
Abstract
Objective
To describe treatment patterns of migraine patients in the Japan Medical Data Center (JMDC) database.
Methods
Patients aged ≥18 years with ≥1 inpatient or ≥2 outpatient migraine diagnoses, ≥1 outpatient diagnosis and ≥1 migraine-specific acute treatment (triptan or ergotamine), or ≥2 migraine-specific acute treatments from 1 May 2011 to 30 April 2014 were identified. Patients were required to be enrolled in a health plan for ≥1 year before and after the index date. The first migraine diagnosis or acute treatment defined the index date. Patients were stratified by the migraine treatments observed after the index date (i.e. migraine-specific acute treatment only [AT], prophylactic with or without migraine-specific acute treatment [PT], or no treatment [NT]) and described regarding the first migraine treatment regimen and subsequent treatment patterns during up to 1 year of follow-up.
Results
A total of 16,443 patients met the eligibility criteria (9873 AT, 3022 PT, and 3548 NT). AT patients had mean (SD) 10.3 (20.5) acute treatment days during 1-year follow-up, and 81.9% received triptans. When assessing the first migraine treatment regimen during follow-up in PT patients, 29.2% received prophylactic treatment only and 51.7% received both acute and prophylactic treatment. Calcium-channel blockers with or without concomitant triptans (34.4%) were the most common first regimen. Approximately 62.2% discontinued initial prophylactic treatment after an average of 61.2 days (SD = 65.3) of persistent treatment. Among discontinuers, 15.2% reinitiated original treatment and 7.0% switched treatment post-discontinuation within a year, while the remaining patients did not receive prophylactic therapy following discontinuation.
Conclusions
Among Japanese migraine patients, prophylactic use was low and associated with a high rate of discontinuation following a brief treatment period. Many patients reinitiated or switched treatment following discontinuation, while a significant proportion of patients remained discontinued from prophylactic therapy, suggesting a high unmet need.
Introduction
Migraine is a neurological disease characterized by disabling headache, which negatively affects patients’ quality of life and function status (1–4). Findings from the Global Burden of Disease Study 2010 showed that migraine was the third most prevalent and seventh most disabling medical disorder globally (5). However, studies evaluating the epidemiological burden of migraine in Japan are limited. Prevalence of migraine in Japan was reported to be 8.4% in a nationwide survey conducted in 1997 (6). Another study estimated migraine prevalence of 6.0% in Daisen, a rural community in western Japan (7).
Episodic migraine is often defined among patients experiencing 0–14 headache days per month, while chronic migraine is typically defined as headache affecting the patient for 15 or more days per month (2,8). The Japan Headache Society updated the treatment guidelines in 2013 for the management of chronic migraine. According to these guidelines, calcium-channel blockers (lomerizine – most widely used as it is a flunarizine analogue, verapamil), an antiepileptic drug (valproate), a beta blocker (propranolol), and an antidepressant (amitriptyline) are currently approved under insurance coverage as treatment options for patients with chronic migraine as well as for patients with high-frequent or disabling episodic migraine (9). Many more migraine prophylactic therapies are available in the United States (US) for the treatment of chronic and episodic migraine, including beta blockers (metoprolol, propranolol, timolol, atenolol, and nadolol), antiepileptic drugs (topiramate, sodium valproate, and divalproex sodium), triptans (frovatriptan, naratriptan, and zolmitriptan), and antidepressants (amitriptyline and venlafaxine). Additional medications within the classes of beta blockers, calcium-channel blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, antihistamines, and antithrombotic agents are also considered to be possibly effective in prevention of migraine episodes (10–12). Acute treatments for migraine in the US include combination NSAIDS/acetaminophen/aspirin/caffeine; ergotamines; triptans; and opiates.
As limited data exist, information from a real-world migraine population in Japan on epidemiology and current treatment practices is needed. This study sought to describe the epidemiology of migraine and characterize adult migraine patients using the Japan Medical Data Center (JMDC) database. The study also reported on treatment patterns, including therapies received (i.e. prophylactic medications and acute medications) and treatment duration, discontinuation, switches, and augmentations.
Methods
Data source
All Japanese residents are required to have health insurance coverage, with coverage offered through both employee-based and community-based insurers, and fee schedules for medical services set by the government (13). Furthermore, in Japan, services are provided by either public or private hospitals and clinics, with hospitals required by law to be run as nonprofit and managed by physicians and clinics required to be owned and operated by physicians. This study used data from the JMDC database. The JMDC database comprises retrospective claims data from primarily working age persons and their family members in Japan enrolled in one of several insurance programs, including public and private payers. The data include more than 1 million unique persons from 2003 onward and represent approximately 1% of the population of Japan. Data elements in the database include patient-level demographic and plan enrollment information, inpatient and outpatient medical claims, and pharmacy claims. This study used the most recent 5 calendar years of data available at the time this study was conducted (i.e. 1 May 2010 to 30 April 2015). As data were de-identified and retrospective, RTI International’s institutional review board determined that this study was not research with human subjects.
Study population
This study aimed to capture a broad population of patients with migraine including both treated and diagnosed patients. Therefore, patients were identified if they met any of the following criteria between 1 May 2011 and 30 April 2014: (a) One inpatient or two outpatient diagnoses (at least 7 days apart) of migraine based on International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) code G43.xx; (b) one outpatient diagnosis of migraine and one prescription claim for either triptan or ergotamine; or (c) two prescription claims for either triptan or ergotamine. The date of the first observed migraine diagnosis or prescription claim for triptan/ergotamine (if no migraine diagnosis was present) defined the index diagnosis date.
Patients were further required to be aged at least 18 years on their index diagnosis date, enrolled in the health plan for a minimum of 12 months before the index diagnosis date (i.e. the baseline period, to allow for assessment of comorbidities and confirmation of newly observed migraine diagnosis) and 12 months after this date (i.e. the follow-up period), and to have not had diagnoses of epilepsy or seizure during the baseline and follow-up periods (ICD-10-CM codes G40.xx, G41.xx, G56.xx, F44.5x).
Study cohorts
Summary of prophylactic and acute migraine treatments.

Study measures
Study measures included migraine incidence and prevalence, demographic and clinical characteristics, and treatment patterns.
As incidence refers to the number of new cases during a period of time, patients were required to have 12 months of continuous health plan enrollment before the index diagnosis date with no migraine diagnosis or acute treatment (i.e. triptan or ergotamine) during this time. As prevalence refers to the number of cases during a time period, no minimum period of continuous health plan enrollment before the index diagnosis date was required.
The denominator for the incidence and prevalence calculation was based on all persons aged >18 years in the JMDC database. From this population, patients with at least 1 month of enrollment between 1 January 2010 to 31 December 2014 were selected for inclusion in the denominator. To calculate migraine incidence, person-time (i.e. person-years) was the denominator. For patients with migraine, the period started on the enrollment date and ended on the date of the first migraine diagnosis. For patients without migraine, the period started on the enrollment date and ended on the minimum of either (1) date of disenrollment from the health plan or (2) the end of the database.
Demographics measured at the index diagnosis date included age and sex. The Charlson Comorbidity Index (CCI) score was calculated to obtain patients’ overall comorbidity burden during the baseline period. The CCI score includes 20 categories of conditions, defined by ICD-10-CM codes, with weights corresponding to the severity of the condition, and a higher CCI score indicating a patient having a higher baseline disease burden (14). The presence of other comorbidities (i.e. depression and anxiety) during the baseline period were also reported. Additionally, the presence of migraine medications (at the class level) were also reported during the baseline period.
Among patients receiving acute treatment only during the follow-up period, the following treatment pattern measures were reported: Type of first observed acute treatment class, acute treatment history, acute and prophylactic treatments received during the baseline period, time from index diagnosis date to treatment initiation (in days, among patients initiating treatment after the index diagnosis date), types of acute treatments received during follow-up, days supplied for the first observed acute treatment, and days supplied for any acute treatment.
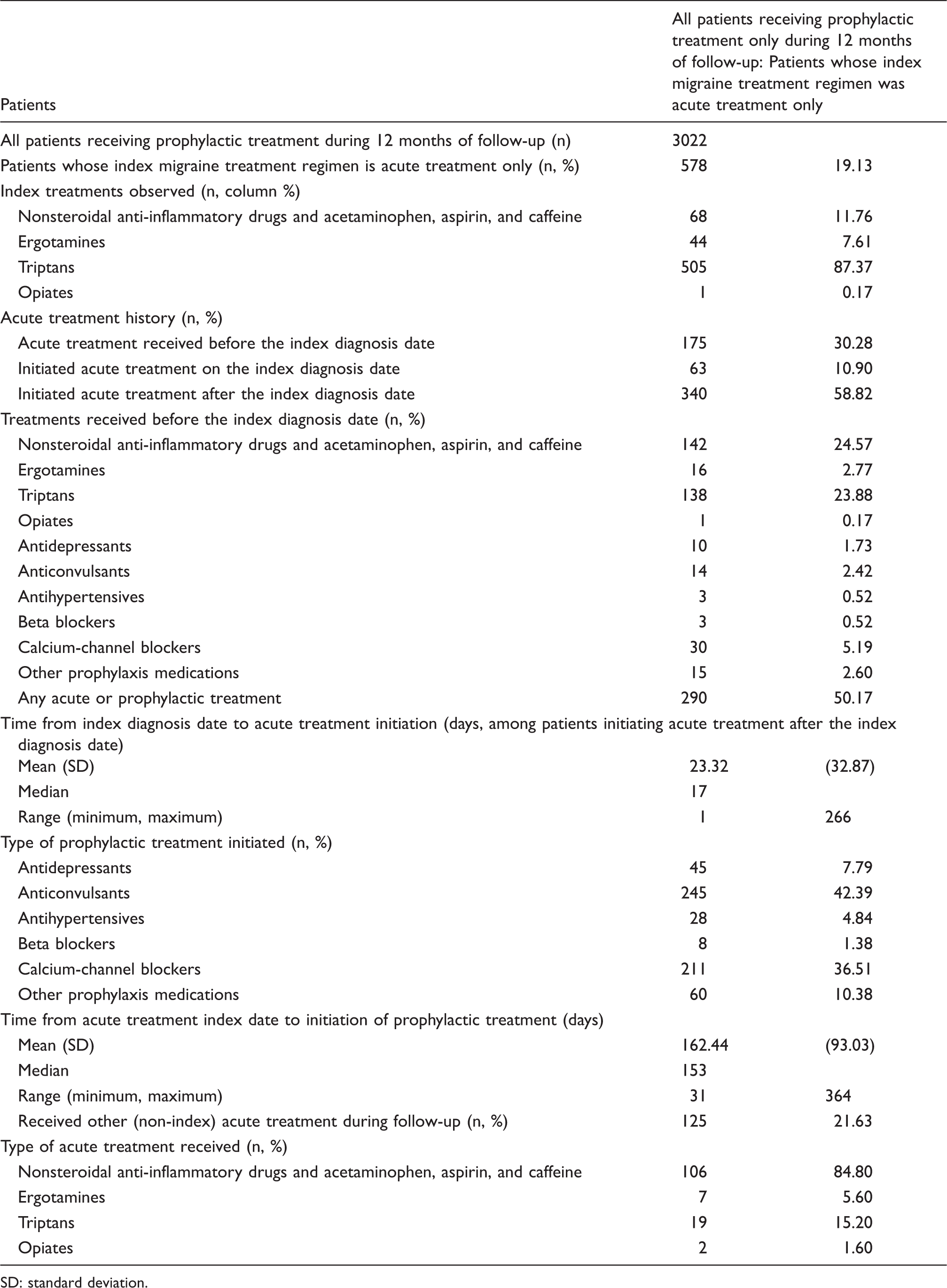
Among patients receiving prophylactic treatment during the follow-up period, treatment patterns were reported based on the index migraine treatment regimen, including acute treatment only (i.e. patients starting acute treatment and subsequently adding prophylactic treatment), prophylactic treatment only, and both acute and prophylactic treatment. For patients receiving acute treatment only as their index migraine treatment regimen, the following treatment pattern measures were reported: Type of acute treatment received as the index migraine treatment regimen, acute treatment history, types of acute and prophylactic treatments received before the index diagnosis date, time from index diagnosis date to initiation of acute treatment (in days, among patients initiating acute treatment after the index diagnosis date), type of prophylactic treatment initiated, time from index diagnosis date to initiation of prophylactic treatment, and receipt of other acute treatments during follow-up.
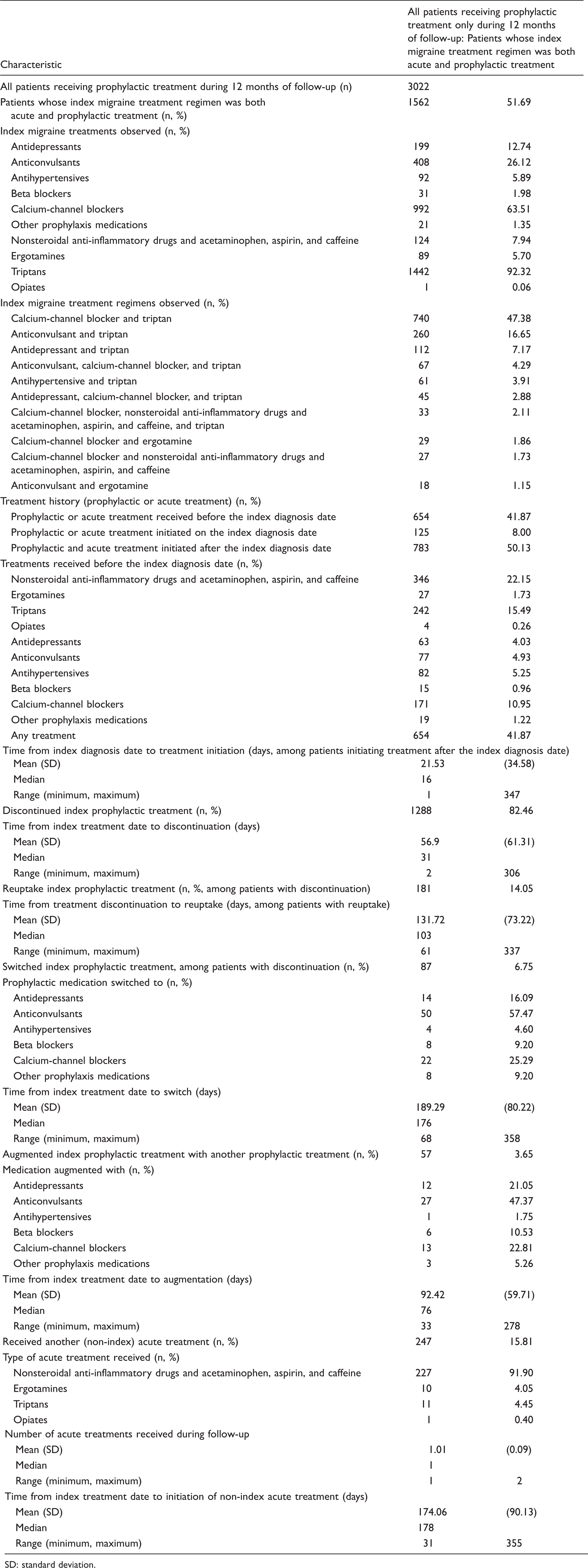
For patients who received prophylactic treatment as their index migraine treatment regimen (i.e. index migraine treatment regimens composed of either prophylactic treatment only or prophylactic and acute treatment), the following treatment pattern measures were reported: Type of prophylactic treatment classes in the index migraine treatment regimen, treatment history, time from index diagnosis date to treatment initiation (in days, among patients initiating treatment after the index diagnosis date), types of acute and prophylactic treatments received before the index diagnosis date, discontinuation of any prophylactic treatment in the index migraine treatment regimen, time from index diagnosis date to discontinuation (in days, among patients discontinuing the prophylactic portion of their index migraine treatment regimen), reuptake of the prophylactic portion of their index migraine treatment regimen after discontinuation, time from discontinuation of the prophylactic portion of their index migraine treatment regimen to reuptake (in days, among patients with reuptake), switching prophylactic treatment, type of prophylactic medication switched to, time from index treatment date to treatment switch (in days, among patients switching prophylactic treatment), augmentation of index migraine treatment regimen with another prophylactic treatment, type of prophylactic medication augmented with (among patients with augmentation), and time from index treatment date to treatment augmentation (in days, among patients augmenting prophylactic treatment). Among patients whose index migraine treatment regimen was prophylactic treatment only, subsequent use of acute treatment, including types of acute treatments received and time from index treatment date to acute treatment initiation, was reported. Among patients whose index migraine treatment regimen was both acute and prophylactic treatment, the type of acute treatment received as part of the index migraine treatment regimen was reported, along with any subsequent acute medications received that were not part of the index migraine treatment regimen.
Prophylactic treatment discontinuation was defined as ending treatment with the prophylactic portion of the index migraine treatment regimen without evidence of another refill for the same medication within 60 days of exhausting the drug supply for the prior prescription. Prophylactic medication reuptake was identified when the patient reinitiated the prophylactic portion of the index migraine treatment regimen after discontinuation. Prophylactic treatment switching was assessed among patients discontinuing treatment and was identified when patients filled a prescription for another prophylactic medication (either in the same class or a different medication class) following the 60 days after exhaustion of the drug supply for the prophylactic portion of the index migraine treatment regimen. Medication augmentation was defined as the subsequent uptake of an additional prophylactic migraine medication (either in the same class or a different medication class) to the index migraine treatment regimen within the 60 days after exhaustion of the drug supply for the prior prophylactic medication.
Data analysis
Study measures were analyzed through descriptive statistics. All analyses were conducted using SAS (version 9.3).
Results
Migraine incidence and prevalence in the JMDC population
Of the 2,289,915 patients in the JMDC database, 16,479 incident migraine cases were identified in 6,446,991 person-years of follow-up, resulting in an incidence of 2.56 per 1000 patient-years. A total of 32,702 patients (1.43% of the JMDC population) were identified as having a migraine diagnosis.
Sample selection
Between 1 May 2011 and 30 April 2014, 47,295 patients with a diagnosis of migraine or at least one prescription for triptan or ergotamine were identified, and 16,443 patients met all study inclusion criteria and were included in the final study sample (Figure 1). Most patients (63.6%) received acute treatment only as their index migraine treatment regimen and 14.9% of patients received prophylactic treatment as their index migraine treatment regimen, while 21.6% of patients had no prescription claims indicating treatment was received during follow-up. Among patients receiving prophylactic treatment as their index migraine treatment regimen, 36.1% received prophylactic treatment only, while 63.9% received both acute and prophylactic treatment.
Sample selection flow chart.
Patient demographic and clinical characteristics
Patient demographics and baseline clinical characteristics.

AIDS: acquired immunodeficiency syndrome; CCI: Charlson Comorbidity Index; HIV: human immunodeficiency virus; SD: standard deviation.
Measured during the 12-month period before the index diagnosis date.
CCI comorbidities occurring in less than 1% of the overall population not shown (i.e. cellulitis, dementia, HIV/AIDS, paraplegia/hemiplegia, metastatic carcinoma, diabetes with chronic complications, moderate to severe liver disease, metastatic carcinoma, myocardial infarction, peripheral artery disease).
Patient age was highest for patients with prophylactic treatment only as their index migraine treatment regimen and lowest for patients with acute treatment only as their index migraine treatment regimen, with patients with no treatment in the middle. Patients with prophylactic treatment only as their index migraine treatment regimen had a higher CCI score compared with patients with acute treatment only and patients with both acute and prophylactic treatment as their index migraine treatment regimen, and compared with patients with no treatment during follow-up. Among patients receiving acute treatment only as their index migraine treatment regimen, the percentage of patients receiving any prophylactic treatment during the baseline period was low (3.2%), while among patients with any prophylactic treatment as their index migraine treatment regimen, 30.6% also received prophylactic treatment during baseline. Use of acute treatments during the baseline period was similar for patients with acute treatment only as their index migraine treatment regimen and for patients with any prophylactic treatment as their index migraine treatment regimen.
Treatment patterns
Patients receiving acute treatment only during 12-month follow-up
Treatment patterns among patients receiving acute treatment only during 12 months of follow-up.

SD: standard deviation.
Patients receiving any prophylactic treatment during 12-month follow-up
Patients whose index migraine treatment regimen is acute treatment only
Treatment patterns among patients receiving prophylactic treatment during 12 months of follow-up: Patients whose index migraine treatment regimen was acute treatment only.
SD: standard deviation.
Patients whose index migraine treatment regimen is prophylactic treatment only
Treatment patterns among patients receiving prophylactic treatment during 12 months of follow-up: Patients whose index migraine treatment regimen was prophylactic treatment only.

SD: standard deviation.
Patients whose index migraine treatment regimen is both acute and prophylactic treatment
Treatment patterns among patients receiving prophylactic treatment during 12 months of follow-up: Patients whose index migraine treatment regimen was both acute and prophylactic treatment.
SD: standard deviation.
Discussion
This retrospective database analysis examined Japanese patients with migraine and reported on epidemiology, demographic and clinical characteristics, and treatment patterns. The incidence of migraine in the JMDC population was observed to be 2.6 per 1000 patient-years, while the prevalence was 1.4%. Previous studies estimated the prevalence of migraine in Japan is between 6.0% and 8.4% (6,7), much higher than the 1.4% observed in this analysis. However, our study required either two diagnoses of migraine or a single migraine diagnosis plus a prescription for triptan or ergotamine. If one migraine diagnosis or triptan/ergotamine prescription had been required, a slightly higher prevalence (i.e. 2.1%) was observed. Our results may be lower than those reported elsewhere as only patients seeking medical advice for migraines (representing the most severe migraine population) were included. Sakai and Igarashi (6) observed 69.4% of patients with migraine never consulted a physician for headache and only 11.6% of patients were aware that their headache was migraine. This would partially explain the lower prevalence of migraine in the JMDC population, as all patients included in our study were required to have a physician diagnosis of migraine.
This present study observed, among patients with migraine, 63.6% received acute treatment only, 5.4% received prophylactic treatment only, 9.5% received both acute and prophylactic treatment, and 21.6% of patients received no prescription migraine medication. Triptans were the most common medication received, with 62.3% of patients having at least one prescription for a triptan during the follow-up period. Combination NSAID/acetaminophen/aspirin/caffeine treatment was received by more than 20% of patients, and ergotamines were received by 6.1% of patients. Consistent with the Japan Headache Society guidelines for treatment of chronic migraine, calcium-channel blockers were the most common prophylactic medications received in the baseline period, followed by anticonvulsants (9).
This study observed similar treatment patterns as those reported previously in US populations. This analysis found nearly two-thirds of patients discontinued the prophylactic portion of their index migraine treatment regimen, with the medication being restarted in only 15.2% of patients. Lenz and colleagues (15) observed that only 10% of patients who discontinued treatment restarted therapy within a year. Additionally, our study found that less than 10% of patients either switched or augmented medication, which is consistent with Lenz and colleagues (15), who reported that only 13% of patients in their US population either switched or augmented treatment during follow-up. However, unlike Lenz and colleagues (15), our analysis observed very low opiate use (i.e. less than 1% of our sample compared to 53% of patients in the study by Lenz and colleagues (15)). This illustrates a significant difference in physician prescribing patterns for opioids in Japan compared with the US and with countries in the EU, where a self-reported study found that 8.4% of migraine sufferers utilized opioids as acute treatment (16).
This study has several limitations common to analyses of retrospective administrative claims data. Patients were identified based on information available in the claims (i.e. diagnosis, procedure, and drug codes). All diagnosis codes for migraine and other comorbid conditions were recorded for billing purposes, which are subject to coding error. Patient charts were not available to validate diagnoses of migraine or other comorbid conditions, and no information was available on migraine severity or frequency. Studies using administrative codes to identify patients with migraine may miss those who do not seek treatment from a healthcare provider (e.g. patients using over-the-counter medications only). Therefore, this study likely underestimated the incidence and prevalence of migraine. It was not known whether migraine treatments with multiple indications (e.g. anticonvulsants, antidepressants) were dispensed to treat migraines or for other conditions (e.g. depression), so patients may have been incorrectly considered to have received treatment for migraine when the treatment was actually for another comorbid condition. This limitation may be further supported by the observation that patients receiving prophylactic treatment only as their index migraine treatment regimen were slightly older and correspondingly had a slightly higher CCI score compared with patients receiving other index migraine treatment regimens. Therefore, the rate of migraine treatment may be overestimated in this analysis. The use of herbal medicine (which is covered by the Japanese insurance system) was not included in this analysis, as herbal medicine may be used for both prophylaxis and acute treatment; therefore, the rate of migraine treatment may be underestimated in this analysis. Additionally, this study observed that 21.6% of patients did not have any pharmacy claims for migraine treatment – these patients may have received over-the-counter medication that is not included in the insurance database. The JMDC database includes an employed, primarily working-age population, and older individuals are underrepresented (i.e. 10% of the study population are aged 55 years or older) compared with the total Japanese workforce, of which 29% are aged 55 years or older (17). In addition to a possible “healthy worker” bias introduced by the age distribution of the JMDC population, the database represents only 1% of the total Japanese population. Furthermore, persons aged greater than 75 years and those persons covered by other government plans are not included in the database. Therefore, findings may not be generalizable to other populations.
This retrospective database analysis described working patients in Japan with migraine. Prophylactic medication use is low, and patients treated with prophylactic medications as their index migraine treatment regimen were older and had a higher comorbidity burden than patients treated with acute treatment only as their index migraine treatment regimen. Prophylactic use was associated with a high rate of discontinuation following a brief treatment period, and after discontinuation the percentage of patients reinitiating or switching treatment was low, suggesting a high unmet need for new prophylactic therapies.
Institutional Review Board approval
As data used in this study were de-identified and retrospective, RTI International’s institutional review board determined that this study was not research with human subjects.
Key findings
Among Japanese migraine patients, approximately two-thirds received acute treatment only, 15% received prophylactic treatment, and 22% received no treatment. Prophylactic medication use was associated with a high rate of discontinuation (range: 67% among patients initiating prophylactic treatment only to 82.5% among patients initiating both acute and prophylactic treatment) with patients who discontinued therapy receiving treatment for approximately two months. Many patients reinitiated or switched treatment following discontinuation, while a significant proportion of patients remained discontinued from prophylactic therapy, suggesting a high unmet need.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JM and KD are employees of RTI Health Solutions, which received compensation from Amgen Inc to conduct the study. RL and FX are employees and stockholders of Amgen Inc. FS was a consultant hired by Amgen and received compensation by Amgen for his consultation. All listed authors meet the criteria for authorship set forth by the International Committee for Medical Journal Editors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Amgen Inc and conducted by RTI Heath Solutions.