
Abstract
Background
Migraine in children and adolescents is associated with significant disability and a high risk of persistence into adulthood.
Objective
Data on migraine incidence in children and adolescents are few and relatively coarse. To tailor interventions starting shortly after disease onset, detailed information on age- and sex-specific incidence of migraine in children and adolescents is needed.
Methods
We used health care data prospectively collected by the BARMER statutory health insurance, representing ∼11% of the German population. The incidence of migraine diagnoses (International Classification of Diseases (ICD)-10 code G43) in the year 2016 was assessed in subjects aged 0–19 years, who had been continuously insured with the BARMER between 2005 and 2016 or during their entire lifespan.
Results
Data from ∼1.2 million children and adolescents were available. The incidence of migraine diagnoses steadily increased with age, reaching ∼1% per year around the age of 10 for both sexes, and 3.49% per year in females and 1.72% per year in males at the age of 19. Incidences in males and females were similar up to the age of 13 and higher in females from there on. The proportion of incident migraine diagnoses specified as “definite” versus “probable” migraine increased with age.
Conclusion
The present study provides a representative estimation of the first documented health care use for migraine in children and adolescents in Germany within 1-year age bins, separately for boys and girls. These data will be helpful for tailoring early healthcare interventions to reduce disability and prevent migraine chronification.
Introduction
Migraine is a chronic condition that may start early in childhood (1–3). Even in preschool children, migraine has been reported as the most common cause of recurrent and chronic headache (4). Childhood migraine is associated with significant disability, including poor performance at school (5,6) and reduced quality of life (7). In addition, migraine starting in childhood is a persistent disorder. Only 10% of children and adolescents diagnosed with migraine are migraine-free after 1 year (8), and roughly three quarters of the children diagnosed with migraine have recurrent headaches as adolescents and adults, although some switch from migraine to tension-type headache (9,10). Although this has not been shown directly up to now, it would seem that early and effective treatment is important to minimize the impact of migraine in children and adolescents, and maybe even help to reduce persistence into adulthood. Early interventions for migraine in children and adolescents have to be adapted to age, and maybe also to sex, to be successful. Therefore, detailed information of the age- and sex-specific onset of migraine in children and adolescents is needed.
Existing incidence data for this age range are few and relatively coarse, reporting only average incidences within 5- or 10-year age groups. Retrospective assessment of migraine onset is subject to significant recall bias and has to be interpreted with caution even after statistical correction. The American Migraine Prevalence and Prevention (AMPP) study used retrospective data to estimate incidences in children and adolescents, resulting in maximum incidences of 1.56% and 0.62% per year in 15–19 year-old females and males, respectively (11). Prospectively collected data from US medical records and from a UK general practice database for the 0–19 years age range have shown an average incidence of 0.74% per year in 15–19 year-old females (12) and of 0.79% in 10–19 year-old females (13), respectively, while incidences in adolescent males and in children were again lower. The look-back period for differentiating incident from prevalent cases was unspecified (12) or 3 years (13) in these studies, which might be too short when assessing a persistent disorder.
Therefore, there clearly is a need for a more detailed (preferably using 1-year age groups), prospective assessment of age- and sex-specific migraine incidence in children and adolescents, validated by using longer look-back periods. A recent article has highlighted the use of electronic databases for population-based assessment of migraine prevalence (14). Population-based healthcare data in Germany can be assessed from health insurers' databases, since about 90% of the employed people living in Germany have a compulsory statutory health insurance, which includes family members (15,16). Physicians (including general practitioners and specialists) charging for their care within the statutory health insurance have to provide information on the patients' diagnosis, coded in the International Classification of Diseases (ICD-10). Health insurances may thus provide representative long-term data on age- and sex-specific healthcare use.
We had access to the 2005–2016 health care data set of the BARMER, a major German health insurer. In the present study, we used these data to detect the first physician contact leading to a documented migraine diagnosis to estimate age- and sex-specific migraine incidences in children and adolescents within 1-year age cohorts, using a 12-year look-back period. Data from the German health care system additionally provide the opportunity to assess the diagnostic certainty of the diagnoses, forcing physicians to label their diagnoses as “definite” or “probable”. As childhood migraine often presents with symptoms less specific than adult migraine (17,18), we hypothesized that diagnostic certainty would increase from childhood to adolescence.
Methods
Study population
In this study, we analyzed the BARMER data set covering the years 2005 to 2016. With about 8.6 million health insurance holders in 2015, the BARMER GEK is the second largest statutory health insurance in Germany, serving about 11% of the German population (19,20).
The ethics committee of the medical faculty, Ludwig-Maximilians-University Munich, approved the study protocol (17-744 UE).
Main outcomes
Only children and adolescents who were insured at the BARMER during the entire period from 2005 to 2016 (or during their entire lifespan for children aged 12 years or younger) were included in the present study, both for cases with a migraine diagnosis and controls. We identified cases with a first documented diagnosis of migraine (ICD-10 code G43) within the calendar year 2016. This was done separately for males and females in each of the 1997 to 2016 1-year birth cohorts; that is, in children and adolescents aged 0–19 years in 2016. Prevalent cases were differentiated from incident cases using a look-back period of 12 years (for adolescents aged 13 years and above) and the entire lifespan for children between 0 and 12 years. Therefore, an incident case was defined as a case having a migraine diagnosis in 2016 but no migraine diagnosis between 2005 and 2015. Age- and sex-specific incidence of migraine diagnoses was then calculated as the number of incident cases within the respective birth cohort in 2016, divided by the size of the birth cohort. For ease of interpretation, the incidence of migraine diagnoses for each birth cohort was labeled as, for example, “the incidence of migraine diagnoses in four year old children”, but more precisely it would have to be called “the incidence of migraine diagnoses in children turning four years of age in 2016”.
The German health care system requires further specification of the certainty of ICD-10 diagnoses as “definite” or “probable”. In the main analysis, we looked at all incident migraine diagnoses (definite and probable). In an additional analysis, we looked at the age dependence of the proportion of definite versus total (definite and probable) incident migraine diagnoses. It is important to mention that the “definite” and “probable” migraine diagnoses used in the German health care system do not necessarily correspond to “migraine” versus “probable migraine” as defined by the Classification of Headache Disorders (ICHD-3 (22)), as not all physicians are sufficiently acquainted with the ICHD-3 criteria.
Age-specific incidences of migraine diagnoses stratified by sex.
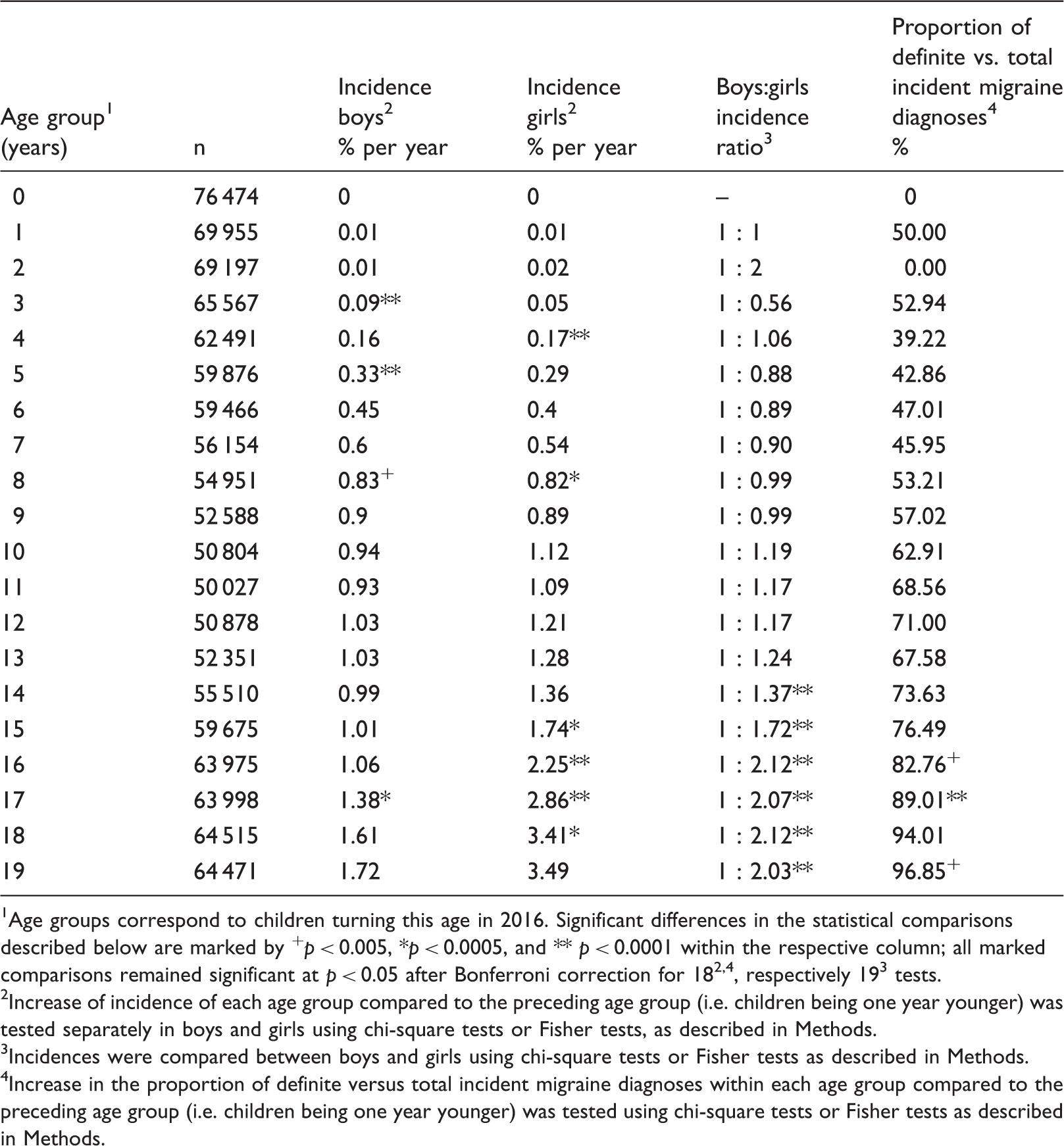
Age groups correspond to children turning this age in 2016. Significant differences in the statistical comparisons described below are marked by +p < 0.005, *p < 0.0005, and ** p < 0.0001 within the respective column; all marked comparisons remained significant at p < 0.05 after Bonferroni correction for 182,4, respectively 193 tests.
Increase of incidence of each age group compared to the preceding age group (i.e. children being one year younger) was tested separately in boys and girls using chi-square tests or Fisher tests, as described in Methods.
Incidences were compared between boys and girls using chi-square tests or Fisher tests as described in Methods. 4Increase in the proportion of definite versus total incident migraine diagnoses within each age group compared to the preceding age group (i.e. children being one year younger) was tested using chi-square tests or Fisher tests as described in Methods.
Incidences of migraine diagnoses stratified by sex, summarized for 5-year age groups.
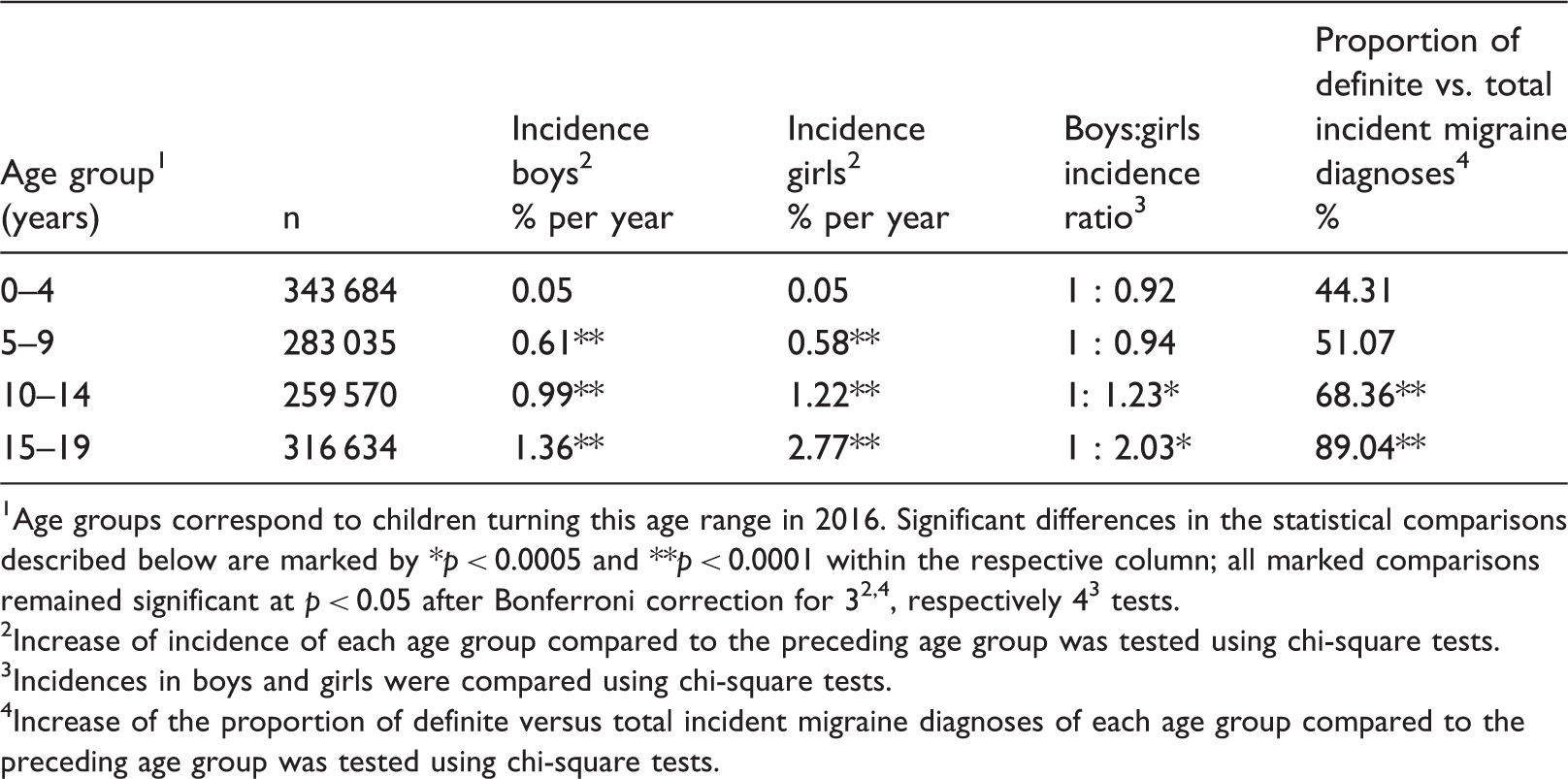
Age groups correspond to children turning this age range in 2016. Significant differences in the statistical comparisons described below are marked by *p < 0.0005 and **p < 0.0001 within the respective column; all marked comparisons remained significant at p < 0.05 after Bonferroni correction for 32,4, respectively 43 tests.
Increase of incidence of each age group compared to the preceding age group was tested using chi-square tests.
Incidences in boys and girls were compared using chi-square tests.
Increase of the proportion of definite versus total incident migraine diagnoses of each age group compared to the preceding age group was tested using chi-square tests.
Statistical methods
Differences in incident migraine diagnoses between boys and girls were tested using chi-square statistics within age groups. To test for an increase of incident migraine diagnoses with age, the incidence within each age group was compared to the incidence in the preceding (next younger) age group using chi-square statistics. Finally, to test for an increase in the proportion of definite diagnoses with age, the proportion of definite diagnoses within each age group was compared to the proportion in the preceding (next younger) age group using chi-square tests.
Because of the low numbers of incident cases in the age groups of children aged 0–2 years, Fisher tests were performed instead of chi-square tests. For all tests, Bonferroni correction was applied. Two-tailed tests were used throughout. p < 0.05 was considered significant. All analyses were performed with SAS Enterprise guide 7.1.
Results
Data from n = 50,027 to 76,474 children and adolescents per 1-year age group are included in the analysis (Table 1), with a slight preponderance of boys (boys:girls ratios ranged from 1:0.93 to 1:0.98, see also Supplementary Table 1). Incidences of migraine diagnoses stratified for sex are given for 1-year age groups in Table 1 and Figure 1. For ease of comparison with previous studies, incidences of migraine diagnoses are also presented within 5-year age groups in Table 2.
Incidence of migraine diagnoses stratified by age and sex in 2016 in the 0–19 years age groups, corresponding to the 1997 to 2016 birth cohorts. Age groups correspond to children turning this age in 2016; * denotes a significant difference between boys and girls in the corresponding age group (p < 0.05 after Bonferroni correction). See Table 1 for more details.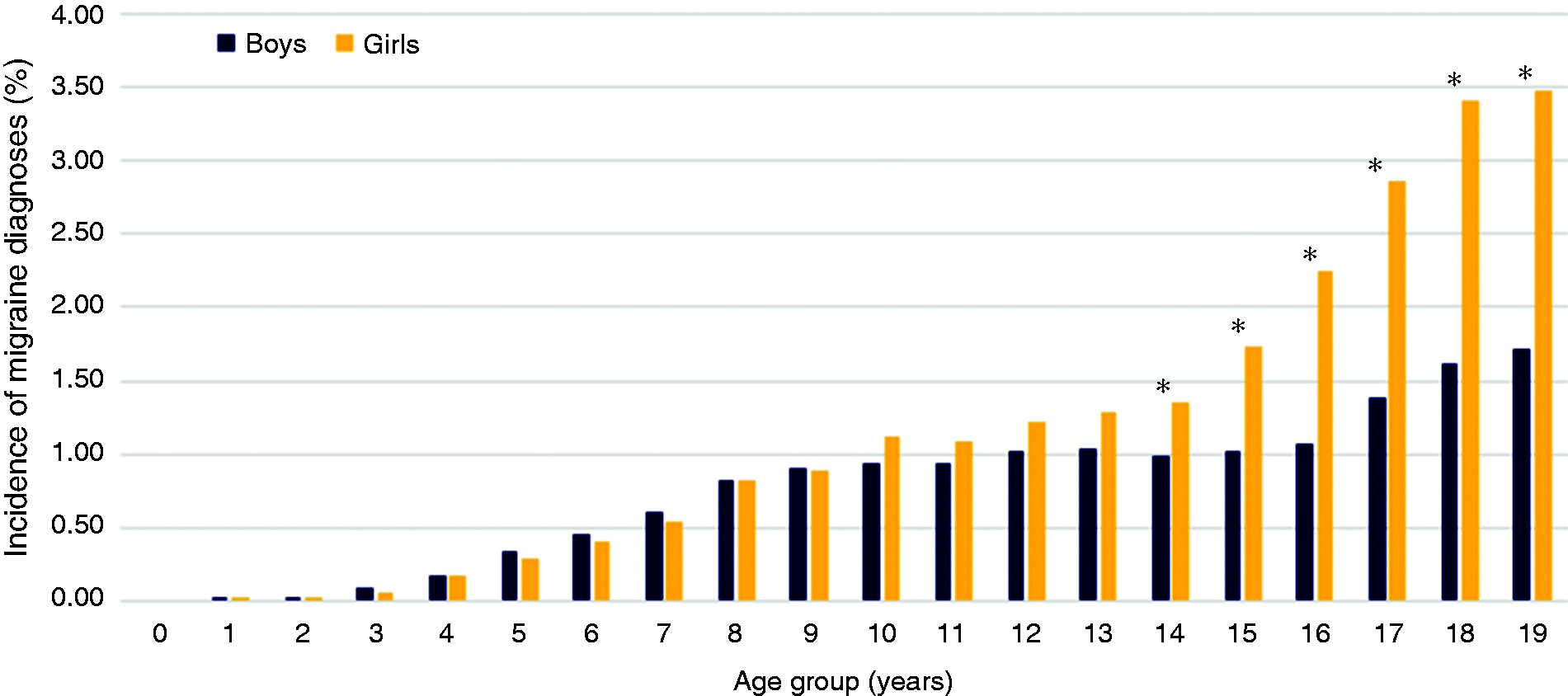
Higher incidence of migraine diagnoses in girls compared to boys starting at the age of 14
Boys:girls ratios for incident migraine diagnoses ranged from 1:0.56 at the age of 3 to 1:2.12 at the age of 18. Incidence of migraine diagnoses was significantly higher in girls than in boys starting from the age of 14 when looking at the 1-year age groups (Table 1) and starting from the 10- to 14-year age group when looking at the 5-year age groups (Table 2). No significant differences between boys and girls were observed before that age.
Increase of incident migraine diagnoses with age in boys and girls
The incidence of migraine diagnoses increased with age, starting at almost 0 for the youngest age groups, leveling at ∼1% for both sexes around 10 years of age and reaching a maximum of 3.49% for girls and 1.72% for boys at the age of 19 (Table 1, Figure 1). Significant increases compared to the preceding (next younger) 1-year age group could be found intermittently between 3 and 8 years of age in both sexes and continuously starting from 15 years in girls (Table 1). When 5-year age groups were analyzed, a significant increase of the incidence of migraine diagnoses for all age groups, compared to the respective next-younger age group, was observed in both boys and girls (Table 2).
Increase of the proportion of incident migraine diagnoses labeled as “definite migraine” with age
In the German health care system, the certainty of ICD-10 diagnoses has to be further specified as “definite” or “probable”. Proportions of definite versus all incident migraine diagnoses are given in Tables 1 and 2 (pooled for boys and girls) and in Supplementary Table 1 (separately for boys and girls). The proportion of incident definite migraine diagnoses was around 50% until the age of eight, and then increased up to 97% at the age of 19 (Table 1). In the data pooled between boys and girls, significant differences in the proportions of definite diagnoses were found at 16, 17 and 19 years, compared to the respective preceding (next younger) 1-year age group (Table 1). When 5-year age groups were used, a significant increase in the proportion of definite migraine diagnoses compared to the next-younger age group was observed in the 10–14 and 15–19 years age groups (Table 2). There were no differences between boys and girls except for a small excess of the proportion of definite migraine diagnoses in girls in the two highest age groups (age 18: Boys 88.61%; girls 94.01%; p = 0.0002 and age 19: Boys 91.25%; girls 96.85%; p < 0.0001, Supplementary Table 1).
Discussion
The present study for the first time provides data on the incidence of migraine diagnoses in children and adolescents within 1-year age cohorts, validated by a look-back period of 12 years (respectively the entire lifespan for children aged below 12). In addition, we were able to show that (1) incidences of migraine diagnoses are significantly higher in girls compared to boys from 14 years on, but similar in both sexes before that age; (2) that incidences of migraine diagnoses increase with age in both sexes; and (3) that the proportion of additional labeling of incident migraine diagnoses as “definite” migraine also increases with age.
Higher migraine incidences in girls compared to boys starting from puberty have been repeatedly reported (11–13), but most studies have not tested statistical significance. Our data reveal higher incidences of migraine diagnoses in girl versus boys starting from 10 years, which became statistically significant at a 1-year basis starting from 14 years. The boys:girls ratio reached a maximum of ∼1:2 at 16 years of age. A previous study had suggested higher migraine incidences in boys versus girls below the age of 10 (21), but this was not confirmed by subsequent results (11–13), and also not by our data.
Migraine incidences increase with age during childhood and adolescence. Previous studies within this age range have reported peak incidences in the 15–19 year-old group (11), within the 10–19 year-old group (13) and within the 15–19 year-old group for females and the 10–14 year-old group in males (12). Our data extend the previous results, showing a rather continuous increase from year to year of incident migraine diagnoses, starting at 0% at the age of 0 and increasing to 1.72% in males and 3.49% in females at the age of 19. Data in Table 1 show that significant numbers of children suffer from migraine starting from early school age, with incident migraine diagnoses ∼0.4% at the age of 6 and ∼1% at the age of 10. Migraine in children is associated with significant disability and reduced performance in school (5–7) and tends to persist into adolescence and adulthood (8–10). Our data show that there may be a window of opportunity for early interventions in children with migraine at primary school age, with the aim of reducing disability and chronification. This must be tested in randomized controlled trials.
Childhood migraine often presents with symptoms less specific than adult migraine. Attacks are often short ( < 2 hours), with bilateral and pressing headache. Typical duration > 4 hours, unilateral and pulsating pain often arise only in late adolescence (17,18). This may lead to more uncertainty in migraine diagnoses in younger children. In the German coding system, ICD-10 diagnoses are additionally labeled as “definite” or “probable”, reflecting the degree of certainty of the physician towards the diagnosis. Indeed, the number of definite incident migraine diagnoses in our sample significantly increased with age, from around 50% up to the age of 8 to 97% at the age of 19. An adaptation of the migraine criteria for children has been discussed for years (17,18), but consensus has not been reached. The current Classification of Headache Disorders (ICHD-3 (22)) permits an attack duration of 2–72 hours for children and adolescents (compared to 4–72 hours for adults) but the remainder of the criteria are the same for both groups. To further complicate things, a considerable proportion of children switch from migraine to a non-migrainous headache (e.g. tension-type headache) or vice versa between childhood and adolescence, and on to adulthood (10,23). In conclusion, our data statistically corroborate the increasing diagnostic certainty with age, underlining the need for a better conceptualization of migraine and headache in childhood.
Compared to previous studies, migraine incidences were high in the present study, especially in the older age groups. For example, in our analysis, girls in the 15 to 19-year age group showed an average yearly migraine incidence of 2.77%, while in the AMPP study, this was estimated to be 1.56% (1.36% and 0.62% for boys, respectively) (11). This might be due to several differences between the two studies. First, while our study assessed the incidence of migraine diagnoses prospectively, the AMPP study estimated incidences based on retrospective report of migraine onset. In retrospective report, subjects tend to overestimate the age of onset, and more so the longer ago the symptoms started (telescoping phenomenon) (21). Although the study tried to statistically account for this, it might have contributed to underestimation of migraine incidences at young ages. In addition, the AMPP study only included subjects reporting “at least occasional severe headache” as identified by the head of household. This might underestimate true incidences, as migraine is not always severe, the head of household may not be aware of all cases, and remitted cases are excluded. On the other hand, the AMPP study was a mailed survey to a representative US population sample, which may have reached subjects not seeing a physician because of their headache. Another study, based on review of medical records from the years 1989–1990 in Olmsted County, US, found incidences of 0.74 for females and 0.29 for males in 15 to 19-year-olds (12). A study using diagnoses from the General Practice Research Database in the UK between 1994 and 2001 with a look-back period of ≥ 3 years reported migraine incidences of 0.74% per year in females and 0.50% in males in the 10- to 19-year age group (13). Although the approach of data collection in these two studies was similar to our study, different incidences might be due to differences in health care utilization between countries and between periods of data collection. In Germany, seeing a doctor does not produce extra cost for those with a statutory health insurance (as in our study population), and appointments with a general practitioner or pediatrician are readily available. This leads to a larger health care utilization for disorders that might not be regarded as potentially dangerous, such as recurrent headache. On the other hand, much higher migraine incidences than ours have also been reported. In a Finnish study conducted in 2002 in 7-year-old children examined by their school doctor, 6-month migraine incidence was ∼13.0% in a sample of ∼1000 children (24). Wrongly classifying prevalent cases as incident cases might also explain high incidences of migraine diagnoses. However, this is unlikely because the 12-year look-back period used in the present study largely exceeded that of the previous studies. High incidences of migraine diagnoses might also arise where physicians had a monetary interest in coding other types of headache as migraine. However, coding is unlikely to be influenced by monetary interests as payment in German ambulatory care is by case, not by diagnosis. An uncertainty remains because coding physicians were not specifically trained in headache. However, the expected increase in proportion of definite migraine diagnoses from childhood to adolescence shows that the physicians were to a certain point familiar with the migraine criteria, which, as discussed above, were developed for the diagnosis of migraine in adults but do not always adequately reflect the presentation of childhood migraine. In conclusion, we believe that our incident migraine diagnoses provide a realistic estimate of migraines severe enough to prompt a first physician visit in Germany in 2016.
Strengths and difficulties
The major strength of the present data is the large sample (∼1.2 million) of children and adolescents (0–19 years) continuously insured over 12 years, allowing for prospective assessment of the incidence of migraine diagnoses in the year 2016. Looking back over the entire lifespan in children younger than 13 years assures definitely valid incidences in this age group. The extensive look-back period of 12 years in those 13 years of age and older reduces the risk of overestimating incidences by misclassification of prevalent cases.
External validity of the BARMER data might be an issue. About 8% of the children living in Germany are insured with the BARMER (19), with demography similar to the German average (data not shown). Data comparing socio-demographics and health status of German speaking BARMER-insured adults to the German average show that the highest academic achievement in BARMER-insured adults was slightly above, smoking was slightly below, and body mass index almost identical to the German average (25). This demonstrates a representative socio-demographic background of BARMER-insured children, who have their insurance access through their parents. However, it clearly remains to be demonstrated how these data can be generalized to other countries.
It is important to emphasize that estimation of migraine incidences from health care utilization data is not equivalent to assessing population-based incidences. One problem of using healthy insurance records is the underestimation of incidences resulting from the fact that not all children and adolescents afflicted with migraine necessarily seek medical care and, even if they do, they may not do so in the year of first occurrence. In addition, the inclination of parents to take their child to the doctor for headaches might depend on the child's age and even sex and be lower in parents suffering from migraine themselves because they are familiar with basic headache treatment. All this may result in a distortion of incidence patterns. It is difficult to estimate the size of these effects. A previous German study showed that 31% of children with headache (independent of type) had seen a doctor for their headache in the previous 6 months (26). In a large Brazilian study, 72% of children with migraine had seen a doctor for their headache (27). In a health system where consultation of a physician does not produce extra cost, diagnosed migraine likely corresponds to the more severe/disabling cases of migraine. The incidence of diagnosed migraine is also interesting because it represents the earliest time of physician-initiated treatment (e.g. the earliest time where a child could be referred to a specialized headache treatment program).
Another point is that we had to rely on migraine diagnoses by pediatricians and general practitioners, not all of whom might be fully acquainted with the ICHD migraine criteria. This might also have led to the (small) number of migraine diagnoses made in children before the age of four, where state-of-the-art migraine diagnoses are difficult because of the limited capacity of the child to describe pain and accompanying symptoms. Unfortunately, we had no opportunity to validate diagnoses because the data were anonymous to comply with German data confidentiality laws.
Finally, comparing each 1-year age group with the next-younger 1-year age group for detecting age-related increases in incidence of migraine diagnoses may underestimate increases that are small but constant from year to year. In this case, looking at the 5-year age groups may provide a better estimate of increase with age.
Conclusion
The present data provide prospectively assessed yearly incidences of migraine diagnoses in a large, representative sample of children and adolescents (aged 0–19 years) from the German population, validated by using a 12-year look-back period. Incidences steadily increased with age, being around 1% per year at the age of 10 for both sexes and reaching 3.49% for females and 1.72% for males at the age of 19. The time of the first migraine diagnosis represents the earliest possible time of health care intervention for these children and adolescents.
Supplemental Material
Supplemental material for Age- and sex-specific first health care use for migraine in 2016 in children and adolescents from prospectively collected health insurance data in Germany
Supplemental Material for Age- and sex-specific first health care use for migraine in 2016 in children and adolescents from prospectively collected health insurance data in Germany by Lucia Albers, Rüdiger von Kries, Andreas Straube, Florian Heinen, Mirjam N Landgraf, Viola Obermeier and Ruth Ruscheweyh in Cephalalgia
Footnotes
Public health relevance
The present study for the first time gives sex- and age-specific incidences of migraine diagnoses in children and adolescents within 1-year age bins, based on German health care data on ∼12 million subjects, using a look-back period of 12 years.
It also shows that diagnostic certainty of migraine diagnoses increases from childhood to adolescence, likely because childhood migraine often presents with less specific symptoms than adult migraine.
Acknowledgements
The authors thank Ursula Marshall (BARMER) for providing access to the BARMER health insurance data and Joachim Saam (BARMER) for his tremendous help in coping with the data structure.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RR has received honoraria and/or support for travel from Novartis, Hormosan, and Allergan. FH received honoraria/unrestricted educational grants from (in the last 3 years): Allergan, Merz, Ipsen, Novartis, and Desitin. ML, RvK, LA, and VO declare no conflicts of interest.
Ethics
The study has been approved by the ethics committee of the medical faculty of the Ludwig-Maximilians-University, Munich 17-744 UE.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.