professionals as the main reasons (41). In the United States, there are more than 80,000 persons with migraine for each headache specialist, and the number of headache specialists certified by the United Council of Neurologic Subspecialties is inadequate to meet patient demand in the United States (32) – a substantial barrier to care that is projected to worsen through 2025 (42). Among 17 countries in sub-Saharan Africa, for example, there is an estimated average of 0.6 neurologists per million people (38). Migraine and other primary headache disorders are low priority and are under-recognized, and the majority of those with migraine resort to herbal or traditional healers (43).
The global objectives of IHS-GPAC advocacy should be to promote access to adequately trained healthcare providers; early and accurate diagnosis of headache disorders; prescribing of evidence-based acute and preventive treatments; integration of nonpharmacologic therapies (e.g. cognitive, behavioral, and relaxation treatments, as well as complementary, integrative, and traditional medicine); attention to factors, including diet, exercise, and sleep, that influence the health outcomes of various diseases, including headache disorders; and meaningful awareness of patient preferences. Specific recommendations for expanding access to appropriate medical care for people with headache disorders include providing patients and healthcare professionals with more information and education to help them understand the scope of the problem; defining and widely disseminating simple and shared models of care; increasing the availability of specialized headache centers and specialists regardless of geographic, financial, and time barriers to care, particularly through the use of technology (i.e. electronic consultation, secure text messaging, telemedicine) (44); and making awareness and consideration of headache disorders and patients high priority among policymakers (41). Health policy initiatives should be launched and aimed at facilitating integrated service delivery through disease awareness, surveillance, initial and ongoing care, and establishing social support through patient peer-groups that promote health literacy and disease management through mutual learning. In developing nations, it has been suggested that improvements in early headache management at the community level, training and research at the facility level, and healthy lifestyle modification among urban residents may help to reduce the burden of illness and improve productivity in what are often young, thriving populations (45); this may require training social and community health workers, healers, and spiritual leaders, as well as regulating treatments lacking evidence to support their use. While these benchmarks may be aspirational in many parts of the world (even in developed nations with access to specialized care), patient advocates should urge policymakers to adopt and meaningfully work towards achieving them.
4. Training in Headache Medicine should be integrated into all medical school and postgraduate medical education curricula
Headache Medicine electives are rarely offered at medical schools, and academic neurologists with interest in Headache Medicine spend most of their time in clinic – less than 25% of time is spent conducting research or teaching (46). As a result, medical students receive an average of 1 hour of preclinical and 2 hours of clinical teaching in headache. The extent of preparation is nearly the same for neurology residents; they receive an average of 3 hours of didactic instruction in headache (46). Among professionals working in Headache Medicine, only 1.3% were exposed to a headache center during medical school (32). Since the clinical consequences of suboptimal training – low rates of evidence-based medical care (10,11) – can be substantial, it is understandable that a large majority (82.4%) of those currently working in Headache Medicine strongly agree that there needs to be improved headache education for physicians of all specialties (32). Topics about which the majority of neurology residents feel unprepared and want more extensive training than they currently receive include procedural approaches and practice management (47). Given the frequent overlap in symptoms, the ability to differentiate between primary and secondary headaches and implement a specific and cost-effective diagnostic evaluation for relevant secondary headache disorders, some of which are potentially life-threatening, is of paramount importance in training programs. In addition, training is required in the basic communication and interpersonal skills that allow for patient preferences to surface in the decision-making and care-planning process. Healthcare professionals need to learn the skill set that empowers patients to talk about what matters most to them so they can translate that content into information to facilitate shared decision-making.
Sanctioned educational programs should be developed and offered in partnership with accredited providers, and they should be tailored to the needs of medical students as well as those seeking postgraduate and continuing medical education. Migraine programming should also be aimed at primary care providers, including pediatricians and pharmacists, as migraine alone affects up to 10% of all school-aged children and adolescents, and these healthcare professionals frequently interface with young patients and parents (48,49). Educational curricula should encourage integrated service delivery, including the use of traditional medicine (with appropriate regulation of effectiveness and safety), lifestyle modification, and cognitive, behavioral, and mindfulness-based approaches. In cluster headache, educational programs should target general neurologists, primary care physicians, otorhinolaryngologists, and dentists (9). Content for new programming should complement existing programs, such as those presently offered by the International Headache Society and its country affiliate members, leading neurological organizations, academic headache programs, and whenever possible take advantage of ascendant platforms (e.g. online, social media, smart phones) (38).
5. Regional and local partners should work to establish a system for the routine and standardized collection of data pertaining to consultation, diagnosis, and treatment of headache, with emphasis on patient-reported measures of efficacy, disease-specific quality of life, and satisfaction
Patient registries – organized systems using observational methods to collect uniform data (clinical and other) about patients with a particular disease or condition for predetermined scientific, clinical, or policy purposes – produce highly valuable evidence-based outcomes and patient-preference data that offer a range of important benefits, mainly because they involve large, heterogeneous study populations that provide “real world” information. Registries have been shown to improve patient care in a range of disease states, including cystic fibrosis, diabetes, heart disease, and cancer (50–53). For headache disorders, by engaging patients in shaping research agendas and protocols, and linking results with existing databases (e.g. national health insurance and patient health record systems), the resulting analyses can serve as important tools in helping researchers, policymakers, and medical professionals work with patients in the improvement of patient care.
Data for collection by the International Registry for Migraine Research.

Patient registries that generate real-world evidence from a variety of sources, including patient-generated data and electronic health records, can complement traditional evidence generation strategies regarding the usage, potential benefits or risks, as well as the comparative effectiveness of various treatment and management approaches. They can facilitate shared decision-making amongst clinicians and patients – an integral component of patient-centered care. Shared decision-making is the process by which patients and clinicians work collaboratively to develop a care plan that is based on the best available evidence, clinical experience that balances anticipated outcomes and potential risks with the preferences, values, and goals of the patient. Shared decision-making builds trust and can enhance patient compliance, adherence, and outcomes.
Conclusion
By bringing together patients, leaders, and diverse stakeholders, the Global Patient Advocacy Summit galvanized the establishment of a global movement in headache advocacy. The formation of the IHS-GPAC and the pursuit of the expressed goals outlined in this Vancouver Declaration establish benchmarks, and will facilitate awareness and policy development toward improvements in the diagnosis and care for those with headache disorders across the globe.
Clinical implications
The Vancouver Declaration on Global Patient Advocacy establishes the benchmarks, priorities and an advocacy blueprint for the International Headache Society's Global Patient Advocacy Coalition (IHS-GPAC). The IHS-GPAC will promote the global, regional, and local interests of people with headache disorders.
Footnotes
Acknowledgement
The International Headache Society would like to thank the sponsors of the Global Patient Advocacy Summit: Amgen, Eli Lilly, Novartis, Allergan, Teva and electroCore.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DWD has provided consultation, within the past 5 years, to Acorda, Allergan, Amgen, Alder, Promius, eNeura, Eli Lilly & Company, Insys Therapeutics, Autonomic Technologies, Teva, Xenon, Tonix, Trigemina, Boston Scientific, Nocira, Zosano, Biocentric, Biohaven, Magellan, Theranica, Charleston Laboratories, Supernus, Gore and Electrocore. Royalties: Oxford University Press and Cambridge University Press (book royalty); he receives editorial/honoraria from UpToDate, MedNet LLC, Peer View Institute for Medical Education, Medicom, Chameleon Communications, Medscape, WebMD, Academy for Continued Healthcare Learning, Haymarket Medical Education, Global Scientific Communications, HealthLogix, Miller Medical, Academy for Continued Healthcare Learning, MeetingLogiX, Wiley Blackwell, Medicom; stock/options: Nocira, Epien, Healint, Theranica, and Mobile Health; he has a consulting use agreement with NAS and Myndshft; he has a board position at King-Devick Technologies, Inc. and Epien Inc. LE has given lectures and received unrestricted grants from AMGEN/Novartis and TEVA. RJ has given lectures and conducted trials for ATI, Merck, and Allergan, is a Director in LTB and Trustee in IHS. MA discloses he is a consultant, speaker or scientific advisor for Allergan, Amgen, Alder, ATI, Eli Lilly, Novartis, and Teva, primary investigator for Amgen 20120178 (Phase 2), 20120295 (Phase 2), 20130255 (OLE), 20120297 (Phase 3), Alder ALD403-CLIN-001 (Phase 3), Amgen PAC1 20150308 (Phase 2a), and GM-11 gamma-Core-R trials. The other authors have no conflicting interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.