
Abstract
Background
Orbital myositis is an idiopathic, non-infectious condition, typically seen in young females and usually affecting one extraocular muscle. Orbital myositis mimicking cluster headache is a rare clinical entity, and this is the first description of a case of a secondary trigeminal autonomic cephalalgia from orbital myositis responsive to high-flow oxygen.
Case
A young woman presented with new-onset, oxygen-responsive headache, periorbital pain and autonomic features. She had associated vertical diplopia on downgaze and subtle ocular misalignment. An initial diagnosis of cluster headache was made. Initial brain MRI was unrevealing, but dedicated MRI of the orbits showed enhancement of orbital muscles. The diplopia and the imaging findings were consistent with orbital myositis.
Conclusion
Orbital myositis mimicking cluster headache is rare, and not previously reported as an oxygen-responsive headache.
Introduction
Cluster headache is a typically severe headache disorder that is characterized by unilateral pain associated with prominent ipsilateral autonomic features such as ptosis, pupil changes, lacrimation or rhinorrhea. Similar to other trigeminal autonomic cephalalgias (TACs), cluster headache is most commonly a primary headache disorder (1). However, TACs have also been described in conjunction with lesions that are typically in the posterior cerebral fossa or the sella turcica region. Brain imaging has therefore been recommended in all patients with suspected TACs.
We report a case of a young woman presenting with new-onset oxygen-responsive headache, periorbital pain, restlessness, and autonomic features of an ipsilateral Horner’s syndrome. Unexpectedly, she also had diplopia and ocular misalignment. Initial brain MRI was interpreted as unrevealing, but dedicated MRI of the orbit showed inflammation of orbital muscles. Orbital myositis mimicking cluster headache is a rare clinical entity. We are not aware of orbital myositis being previously described as presenting as an oxygen-responsive headache.
Case
Patient information
A 19-year-old woman presented for assessment of new headaches and double vision. She previously had a history of migraines since about age 16 that typically occurred once monthly, peri-menstrually, and were reliably preceded by scintillating visual aura lasting 5 to 15 minutes. These headaches, with duration of 3 to 5 hours, produced severe bilateral occipital pain, photophobia, phonophobia, nausea and the need to rest or sleep in a dark room. These headaches were historically responsive to non-steroidal anti-inflammatory drugs (NSAIDs). The patient was never on migraine prophylaxis, but she had been started on oral contraception, prescribed by her primary care doctor, in an attempt to help the migraine headaches. One month prior to presentation, the patient decided to stop taking the hormonal contraceptives as she found them ineffective.
While recovering from an upper respiratory infection and an ear infection for which she was taking amoxicillin, the patient developed a headache that was different in character, which was experienced as severe “tearing” right-sided retro-orbital pain that occurred in bouts lasting a couple of hours at a time. The pain was accompanied by restlessness, with the patient rocking back and forth and applying pressure on the eye in an attempt to alleviate it. She had intermittent episodes of pain several times daily for four days without identifiable triggers. These new headaches were associated with a right-sided ptosis, inverse ptosis, lid edema, miosis, rhinorrhea and unilateral photophobia, consistent with a Horner’s syndrome (Figures 1 and 2). They were unrelieved by rest or NSAIDs. In between the bouts of headache, she had persistent right retro-orbital aching and mild ptosis. She also noticed binocular vertical diplopia when looking down.
During attack. After attack.

After 4 days, a neurologist diagnosed cluster headaches and administered high-flow inhaled oxygen at 100%, 12 l/min, which aborted the attacks of acute pain. A brain MRI and orbit without contrast was interpreted as normal. Patient was started on prednisone 40 mg daily. The patient had no recurrence of the severe attacks of headache but continued to have ocular discomfort and diplopia on downgaze and was referred to the Neuro-ophthalmology clinic.
Clinical findings
Afferent visual function was normal, with best corrected visual acuity of 20/15 in both eyes and normal color vision, stereopsis and visual fields. She had a small anisocoria with a smaller right pupil that was equal in light and dark and appeared to be within normal physiologic range; on subsequent exams the pupils were found to be normal. There was a mild right ptosis. Cover testing revealed a flick of right hypertropia, and a subtle right hypertropia on downgaze was elicited with Maddox rod. Forced ductions test was not performed. Ocular pressure was within normal limits in both eyes. Slit lamp exam of the anterior segment was unremarkable. Dilated fundus exam was normal. Of note, the majority of the ictal autonomic signs were no longer present, apart from mild residual ptosis and minor pupillary asymmetry.
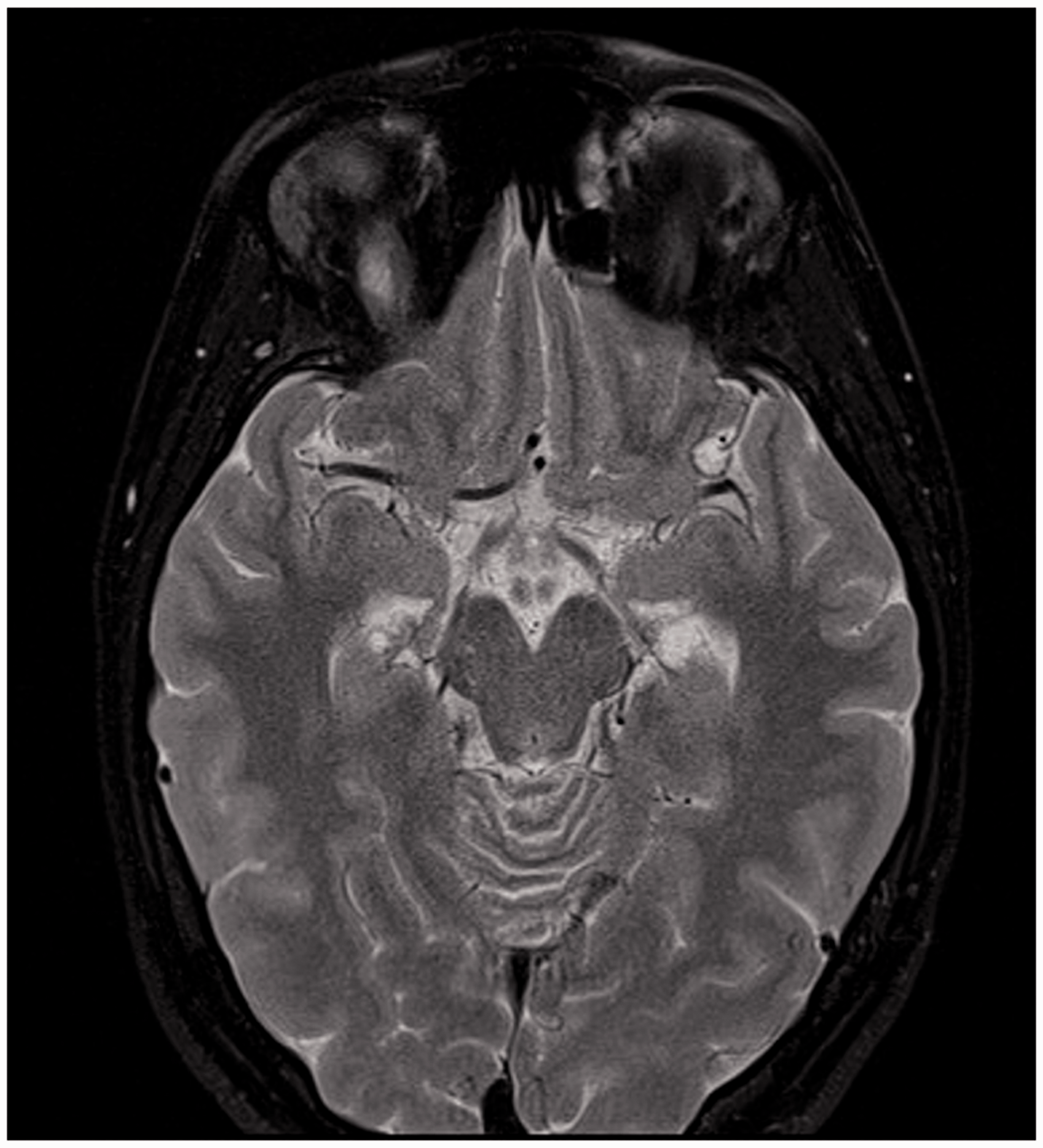
Our independent review of her prior MRI of the brain and orbits was suggestive of increased T2 signal in the right superior rectus muscle (Figure 3). A repeat MRI of the orbits with contrast found enlargement of the right superior rectus muscle and levator palpebrae superioris muscle complex, with abnormal T2 signal and contrast enhancement of both (Figures 4–6). The clinical and new radiological findings led us to diagnose orbital myositis. Her vertical diplopia was considered the result of the enlargement and edema of the superior rectus muscle, causing a restrictive deficit. On prednisone 40 mg daily, the patient reported good symptomatic response. However, due to anxiety she lowered the dose to 20 mg daily, which she took for 1 week, and then 10 mg daily for 1 month at which point she was re-examined. She then received 7.5 mg daily for 2 weeks, 5 mg daily for the next 2 weeks, 2.5 mg daily for the same period and then stopped. Given the rapid and complete response to prednisone, further workup for systemic associations was not performed. She was seen in follow-up at 6, 12 and 16 weeks (last follow-up) and was asymptomatic at each visit. Given the rapid and complete response to oral steroids, no further laboratory workup for systemic associations of orbital myositis was performed. The patient has remained free of recurrence from cluster headache.
MRI T2 coronal. MRI T2 axial. MRI T1 coronal pre-contrast. MRI T1 coronal post-contrast.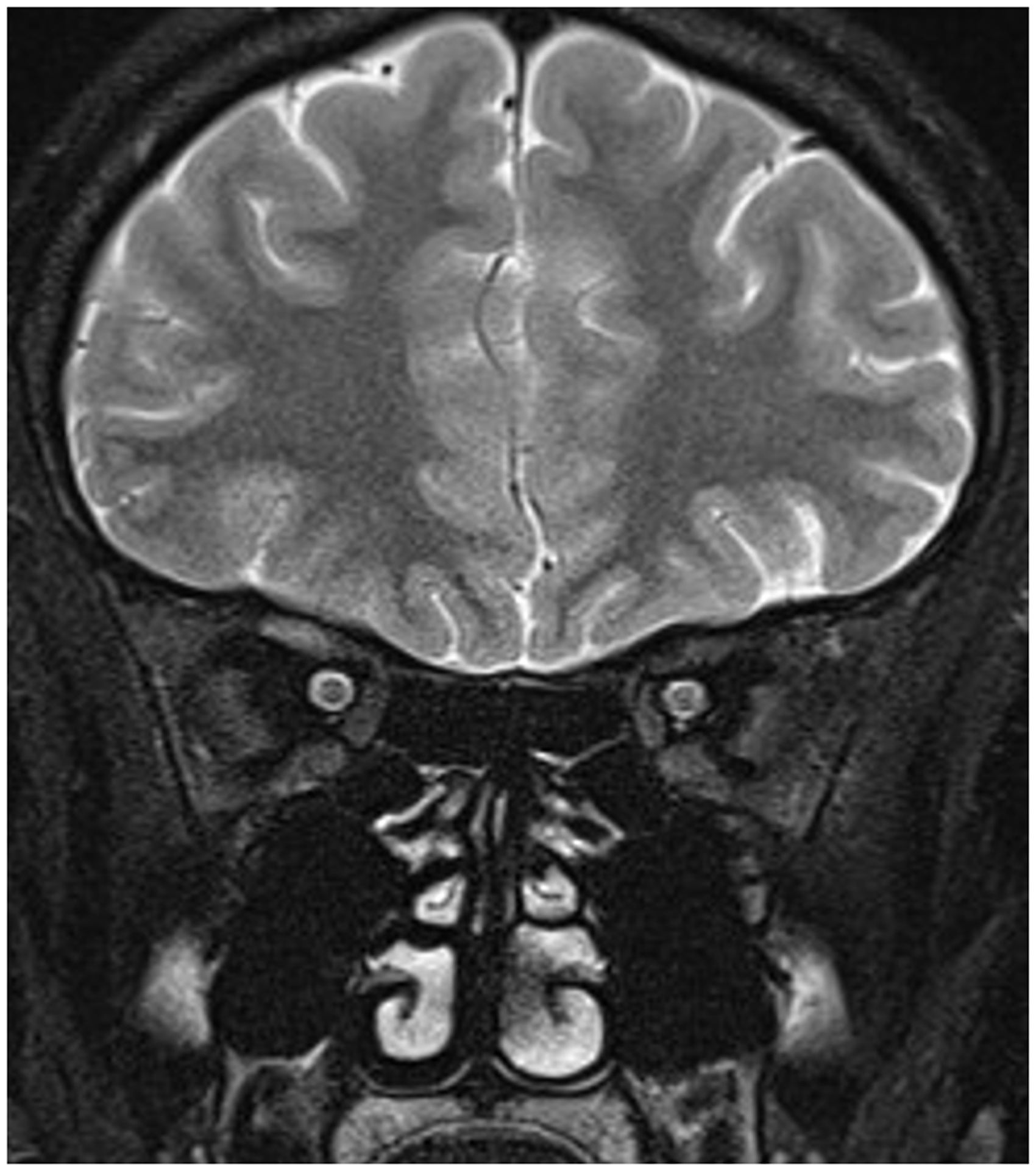


Discussion
Cluster headache, like the other TACs, is characterized by unilateral headache or periorbital pain with ipsilateral autonomic features, including typically conjunctival injection, lacrimation, ipsilateral rhinorrhea or facial sweating (2). Patients are frequently restless and motorically active during attacks of cluster headache, and pain may characteristically resolve with administration of high-flow oxygen.
Orbital myositis that mimics cluster headache has been described only once before (1). The present case, which curiously is from the same practice, has very similar findings to the seminal case, except that the current patient had an oxygen-responsive headache that met International Headache Society criteria of a cluster headache, in that our patient experienced multiple attacks of severe periorbital pain for 4 days, lasting a couple of hours with associated autonomic signs occurring multiple times daily. A positive response to high-flow oxygen supports the diagnosis.
The pathophysiology of the TACs is believed to involve reflex interactions between trigeminal nociceptive afferents and autonomic centers, leading to parasympathetic overactivity, vascular dilation and sympathetic underactivity (3). Hypothalamic circadian centers are thought to generate the characteristic periodicity of attacks. While the majority of TACs are primary headache disorders, brain imaging is recommended in the workup as some cases are associated with intracranial pathology, mostly in the posterior fossa or pituitary/sellar area (4). Lesions have included vascular ones such as aneurysms or arteriovenous malformations as well as benign and malignant neoplasms, most commonly pituitary adenoma. A brain MRI is therefore recommended in the workup, but orbital pathology is not generally considered a trigger.
Interestingly, in the initial report of orbital myositis presenting as cluster headache by Drs Lee and Lessell, imaging demonstrated myositis affecting specifically the ipsilateral superior rectus. We hypothesize that inflammation in the superior rectus muscle, with its proximity to the frontal branch of the trigeminal nerve, triggered a trigeminal-autonomic reflex, which clinically presented as recurrent bouts of cluster headache. Our case supports the original linkage described by Drs. Lee and Lessell of an orbital inciting event becoming a trigger for cluster headache.
In the current case, the clinical and the radiologic signs of an orbital lesion were initially missed. In the diagnostic workup of headache and facial pain, the presence of orbital symptoms and signs such as pain with eye movements or diplopia should direct attention to the orbit, and appropriate imaging should be obtained. We emphasize that diplopia is not an expected symptom of cluster headache, that the persistence of autonomic or orbital signs interictally is a red flag for secondary pathology, and that oxygen responsiveness does not rule out a secondary headache. We hope that greater awareness of atypical features and red flags will facilitate the diagnosis of secondary trigeminal autonomic cephalalgias, and that the identification of other cases of secondary TACs may shed more light on the pathogenesis of these severe headache disorders.
Clinical implications
We report a unique case of orbital myositis mimicking cluster headaches presenting as an oxygen-responsive headache. In the diagnostic workup of headache and facial pain, the presence of orbital symptoms and signs such as pain with eye movements, diplopia or ptosis should direct attention to the orbit, and appropriate imaging should be considered.
Footnotes
Consent
Informed consent was obtained from the patient to utilize her medical records and case for the purpose of this report. All information has been appropriately de-identified.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.