
Abstract
Sudden onset headache is a common condition that sometimes indicates a life- threatening subarachnoid haemorrhage (SAH) but is mostly harmless. We have performed a prospective study of 137 consecutive patients with this kind of headache (thunderclap headache = TCH). The examination included a CT scan, CSF examination and follow-up of patients with no SAH during the period between 2 days and 12 months after the headache attack. The incidence was 43 per 100 000 inhabitants > 18 years of age per year; 11.3% of the patients with TCH had SAH. Findings in other patients indicated cerebral infarction (five), intracerebral haematoma (three), aseptic meningitis (four), cerebral oedema (one) and sinus thrombosis (one). Thus no specific finding indicating the underlying cause of the TCH attack was found in the majority of the patients. A slightly increased prevalence of migraine was found in the non-SAH patients (28%). The attacks occurred in 11 cases (8%) during sexual activity and two of these had an SAH. Nausea, neck stiffness, occipital location and impaired consciousness were significantly more frequent with SAH but did not occur in all cases. Location in the temporal region and pressing headache quality were the only features that were more common in non-SAH patients. Recurrent attacks of TCH occurred in 24% of the non-SAH patients. No SAH occurred later in this group, nor in any of the other patients. It was concluded that attacks caused by a SAH cannot be distinguished from non-SAH attacks on clinical grounds. It is important that patients with their first TCH attack are investigated with CT and CSF examination to exclude SAH, meningitis or cerebral infarction. The results from this and previous studies indicate that it is not necessary to perform angiography in patients with a TCH attack, provided that no symptoms or signs indicate a possible brain lesion and a CT scan and CSF examination have not indicated SAH.
Introduction
Patients with severe headache of sudden onset commonly attend emergency units. This kind of headache may herald a potentially life-threatening subarachnoid haemorrhage (SAH) but most patients have a benign condition. Table 1 lists possible causes of sudden onset headache (1–11).

In 1986 Day and Raskin used the expression thunderclap headache (TCH) for sudden onset headache in a report of a patient with three attacks of TCH within 8 days (12). An SAH was excluded by computerized tomography (CT) of the brain and CSF examination including spectrophotometry, but after the third attack a carotid angiography was carried out. It showed a middle cerebral artery aneurysm that was successfully operated on. This case raised the question of whether angiography is sometimes indicated even if an SAH has been excluded by CT and CSF examination.
In the literature it has been reported that 20–60% of patients with SAH have experienced a previous attack of sudden onset headache (13–24). This headache has been suspected to indicate a ‘warning leak’ preceding the following SAH.
Several studies have been published since this case report with a bearing on the role of angiography, closely linked to the discussion of warning leaks.
In a retrospective Dutch study 71 patients with TCH, normal CT scans and CSF were followed for a mean of 3.3 years (25). None of the patients had an SAH during follow-up, but 17% had recurrent attacks of benign TCH (=non-SAH).
In an English investigation 14 of 49 patients who were acutely referred to a hospital because of TCH were found not to have an SAH (7). The non-SAH patients were followed prospectively for 18–36 months and no SAH occurred. In a third prospective study 18 patients with TCH were followed for a mean of 20 months (26). No patient had an SAH during follow-up. A fourth study was retrospective and included 93 patients with benign TCH who were followed for 1 year (16). This study aimed at evaluating the role of warning leaks, but because only 2/37 patients with SAH had had previous bouts of sudden headache, the authors concluded that early recognition of SAH would have only a limited impact on outcome in the general population. They stated that earlier results supporting the idea of a warning leak might have been the result of recall bias, and minor headaches in the past being over-interpreted as minor bleeds. A later study from the same group comparing the headache characteristics of SAH and benign TCH in a prospective manner (27) revealed comparable figures regarding preceding headache: 19% in the SAH patients and 14% in the benign TCH patients. The Dutch studies have included patients with a ‘semisudden’ headache with an onset as long as several minutes (25, 27).
The present study was prospective and aimed at showing the incidence, characteristics and causes of TCH in an unselected population. The term thunderclap headache is used to name a headache that reaches maximum intensity within 10 seconds, whatever the cause may be.
Methods
During a 31-month period, all patients seeking or referred to the emergency department at the University Hospital of Linköping, Sweden, because of sudden onset headache, were considered for inclusion in the study. The patients were examined by the neurologist on call.
The catchment area of the hospital has 118 000 inhabitants >18 years of age.
Calculations of incidences were based on patients included over a 19-month period when conditions at the emergency department were optimal for an incidence study. During this period all patients attending the emergency department within 10 days after onset of a headache with an onset time of <10 s could be included, whereas a few patients during the rest of the study period might not have been reported to the investigators. All patients received a thorough neurological examination and the history was recorded according to a protocol including the onset and features of the headache, other neurological symptoms, previous headache experiences, heredity for headache, etc. A CT scan (GE 9800) was performed acutely. If no definite cause was found on CT, a spinal tap was done >6 h after the onset of the headache, unless contraindications existed. The CSF examination included cell counts, spectrophotometry at 415 nm and 455 nm, and protein analysis.
Patients without SAH were followed up by telephone interview 2–4 days, 7–9 days, 1 month, 3 months, 6 months and 12 months after onset. The primary objective was to monitor recurrence of TCH attacks. The patients were also advised to contact the neurologist on call if they had a new TCH attack. Altogether 162 patients with TCH were recorded and 137 of them fulfilled the criteria for inclusion (Table 2). The patients excluded were five who refused both CT scan and spinal tap, another 19 patients who refused spinal tap and one patient on anticoagulant therapy. Five non-SAH patients received a diagnosis without a spinal tap having been shown on CT of: an acute cerebral infarction (two); an intracerebral haematoma (one); brain oedema (one); and an intraventricular haemorrhage (one). During the 19 months of the incidence study 80 patients were included (Table 2).
Number of patients with thunderclap headache divided into a group with subarachnoid haemorrhage (SAH) and another group with other causes (non-SAH)

Statistical methods
In the statistical analyses Fischer's exact test and Mann–Whitney's unpaired t-test were applied using the Statview software program.
Results
Patients with SAH were older (mean=56 years, median=58) than non-SAH patients (mean=42 years, median=39; P=0.0002). Altogether 23 patients had an SAH, i.e. 17% for the whole study period, but in the group of 80 patients included during the incidence study period, the proportion of SAH was only 11.3% (n=9). This figure is more accurate because of the better control of the material during this period, with a more complete reporting and referral of patients with sudden onset headache.
Five of the SAH patients had a normal CT scan but CSF findings showing an SAH. Of the non-SAH patients, 101 (89%) had a normal CT scan, whereas five patients (4%) had cerebral infarction (three new, one old, one of uncertain age) and three had intracerebral haemorrhage. Four patients who were not examined with CT for various reasons had a normal CSF and were therefore considered sufficiently investigated to be included. Ninety per cent (102/114) had a normal CSF examination but four patients had signs of aseptic meningitis. Documentation of the exact time of TCH onset was obtained in 16/23 SAH cases and when the mean time until radiological examination was calculated there was no difference (P=0.46) between the group of patients with a negative CT scan and those in whom an SAH was diagnosed by the CT scan (mean time 48 h, range 3–192 h, and 34 h, range 1–120 h, respectively).
Statistical analysis was performed using the Mann–Whitney test.
The incidence of TCH of all causes was 43/100 000/year >18 years of age. The incidence of TCH caused by SAH was 5 and for non-SAH (completely investigated) 38/100 000/year.
TCH was reported by all patients as an alarming experience with severe pain and/or dramatic symptoms. Eighty-six per cent had an extremely rapid onset of less than two seconds.
The majority of the patients were resting or in calm activity at onset (61% of the SAH patients, 66% of the non-SAH patients). Seventeen per cent of the SAH patients and 21% of the non-SAH-patients were physically active or were in a Valsalva situation. In 8% the onset occurred during intercourse (nine men and two women), two of the men had SAH but none of the women. Five of the 11 patients with coital TCH had previous experience of coital TCH (=45%). Eight per cent of all patients reported previous coital TCH, regardless of their degree of activity at time of the TCH that brought them to hospital (12% of the men, 4% of the women).
The quality, location and intensity of the headache, and associated symptoms and signs, differed somewhat between SAH and non-SAH patients (Table 3 and Table 4).
Clinical symptoms in patients with SAH and non-SAH thunderclap headache

Headache intensity at onset and after 1 h in patients with SAH and non-SAH thunderclap headache (n=137). Percentage of patients
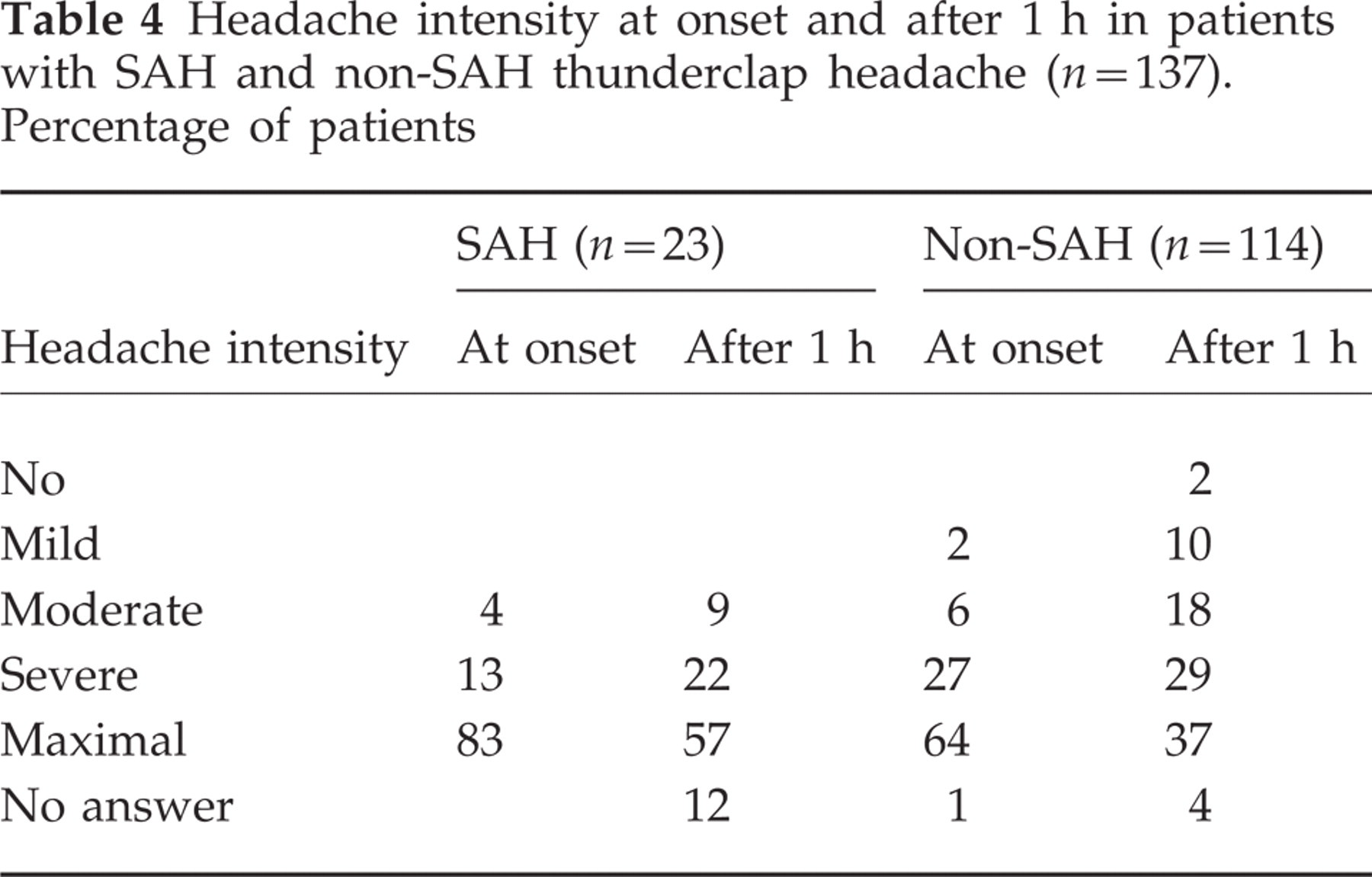
The following were more common (Fisher's exact test) in SAH patients: occipital location (P=0.03), nausea (P=0.007), neck stiffness (P<0.0001) and impaired consciousness (P=0.03). Pressing (P=0.03) quality and temporal location (P=0.009) were more common in non-SAH patients. It should be noticed that no symptom or sign was pathognomonic for SAH or non-SAH.
Figure 1 shows that 25 of the non-SAH patients monitored for 1 year had 83 recurrent attacks of TCH (24%). Four of the patients with SAH (17%) reported previous TCH: one had coital TCH 16 years earlier, another had TCH 11 years earlier after an infection and one patient had a SAH 5 years earlier and now had a new TCH and a re-bleeding; finally, one patient had TCH the day before the attack that brought him to hospital. In the non-SAH group, 29% had previous experience of TCH.

Number of patients with recurrence of thunderclap headache attacks during various time periods after the initial attack in non-SAH patients (n=103 followed-up during 1 year). 25 patients had recurrent attacks.
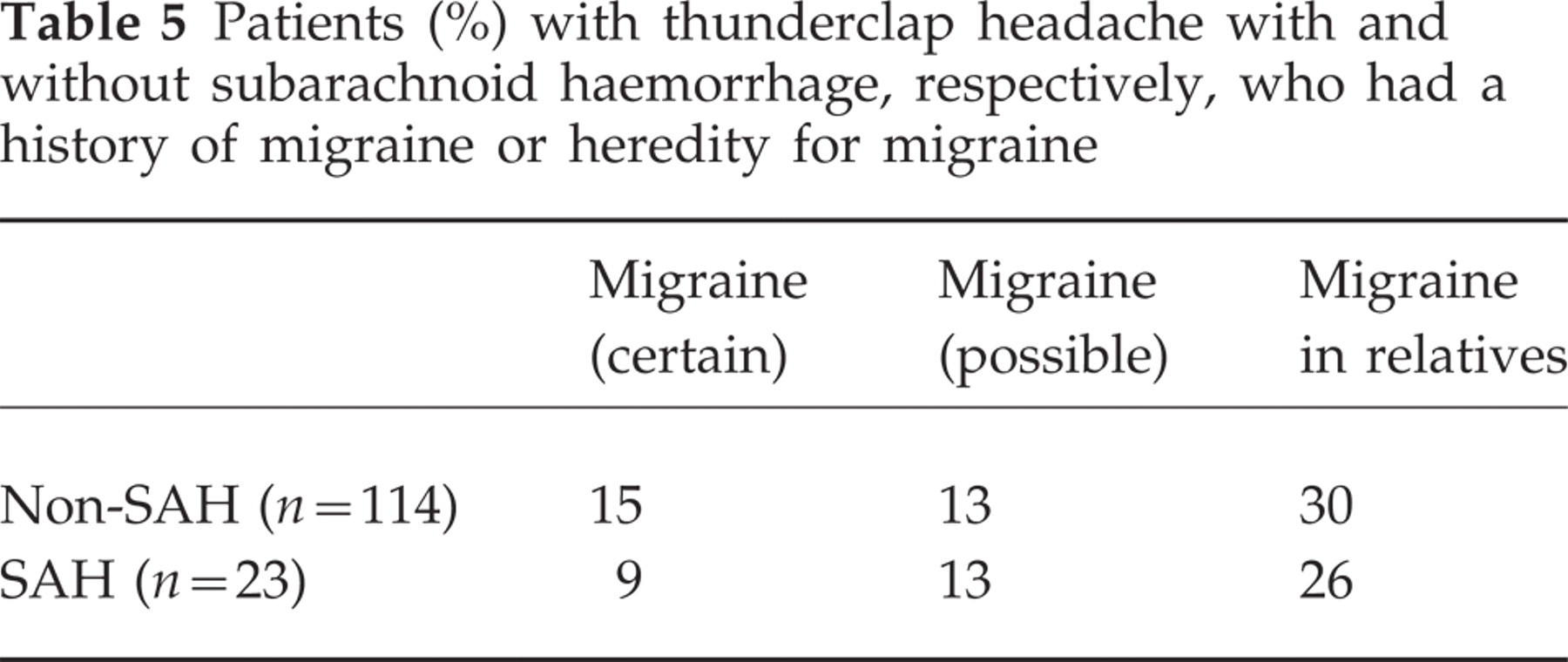
Twenty-eight per cent of the patients with TCH without SAH had certain or possible migraine, compared with 22% for SAH patients (P=0.56). A detailed history was obtained and checked by the investigators and the migraine diagnosis was made according to the IHS criteria for migraine (see Table 5).
Patients (%) with thunderclap headache with and without subarachnoid haemorrhage, respectively, who had a history of migraine or heredity for migraine
Certain or probable tension headache during the 3 months prior to TCH was found in 25% of the non-SAH group, 75% of whom were women, and in 9% of the SAH group, all of whom were women.
Only one SAH patient (4%, n=23) can be regarded as having had a true sentinel headache. Three patients, however, had preceding TCH but with an interval of several years.
Discussion
All patients with sudden onset headache less than 11 days before they were examined were primarily included regardless of what was later found to be the cause (=162). This inclusion criterion was chosen because it reflects the situation in the emergency unit as well as the situation for the patients. For reasons given in the Methods section, 25 of them were not included in the final analysis. The overall incidence of TCH was found to be 43/100 000 inhabitants >18 years of age/year, which to our knowledge is the first estimate that has been done.
SAH as a cause of TCH
During the incidence study period 11.3% of the TCH attacks that first brought the patients to the hospital were caused by an SAH. This gives an incidence figure of 5/100 000 adult inhabitants/year. This is much lower than the proportion of SAH in an English study (7) in which 70% of the patients referred to the hospital had SAH. The explanation for this high proportion is evidently the referral pattern, where only the most severely affected patients were referred for further examination. This is probably also the explanation for the high percentage, 40%, of SAH in a Dutch study (27).
The importance of the referral pattern and the degree of compliance with the study protocol at the emergency unit is illustrated by the fact that a higher proportion of TCH patients were found to have SAH during the period not included in the incidence study, namely 21.2%. Not all of the light and moderately affected patients were included during this period, but as SAH-patients are more often severely affected than non-SAH patients, they were more often referred to the neurologist. This leads to an under-reporting of benign TCH.
The reported incidence figures for SAH are 2–10/year and 100 000 adult inhabitants (1, 16, 21). Our incidence numbers are in the lower interval because we only include SAH with TCH at onset. Interestingly, for 5 of 23 patients with SAH the diagnosis could not be made at CT, but only after CSF spectrophotometry, which underlines the role of the CSF examination.
Possible causes of benign TCH
One of the major conclusions of this study is that sudden onset headache is mostly a benign condition. In most of these patients it was not possible to determine the cause of the attack. Some findings were made, though their significance for the headache attack remains unknown (Table 6). It is reasonable to suspect, however, that the intracerebral haemorrhages, the ‘new’ infarctions (three of the five), the sinus thrombosis and the cerebral oedema could have caused the headache attack. The aseptic meningitis might also have been a deciding factor.
CT and CSF findings in patients with thunderclap headache

Both Wijdicks et al. (25) and Harling et al. (7) argue that migraine and tension-type headache might be significant background factors in the occurrence of benign sudden onset headache. Wijdicks et al. reported that 44% of patients had a history of one of these types of headache. We found a slightly increased prevalence of migraine compared with the point prevalences in a recent Danish study, RR 1.3, P=0.06 (28). This might be a background factor, whereby an inherited increase in reactivity of the cranial blood vessels and their nociceptive nerve fibres leads to attacks of headache and other symptoms, although generally not of a sudden onset. The high incidence of nausea in the non-SAH group supports this idea (61%).
A recent report of two patients with repeated TCH points to another possible cause of the acute headache, namely diffuse multifocal segmental vasospasms involving all cerebrovascular territories (11). It was shown in angiograms (one by MRI, the other by intrarterial contrast angiography) 6 days and 7 days, respectively, after the headache attacks. None of the patients had symptoms or signs indicating brain dysfunctions. It appears that the vasospasms were spontaneously reversible. Suspicions of cerebral arteritis arose but this does not appear to evoke THC and the benign course also speaks strongly against arteritis as a course of THC.
Activities at onset: coital headache
Eight per cent of our patients had coital TCH, which has been described previously (2, 29, 30). Wijdicks et al. reported that 4% had onset during intercourse (25). This appears to be more common in men than women (2), as also was the case in our material (9 men, 2 women). It has been suggested that the headache attacks are evoked by an increase in blood pressure during orgasm, the systolic pressure rising by 40–100 and the diastolic pressure by 20–50 mmHg (31).
About one-third of the patients were engaged in strenuous activities, including sex, at the onset of the TCH (39% and 34% of SAH and non-SAH patients, respectively). The results obtained in the prospective study by Linn et al. were 50% and 22% of SAH and benign TCH patients, respectively (27). In the retrospective study of 71 patients with benign TCH by Wijdicks et al. (25) the figure was 28%, and in the English study by Harling et al. (7) the figures were 28% of SAH patients and 21% of non-SAH patients. However, in the small prospective study by Markus (26) the numbers were smaller, 8% and 19% of SAH and non SAH-patients, respectively.
Symptoms and signs
When the headache features and neurological symptoms in SAH and non-SAH patients were compared some differences were found (Table 4). Nausea, neck stiffness
In the study by Linn et al. in 1998 (27) 26% and 16% of patients with SAH and benign TCH, respectively, had transient loss or clouding of consciousness, which is in accordance with our findings. In Linn's study nausea also had an occurrence similar to ours, i.e. around 75% in both groups. In the study by Markus 60% and 88% of SAH and benign TCH patients, respectively, had nausea (26). Linn interestingly reported the exclusiveness of two symptoms in SAH patients, namely diplopia and seizures, and proposed these to be pathognomonic signs, having, however, a very low frequency. This is not supported by our results, where none of the SAH patients but 2% of the non-SAH patients had diplopia. No patient in our material had seizures.
These results are in good agreement with the generally accepted notion about the clinical profile of SAH. It should be noticed that even though there are differences in the frequencies of the symptoms and signs between patients with TCH of SAH and non-SAH origin, there are also similarities between the two groups. One further important conclusion from these data is that there are no pathognomonic symptoms or signs that enable a reliable clinical differentiation between SAH and non-SAH forms of TCH.
Recurrences of benign TCH
Recurrences are common after the initial attack of benign TCH. In the present material, 24% had at least one recurrent attack during follow-up (Table 5). They most commonly occurred during the first 30 days. Only two of the patients had attacks during the second half of the 1-year follow-up period. The recurrent attacks were similar to the original attack. The patients with recurrences were interviewed and in some cases also examined at the outpatient clinic. No indication for renewed CT and CSF examination was found and it was concluded that no patients had had an SAH as it had been ruled out at the initial attack.
Our figures regarding recurrence are comparable with the results in Markus' small study, which reports 25% recurrence in a material of 16 patients with benign TCH (26). Our results are somewhat higher than those obtained by Wijdicks et al. (25), who had a follow-up period of 1–7 years (mean 3.3) and reported a recurrence rate of 17%, and by Linn et al. (16), who found recurrences in 12% over a 1-year follow-up.
Is angiography indicated after normal CT and CSF results?
In the prospective study by the Dutch group the significance of warning leaks was questioned as only 2/37 of the SAH patients had had a previous attack of headache. Our study partly supports this statement, with only one of 23 patients with SAH (4%) regarded as possibly having had a warning leak. On the other hand some of our patients with a rather mild TCH unexpectedly ended up with an SAH diagnosis. It should be noted that our indication for investigation was founded on the rapidity of onset rather than the intensity or the duration of the headache.
In the discussion of sudden headache and ‘warning leaks’ preceding a SAH it is relevant to ask the question: is it possible that an attack of ‘benign’ TCH is a warning sign of a later SAH, even if an SAH has been excluded at the time of the TCH attack? This would require that a sudden enlargement of an aneurysm occurs and evokes sudden onset headache without causing a bleed. It is not known if such sudden enlargements occur and if they can be painful.
The results from the present and the other studies on TCH have a bearing on this question. Altogether 297 patients with TCH attacks and normal results, including at least CT scan of the brain and CSF examination, were followed-up for 1–7 years without any SAH morbidity. In the study by Wijdicks et al. (25) 71 patients were monitored for a mean of 3.3 years and no SAH occurred, although some patients had recurrent TCH attacks. Two of these patients had angiograms done but no aneurysms were found. In a study by Harling et al. (7) 14 non-SAH patients were followed for 18–30 months. Eight of these patients had angiograms, all with normal findings. Linn et al. (16) followed 93 patients with sudden headache without SAH for 1 year and none subsequently had SAH, stroke or sudden death. Markus followed 16 patients over 20 months. Our own study comprises 103 patients with benign TCH. The results from these studies thus provide strong support for the conclusion that angiography is not indicated in patients with non-SAH TCH (defined as TCH with exclusion of an SAH by CT and CSF examination), unless there are special reasons. One such reason could be if a patient is not examined until >10–14 days have passed after the attack, because at that time it is not possible to determine if the TCH was caused by a small SAH.
The question remains of how does one explain the frequent pre-emptive headache attacks experienced by so many SAH patients? It is probable that such an attack is in fact a small SAH. This idea is supported by the present results and by a case-control study (14) in which it was found that 13 of 30 patients with SAH had experienced an attack of sudden onset headache 1–8 weeks before the SAH was diagnosed. Seven of these patients had been to a doctor because of their headache attack but none had undergone CT or CSF analyses. In a later prospective study the same investigators found only two cases with such attacks in a material of 37 SAHs (16). It is probable that a protocol that requires exclusion of SAH in all patients with a first attack of sudden onset headache would save many individuals from a second more dangerous SAH.
Finally, does the demonstration by Dodick et al. (11) that some patients with TCH have diffuse multifocal segmental vasospasms indicate that some form of non-invasive angiography ought to be performed in this condition? We believe that unless there are indications from the symptoms and signs that there might be a disturbance in brain functions, an angiography is not necessary, because the excellent follow-up results of TCH patients show that the condition is spontaneously reversible and that it does not lead to brain lesions or brain dysfunction.
Footnotes
Acknowledgements
This study was supported by research grants from The County Council in Östergötland and the Swedish Migraine Society.