
Abstract
To compare the cervical kinaesthetic sensibility of cervicogenic headache (CEH) patients and asymptomatic controls, the head repositioning accuracy of 10 CEH patients and 23 asymptomatic controls was measured. Should an impaired kinaesthetic sensibility be demonstrated, its assessment could be of diagnostic value in the evaluation of patients with suspected CEH. Additionally, specific exercises to improve cervical kinaesthesia could be prescribed. Kinaesthetic sensibility was assessed using a head repositioning task: subjects were asked to relocate their heads as accurately as possible to a previously memorized head position following an active movement (flexion, extension and left and right rotations). The repositioning error was registered using a validated magnetic tracking device (Flock of Birds). No significant differences were found between the asymptomatic controls and the CEH patients (independent-samples T-test, P < 0.05). We conclude that cervical kinaesthetic sensibility is not impaired in non-traumatic CEH. The use of kinaesthetic assessment and treatment in this patient group seems to be limited.
Introduction
Cervical kinaesthetic sensibility has become increasingly important in the study of neck-related syndromes. Decreased kinaesthetic sensibility has been associated with chronic neck pain, illustrating its potential role in the pathogenesis (1–4). In addition, rehabilitation programmes including kinaesthetic exercises have resulted in an improvement of kinaesthetic sensibility, but also in alleviation of neck complaints (5–7).
Revel et al. were the first to develop a method to assess cervical kinaesthesia (2). Subjects are asked to reposition their heads as accurately as possible following active head movement to a previously memorized head position, being the neutral head position (NHP). The accuracy of the repositioning is measured and the repositioning error is the measure for cervical kinaesthesia. Subjects with decreased cervical kinaesthesia show higher repositioning errors.
Subjects are mostly asked to reposition the head to the NHP, but variants exist such as repositioning to a 30° rotation position (8) or after more complex movements with combinations of side bending and axial rotations (9). Kristjansson et al. have compared the results of asymptomatic controls, patients with insidious neck pain and patients with a whiplash injury on five different variants of the kinaesthetic tests. Only repositioning to the NHP was able to show significant differences between asymptomatic controls and the two patient groups, which makes it the repositioning task of choice (1).
Cervical kinaesthesia has been assessed in different patient samples. In whiplash and neck pain patients, cervical kinaesthesia appears to be impaired (4, 10–12), especially in those subjects with a higher degree of pain and disability (13, 14). In patients with a non-traumatic onset of neck pain, there are indications for a normal kinaesthesia (3, 6).
Dumas et al. have investigated cervical kinaesthesia in patients with cervicogenic headache (CEH) with and without traumatic onset, migraine without aura and asymptomatic controls. No significant differences were found between the four groups (15). Subjects, however, were not asked to relocate their heads to the NHP, but to a 30° starting position as described by Loudon et al. (8). Dumas and colleagues have noted that this measuring method was probably not sensitive enough to detect differences between groups. This was documented later by Kristjansson et al. (1). Dumas et al. also used the Cervical Range of Motion Device (CROM; Professional Medical Technologies, McCallen, TX, USA), which is designed to measure neck mobility. The result is registered with a goniometer using a scale interval of 2°. This interval is probably too large to measure the differences in kinaesthesia, which are reported to be around 3–4° (1, 2, 10, 14).
Zito et al. have found no significant differences between CEH patients and asymptomatic controls. The authors, however, studied a very young sample (mean age 25.3 years), whereas CEH sufferers have a mean age of 42.9 years (16).
This study aimed to measure the head repositioning accuracy (HRA) using a electromagnetic tracking device in adults with CEH and to compare this result with that of a group of asymptomatic volunteers.
Methods
Subjects
Subjects with a combination of headache and neck pain were recruited in out-patient physiotherapy offices and at a university hospital (UZ Brussels). All participants were at least 18 years old. People with a history of major neck trauma were excluded from the study, as were subjects who had undergone cervical spine surgery, suffered from disabling dizziness or had reported a known underlying pathology (osteoarthritis, neurological disorder). Additional in-/exclusion criteria were set to include either patients or controls: patients were included if they had a history of neck pain and headache of at least 3 months and a headache frequency of at least twice a month. A standardized questionnaire, developed to screen for CEH according to the Sjaastad criteria, was used for further patient selection (17–19).
CEH diagnosis was carried out by one examiner (W.D.H.) and was conferred on with a CEH expert (H.v.S.). The criteria proposed by Sjaastad et al. were scrupulously followed to obtain a homogeneous sample of CEH patients (19) (Table 1). Only those subjects who fulfilled the criteria were retained for further analysis. Diagnostic blocks were not performed. Patients with more than one headache type or a bilateral headache were excluded.
Major criteria of CEH diagnosis according to Sjaastad et al. (19)

Asymptomatic controls were excluded in case of headache, neck or arm complaints (pain and/or stiffness) at the time of the study or in the previous 2 years.
Measuring cervical kinaesthesia
The Revel et al. method (2) was used to test cervical kinaesthesia, whereby subjects have to relocate their heads as accurately as possible to a self-determined NHP.
The repositioning error was measured using a electromagnetic tracking device (Flock of Birds; Ascension Technology Corporation, Burlington, VT, USA). The Flock of Birds consists of a transmitter generating a pulsed DC magnetic field. In this generated field, the orientation and position of multiple sensors can be registered. We used a configuration with two sensors.
Subjects were seated with a backrest. They were blindfolded with their hands resting on their lap. Test equipment consisted of an adjustable head fixation belt designed for the attachment of surgical lights (Heine MD 350 F. O.). On this fixation belt, a laser pointer was attached, as well as one sensor of the magnetic tracker. This sensor captured differences in head orientation and position compared with the initial position (program Winbird). The transmitter of the magnetic system was placed behind the subject and the second sensor was used as a fixed reference sensor (Fig. 1)

Starting position and test configuration of the cervical kinaesthetic test. The transmitter of the magnetic system generating a magnetic field is placed behind the subject. In this magnetic field the orientation and position of the two sensors is registered. An adjustable head fixation belt is used for the fixation of a laser pointer and sensor 1. Sensor 2 was used as a fixed reference sensor.
The total weight of the fixation belt and laser pointer was 245 g. The laser pointer projected a spot on the wall.
Subjects were asked to find a NHP and to memorize it. This NHP was marked on a target sheet fixed on the wall by the examiner. This starting position was registered by the Flock of Birds software. Consequently, the subjects performed the repositioning task: after, respectively, right rotation (RR), left rotation (LR), flexion (Flex) and extension (Ext), they were asked to relocate their heads as accurately as possible to their NHP. When they assumed they had reached their NHP, they clearly said ‘yes’, and this position was again registered by the Flock of Birds software. For each movement 10 repetitions were made and an average of these 10 repetitions was calculated.
The validity of the experimental set-up was checked by means of a wooden phantom containing a rotating disc with Flock of Birds sensor, allowing for the verification of registered position differences. Rotations in two perpendicular planes, mimicking flexion and extension, and left and right axial rotation as used in the experimental set-up, respectively, were repeatedly registered (n = 30 for every movement). Compared with a known distance of 14.20 cm, the registered position differences remained inferior to 0.15 cm. Intra- and interobserver reliability of the head repositioning error registered with the present Flock of Birds configuration was subsequently checked on 12 additional healthy subjects by three observers. The best interobserver reliability was found in head repositioning returning from extension and from right axial rotation [intraclass correlation coefficients (ICCs) ranging from 0.91 to 0.97]. Definite lower interobserver reliability was found in repositioning following flexion (ICCs −0.02 to 0.66) and left rotation (ICCs 0.43–0.77), representing, respectively, the first repositioning task in two repositioning sequences. Intraobserver reliability was good to excellent for head repositioning returning from extension, left and right axial rotation (ICCs ranging from 0.75 to 0.97) and moderate to excellent for repositioning after flexion (ICCs ranging from 0.61 to 0.95).
Data analysis
Data were analysed using SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, USA). Normality of data was checked using the one-sample Kolmogorov–Smirnoff test. For normal distributed variables the T-test for independent samples was used. A significance level of P < 0.05 was used.
The study protocol was approved by the ethics committee of the University Hopsital (UZ Brussel) of the Vrije Universiteit Brussel.
Results
After screening for eligibility, 44 headache patients and 23 asymptomatic controls entered the study. From the 44 headache patients, 10 patients fulfilled the CEH criteria (19) and were selected for further analysis.
The distribution of all variables was normal, so the independent samples T-test was used for further analysis.
In Table 2 demographic data and general headache characteristics are presented.
Demographic data and general headache characteristics

No significant difference was found between the age of the patients and controls (P = 0.181, independent samples T-test).
CEH, Cervicogenic headache; VAS, visual analogue scale.
Table 3 provides additional information about the presence of the CEH criteria in our sample.
Overview of the scoring of patients on the major CEH criteria
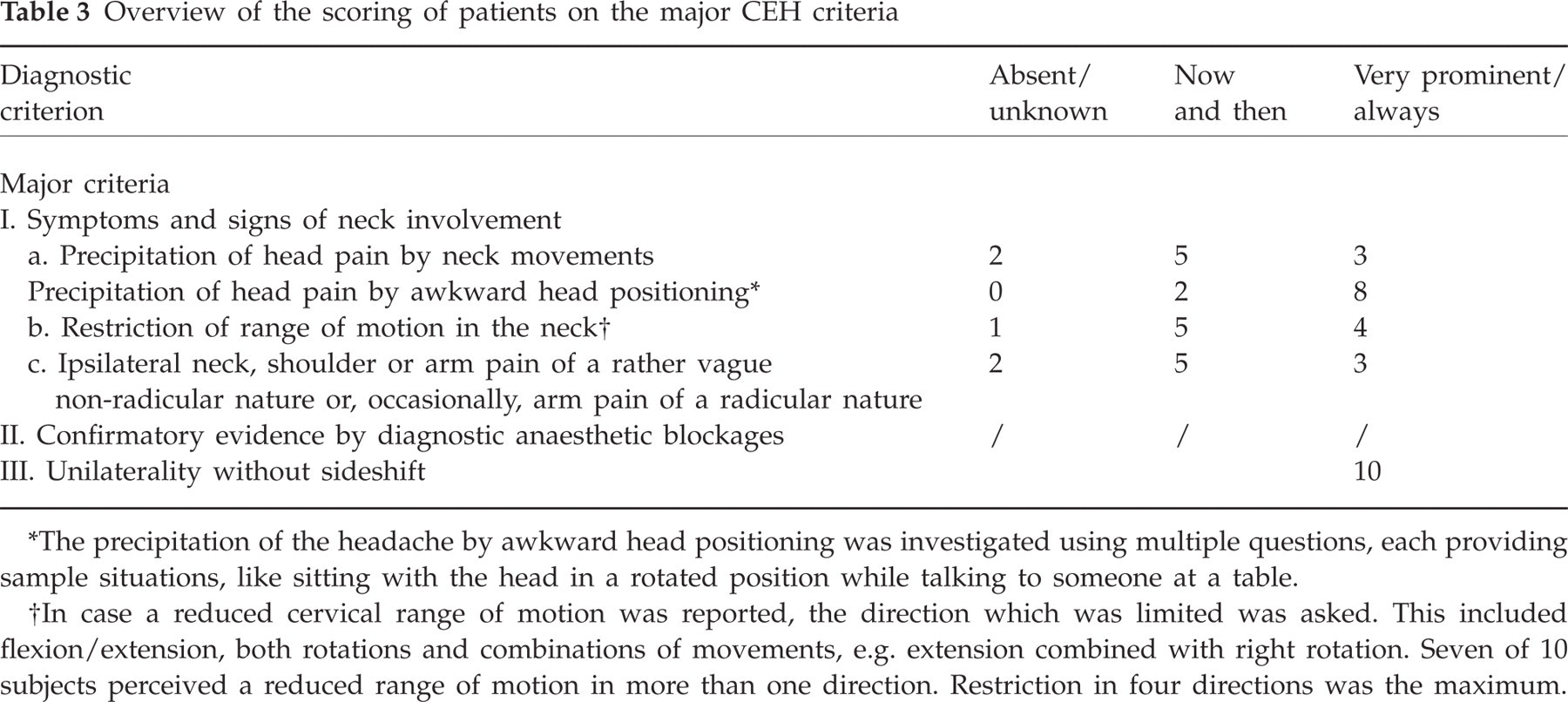
The precipitation of the headache by awkward head positioning was investigated using multiple questions, each providing sample situations, like sitting with the head in a rotated position while talking to someone at a table.
In case a reduced cervical range of motion was reported, the direction which was limited was asked. This included flexion/extension, both rotations and combinations of movements, e.g. extension combined with right rotation. Seven of 10 subjects perceived a reduced range of motion in more than one direction. Restriction in four directions was the maximum.
No significant differences were found between the two groups for the HRA variables (Table 4).
Repositioning error of the cervicogenic headache group (CEH) and of the asymptomatic controls

For each movement the mean and standard deviation are presented. P, significance level (independent samples T-test).
Discussion
Cervical kinaesthetic sensibility was investigated in CEH patients and compared with that of asymptomatic controls. The repositioning error, which is a measure of kinaesthetic sensibility, was registered using a validated electromagnetic tracking device. We were unable to detect significant differences between the patient group and our group of asymptomatic controls, which indicates that kinaesthetic function is not impaired in non-traumatic CEH patients.
Our findings are in line with those reported in the literature. Two studies have reported on cervical kinaesthetic sensibility in non-traumatic CEH (15, 20), and neither found an impaired kinaesthetic function. Two major differences are the type of repositioning task and the method of registering the repositioning error as used by Dumas et al. (15), and the age distribution of the group studied by Zito et al. (20) We used the Revel method (repositioning to the NHP), registered the repositioning error with high-tech equipment and studied a sample of CEH patients with a realistic age distribution.
Even then it was not possible to demonstrate an impaired cervical kinaesthetic sensibility in non-traumatic CEH. A very recent study documenting cervical musculoskeletal impairments, including cervical kinaesthesia, has also been unable to detect differences between CEH patients and patients with migraine or tension-type headache and asymptomatic controls (21, 22).
It is important to note that similar findings have been reported in other categories of cervical spine pain patient. Impairments in cervical kinaesthetic sensibility have been found in patients with post-traumatic neck complaints (10, 12). They were even more pronounced in patients who, in addition, reported dizziness (23, 24). In patients with non-traumatic neck pain or even in patients with mild whiplash-associated disorders, however, these impairments were less frequently reported (3, 14, 25).
These findings and the corresponding literature have two implications for patient assessment. First, we believe that scientific arguments are currently lacking to assess cervical kinaesthetic sensibility in patients with suspected CEH. Second, CEH patients with and without a history of neck trauma should be analysed separately, because a potentially impaired kinaesthetic function is probably a consequence of the neck trauma, and is not related to the headache.
Our findings also have therapeutic implications, as they indicate that the use of proprioceptive exercises in patients with non-traumatic CEH may be limited.
A diagnostic headache questionnaire (17, 18) was used to screen for CEH characteristics. The value of diagnostic questionnaires in comparison with a clinical interview has been studied (26). Questionnaires have their limitations, as they lack the flexibility of a clinical interview. Questions cannot be repeated or reformulated when a patient does not fully understand them. However, the phrasing of a questionnaire is more standardized. Rasmussen et al. have also mentioned methodological pitfalls, particularly the internal consistency and test–retest repeatability. Reliability scores of our questionnaire are very high (κ 0.982, sign. <0.001), as is internal consistency (Cronbach α 0.87) (17). With regard to validation, a CEH expert's advice was sought. Taking this into considering we believe that the use of this questionnaire is justified.
Patients with CEH were selected by two examiners, who after careful consideration retained only those subjects who met the CEH criteria (19). Subjects with combinations of different headache types were excluded. This resulted in the selection of a small but homogeneous sample of CEH patients.
In conclusion, our findings support the evidence of unimpaired kinaesthetic sensibility. As no impairment was documented using various measuring methods in different age groups, such impairment is unlikely in non-traumatic CEH. Further studies with larger patient samples are required to further clarify and determine the role of kinaesthetic assessment and training in CEH patients.
Footnotes
Acknowledgements
The authors thank Sandy Kesler and Muriel Goossens for their help in collecting the data and conducting the pilot study.