
Abstract
Aim
The aim of this article is to determine vasoactive intestinal peptide (VIP) levels outside migraine attacks in peripheral blood as a potential biomarker for chronic migraine (CM).
Methods
Women older than 17 and diagnosed as CM were recruited. Matched healthy women with no headache history and women with episodic migraine (EM) served as control groups, together with a series of patients with episodic cluster headache in a pain-free period. VIP levels were determined in blood samples obtained from the right antecubital vein by ELISA outside a migraine attack, the patients having taken no symptomatic medication the day before. For ethical reasons, preventives were not stopped.
Results
We assessed plasma samples from 119 women with CM, 33 healthy women, 51 matched women with EM and 18 patients (16 males) with cluster headache matched for age. VIP levels were significantly increased in CM (165.1 pg/ml) as compared to control healthy women (88.5 pg/ml) and episodic cluster headache patients (101.1 pg/ml). VIP levels in EM (134.9 pg/ml) were significantly higher compared to controls and numerically lower than those of CM. Thresholds of 71.8 and 164.5 pg/ml optimized the sensitivity and specificity to differentiate CM from healthy controls and EM, respectively. Variables such as age, CM duration, the presence of aura, analgesic overuse, depression, fibromyalgia, vascular risk factors, history of triptan consumption or kind of preventive treatment did not significantly influence VIP levels.
Conclusion
Increased interictal VIP level measured in peripheral blood could be a biomarker helping in CM diagnosis, though it does not clearly differentiate between EM and CM.
Introduction
Migraine is considered to be a neurovascular disorder. Either changes in the modulating nociceptive inputs from the locus ceruleus and raphe brain stem nuclei (1) or a cortical spreading depression phenomenon (2) are thought to activate the trigemino-vascular system (TVS), which releases vasoactive neuropeptides, mainly calcitonin gene-related peptide (CGRP) and vasoactive intestinal peptide (VIP) around leptomeningeal and extracranial vessels (3,4). Cranial autonomic nervous system has for a long time been implicated in migraine pathophysiology (4,5). VIP is a neurotransmitter, in human cerebral parasympathetic perivascular nerve fibers and the sphenopalatine ganglion, acting as a powerful vasodilator (4,6).
Migraine can be divided into two types: episodic (EM) (fewer than 15 headache days per month) and chronic (CM) (15 or more headache days per month). The International Headache Society (IHS) defines CM as 15 or more headache days per month for at least three months, with ≥8 days per month fulfilling migraine criteria, in the absence of medication overuse (7). Although the source of pain persistence in CM is unknown, it is widely accepted that pain pathways become sensitized by repeated episodes of activation of the two arms, sensory and parasympathetic, of the TVS (8,9). It seems reasonable to speculate that VIP could play a role in migraine chronification by inducing sensitization of cranial perivascular nociceptors.
We determined interictal VIP levels in peripheral blood in a series of women with CM as a potential biomarker for a rather continuous TVS activation, which is thought to be present in CM.
Material and methods
Study participants
Females older than 17 years attending the headache clinic at the University Hospital Central de Asturias who had been diagnosed by us as having CM according to current IHS criteria were included in this study (7). All patients fulfilling criteria for analgesic overuse had been detoxified at least once for a minimum of two months. As control groups, we recruited matched healthy women (medical students, residents, nurses or physicians from our hospital) with no history of headache and taking no medication and females also attending our clinic and meeting IHS diagnostic criteria for EM diagnosis. As an ancillary control group we also studied patients with episodic cluster headache always outside a symptomatic period. All subjects underwent a general physical and neurological examination. Without exception, migraine (chronic or episodic) had at least a normal neuroimaging study (brain magnetic resonance imaging (MRI) in 81 cases and brain computed tomography (CT) with contrast in the remaining 89 cases). All episodic cluster headache cases had a normal brain MRI. Exclusion criteria were pregnant or breast-feeding women, excessive use of alcohol, a history of sinusitis and serious, active psychiatric and somatic diseases, including diabetes. The study was approved by the ethics review board of our center and all the participants gave written consent.
Laboratory determinations
Patients rested in supine position and blood samples were obtained from the right antecubital vein between 9:30 a.m. and noon in a fasting condition. The blood was collected, allowed to clot and serum was separated after centrifugation for 10 minutes at 2000 g. Aliquots were stored at –80 iquots were stored at condition. All samples were obtained interictally, outside a migraine attack the patients having taken no symptomatic medication in the previous 24 hours. For ethical reasons, preventives were not withdrawn.
Serum VIP levels were determined using a commercial enzyme-linked immunosorbent assay (ELISA) kit (USCN Life Science Inc., Hubei, China) strictly following the manufacturer’s instructions. Absorption levels were measured with a spectrophotometer from BioRad. The detection limit of the assay was <2.34 pg/ml.
Statistical analysis
VIP levels and age (years) were described by mean ± standard deviations. Absolute and relative frequencies were used for describing categorical variables. The general Bootstrap algorithm (gBA) and the Exact Chi-square test were used in order to compare, respectively, the VIP levels and the categorical variables of the different groups. The receiver operating characteristic (ROC) curve and the AUC (area under the ROC curve) were obtained to measure the discrimination capacity (CM vs controls and CM vs EM) of the VIP levels. The point associated with the Youden index was chosen as the threshold (TH) point. The confidence band for the ROC curves and 95% confidence intervals (CI) for both the AUC and the TH were computed by 10,000 iterations of the Bootstrap method. Finally, to check the diagnostic capacity of the proposed criteria, the Leave-one-out method was performed. P values below 0.05 were considered statistically different. Both the CI and the statistical tests were not adjusted by multiplicity.
Results
Summary of clinical characteristics of our CM patients.

CM: chronic migraine; SSRIs: selective serotonin uptake inhibitors; ACEIs: angiotensin-converting enzyme inhibitors; NSAIDs: nonsteroidal anti-inflammatory drugs.
VIP levels were significantly higher in women with CM (165.1 ± 125.4 pg/ml; range 20.6–668.2) as compared to control women (88.6 ± 62.3 pg/ml; range 5.1–256.11; p < 0.001) and patients with episodic cluster headache (101.1 ± 78.6, range 28.4–349.9) in an interictal period. VIP levels for EM (134.9 ± 80.4 pg/ml; range 39.8–402.1) were numerically, but not statistically different from those for CM, but were significantly higher (p < 0.01) than those found in control women (Figure 1). Both in the group of healthy controls and in the CM group VIP was not influenced by age in the range of our study.
Vasoactive intestinal peptide (VIP) levels are increased in chronic migraine. Box plot for the VIP levels in controls (Ct, gray), chronic migraine (CM), episodic migraine (EM) and cluster headache (CH). **p < 0.001 vs Ct, #p < 0.01 vs Ct, *p < 0.01 vs CM.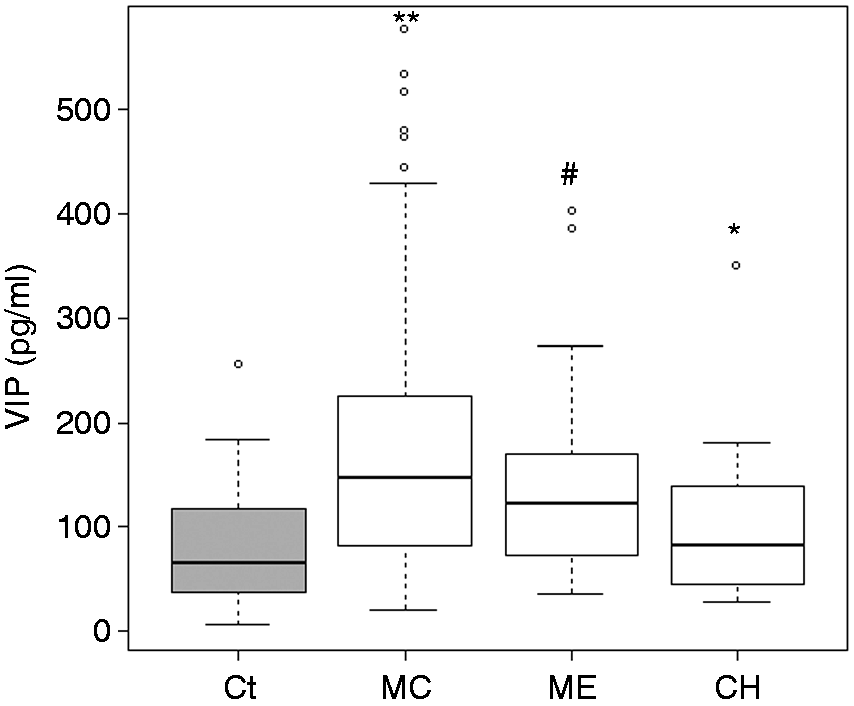
In order to evaluate the VIP concentration as a potential marker for CM, the ROC curve and the AUC were measured. The Youden index was achieved for a VIP concentration of 71.8 pg/ml (95% Bootstrap CI: 50.5–170.5, Figure 2(a)) with an AUC of 0.713 (95% Bootstrap CI: 0.659–0.841). For this TH 79.7% of patients and 61.3% of the controls would be correctly classified. The same discriminatory capacity was obtained by applying the Leave-one-out method. When this methodology was applied to discriminate CM and EM, a VIP concentration of 164.5 pg/ml (95% Bootstrap CI: 71.7–273.2) correctly classified 74.5% of the EM patients and 44.2% of the CM patients (Figure 2(b)).
ROC curve threshold for VIP. (a) Left panel: Kernel density estimations for the VIP levels in CM (continuous line) and controls (dotted line). The vertical line stands for the threshold that achieves the Youden index. In gray, a 95% Bootstrap confidence interval. Right panel: Respective ROC curve with 95% Bootstrap confidence band. Highlighted, the results of the threshold. (b) Similar to (a) for CM (continuous line) and EM (dotted line). ROC: receiver operating characteristics; VIP: vasoactive intestinal peptide; CM: chronic migraine; EM: episodic migraine.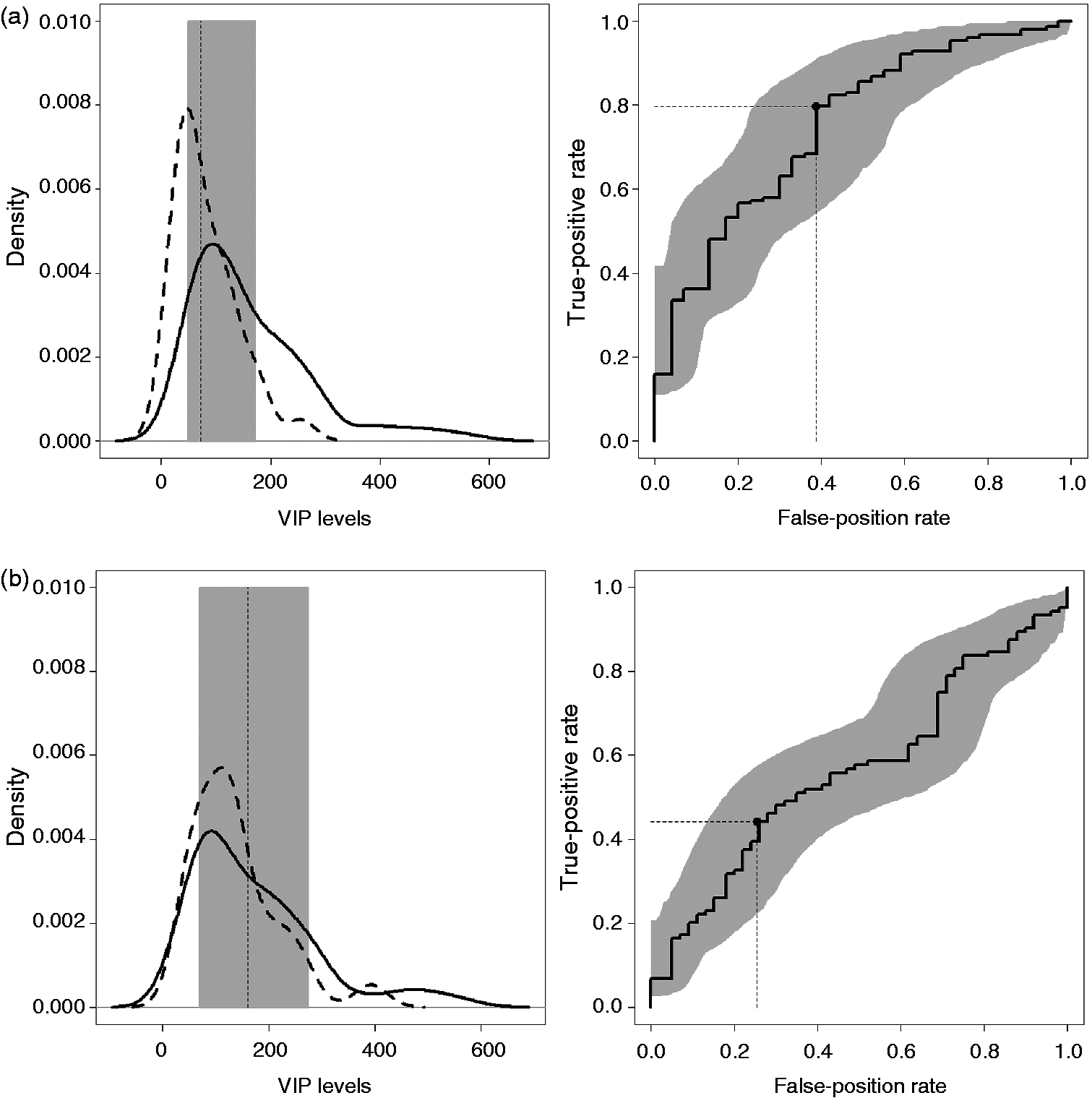
Fifty-six women (47%) with CM had a history of migraine with aura attacks. There were only four women in this group experiencing aura at least once per month in the previous year. Within the sample of women with EM, 26 (54%) also had a history of migraine with aura attacks, though there were just two EM patients who had only attacks of migraine with aura. VIP levels were not different in patients with CM or EM having an aura history (188.4 ± 161.7 and 125.9 ± 63.6) as compared with those without aura (144.4 ± 76.0 and 144.3 ± 95.2). In the group of CM women, VIP levels were not significantly different in patients meeting criteria for analgesic overuse (44 patients, 40.0%) vs those without analgesic overuse (161.4 vs 167.2 pg/ml). VIP levels were not statistically different in patients using triptans as symptomatic medication compared to those who were not taking triptans. VIP levels were not statistically different in patients taking preventives in monotherapy vs politherapy or in those taking topiramate vs those who were not using topiramate. In this group, VIP levels did not change significantly in the presence/absence of a history of depression, fibromyalgia and/or arterial hypertension or depending on CM duration.
Discussion
The main finding of this study was that, compared to healthy women without a history of headache, interictal VIP levels were significantly increased in peripheral blood in a large sample of women with CM. In fact, as an average, VIP levels in CM were double those of healthy controls. To a lesser degree, VIP levels were also significantly elevated in females with EM vs healthy controls. The presence of aura or a variety of clinical comorbidities did not correlate with a change in VIP levels. Concurring with our CGRP results (10), VIP levels were almost identical in CM with and without analgesic overuse.
There are several arguments strongly supporting an involvement of the parasympathetic arm of the TVS in migraine pathophysiology (4,5). Cranial autonomic parasympathetic symptoms, such as lacrimation, rhinorrhea and eyelid edema, do appear, depending on criteria and study design, in 27% to 73% of migraine patients (11–18). Meningeal blood vessels receive dense parasympathetic innervation (3,4,6). Activation and sensitization of nociceptors around extra- and intracranial vessels is a primary source of pain in migraine. It has been proposed that parasympathetic outflow to cephalic vasculature may trigger activation and sensitization of perivascular sensory afferents and thereby migraine pain (19). The parasympathetic innervation of the cerebral circulation, arising from the superior salivary nucleus and passing out of the brain in the facial nerve, represents the most powerful of the neural vasodilator influences on that bed. The parasympathetic system contains and releases a number of transmitter or neuromodulator substances including acetylcholine and several peptides, mainly peptide histidine methionine, pituitary adenylate cyclase-activating polypeptide (PACAP) and VIP, which contribute to regulating cerebrovascular tone and brain hemodynamics. VIP is a 28-amino-acid base polypeptide belonging to a structural superfamily of peptides along with glucagon, secretin and gastrin inhibitory peptide (4,6). It has been clearly established that both the large cerebral and cortical pial vessels have a rich VIPergic innervation (20). Experimental studies have demonstrated that VIP acts as a powerful vasodilator in various species, including humans. In a well-validated model of acute cutaneous pain, intradermal injection of VIP in the forearm increased skin blood flow, wheal and flare more than placebo and even PACAP (21), which strongly supports a role in nociceptive transmission.
Plasma VIP levels have been shown to be increased during cluster headache attacks translating the intense parasympathetic activation (22), but there are very few studies testing VIP levels in migraine, a condition in which up to three-quarters of patients show some symptoms or signs of autonomic parasympathetic activation. Although, in contrast to CGRP, VIP levels were in the range of controls in a series of migraine patients, in the same study plasma VIP levels were elevated in the cranial circulation in the subgroup of migraineurs with pronounced autonomic symptoms (22). VIP levels, also measured in the external jugular vein, were significantly reduced in five migraine patients with autonomic symptoms after successful treatment with rizatriptan in another study (23). Similar findings have been reported in VIP saliva values after sumatriptan in a small group of EM patients (24). There are no data on VIP levels in patients with CM. Our finding of increased peripheral VIP levels in CM patients outside migraine attacks and in the absence of symptomatic medication for at least 24 hours could be interpreted as a distant sign of “permanent” activation of the parasympathetic arm of the TVS. There are at least three possible immediate consequences of these results. First, as happens with CGRP and always carefully considering the clinical data, peripheral VIP levels also seem to be a biomarker for CM, though contrary to CGRP (10), VIP levels were not so consistent and did not clearly differentiate between CM and EM. It seems logical to propose that VIP levels would be increased in those up to three-quarters of patients who express parasympathetic symptoms during migraine attacks. It is even possible that other peptides involved in TVS activation, such as PACAP, could also serve as migraine biomarkers. Second, in theory, peripheral VIP levels could also serve to objectively monitor migraine status and response to preventive treatments, which could be of help, for instance, for a more objective follow-up of patients included in clinical trials. Although we are aware that the fact that, for ethical reasons, most of our patients with migraine were receiving daily preventives could be considered as a limitation of this study, it is also true that this could make our results even more relevant as these drugs should tone down TVS activation. As an example of this, 19 out of the 51 women in this study in a current EM situation had in the past met criteria for CM, which was reversed by preventives. Mean VIP levels in this subset of patients was 143.6 pg/ml, that is, in the range of EM. Third, could these increased VIP levels found in CM patients as a reflection of cranial parasympathetic activation contribute to the development of CM? The role of this peptide in the pathophysiology of individual migraine attacks is controversial as, contrary to CGRP and in spite of being one of the most potent cranial vasodilators, intravenous VIP does not consistently trigger migraine attack, but only a delayed mild headache in some migraineurs (25,26). Other studies, however, have shown that neuromodulating the sphenopalatine ganglion, the main origin of parasympathetic fibers innervating cerebral vessels (6), might be effective in the treatment of migraine attacks and especially in patients with cranial autonomic symptoms (19). We still do not know the exact mechanisms that lead to transformation from EM to CM. It is well established, however, that activation of the TVS system has a crucial role and leads to afferent (CGRP) and efferent (VIP and others) release of neuropeptides. This facilitates leptomeningeal vasodilating and inflammatory responses and induces activation of second-order neurons involved in pain transmission. VIP causes neurogenic inflammation and mast cell degranulation via VIP and PACAP (VPAC) receptor activation (21). Persistent release of VIP could contribute to the appearance of sensitization of central trigeminal neurons (5,8,9,19), which underlies pathophysiology of chronic pain conditions, such as CM. In fact, indirect modulation of central sensory structures, including the trigeminal nucleus caudalis, has been proposed as the mechanism explaining the possible efficacy of sphenopalatine stimulation in the treatment of CM (27). This possible VIP-mediated participation in the transformation from EM to CM is not mutually exclusive, but rather additive, to the more documented role of the CGRP-mediated sensory arm of the TVS system.
Our study has several limitations. First, even though interictal VIP levels in episodic cluster headache out of a symptomatic period were below those of CM, to demonstrate true specificity it would be necessary to test VIP levels in conditions such as stroke, subarachnoid hemorrhage, sinusitis and other trigemino-autonomic cephalalgias in which parasympathetic activation occurs (6). Second, the data shown here come from a headache clinic population with still a limited and selected number of cases. Finally, the real value of VIP levels for monitoring patient status and response to treatment in migraine will be possible only after longitudinal data are available. Taking into account these limitations, interictal VIP levels seem to be a potential biomarker for CM in the context of a patient with long-duration daily or almost daily headaches and a history of migraine, which both could be of help in sharpening a CM diagnosis and supports a role of VIP in the sensitization of pain circuits giving rise to CM.
Clinical implications
Vasoactive intestinal peptide (VIP) levels are increased outside attacks in patients with chronic migraine as a reflection of the activation of the parasympathetic arm of the trigemino-vascular system. Interictal VIP levels seem to be a potential biomarker for chronic migraine (CM) in the context of a patient with long-duration daily or almost daily headaches and a history of migraine. These data support a role of VIP in the sensitization of pain circuits giving rise to CM.
Footnotes
Funding
This work was supported by grant PI11/00889 FISSS (Fondos Feder, ISCIII, Ministry of Education, Spain) and by Allergan Eurasia (Institution Sponsored-Non-Interventional Study MAF/ISS/NS/CM/003). PMC is supported by grant MTM2011-23204 of the Spanish Ministry of Science and Innovation (FEDER support included).
Conflict of interest
None declared.