
Abstract
Background
To assess the prevalence of headache attributed to aeroplane travel (AH) in patients referred to Italian Headache Centres.
Material and method
869 consecutive patients visiting six Italian headache centres during a 6 month-period (October 2013 to March 2014) were enrolled in the survey. Among them, 136 (15.6%) had never flown and therefore were excluded from the study. The remaining 733 patients (f = 586, m = 147; age 39.1 ± 17.3) were asked about the occurrence of headache attacks during flight; those who answered the question positively filled in a detailed questionnaire that allowed the features of the attacks to be defined.
Results
Headache attacks during the flight was reported by 34/733 subjects; four presented attacks fulfilling ICHD-3 beta (1) criteria for migraine without aura and therefore were not further considered. The features of the remaining 30 (4.0%; m = 18, f = 12, age 36.4 ± 7.3) completely fulfilled the ICHD-3 beta criteria for AH. In more detail, the pain was unilateral (fronto-orbital: n = 23; fronto-parietal: n = 7; without side-shift: n = 25, with side-shift: n = 5), lasting up to 30 min in 29 subjects. All the patients reported the pain as very severe or unbearable and landing as the phase of travel in which the attack appeared. In four cases, a postictal, milder, dull headache could last up to 24 hours. Accompanying symptoms were present in eight cases (restlessness: n = 5; conjunctival injection and tearing: n = 2; restlessness + ipsilateral conjunctival injection and tearing: n = 1). The fear of experiencing further attacks negatively affected the propensity for future flights in 90.0% of subjects (n = 27). In all the patients, AH onset did not coincide with the first flight experience. Concomitant migraine without aura was diagnosed in 24, tension-type headache in four, migraine without aura + tension-type headache in two cases; none suffered from cluster headache. Five subjects reported AH on each flight, 20 in > 50% of flights, five occasionally. Despite the severe intensity of the pain, only one third of this sample spontaneously reverted to a pharmacological treatment; the most useful strategy combines a decongestant nasal spray plus the intake of a simple analgesic 30 min before the estimated attack. Spontaneous manoeuvres were applied by 18 patients (Valsalva-like: n = 12; compression: n = 2; both manoeuvres: n = 4), more often without significant improvement. These data confirm our previous finding on the clinical features of AH.
Conclusion
AH was found in 4.0% of a multicentre, large sample of patients with flight experiences. Although limited to a sample of patients followed in six Italian headache centres, to the best of our knowledge these are the first epidemiological data on AH gathered by direct interview. If properly investigated, AH seems to be a not infrequent condition, which, when diagnosed, could probably be prevented in many cases.
Keywords
Introduction
Headache attributed to aeroplane travel (AH) was included for the first time in the beta version of the third International Classification of Headache Disorders (ICHD-3 beta) (1), chapter 10, among other forms of headache attributed to disorder of homoeostasis. After the proposal of provisional diagnostic criteria (2) based on the attacks' stereotypical characteristics, which were clearly outlined by case series described to that point (2–5), several AH cases were described (6–9). Furthermore, the publication of the world's widest case series (10) definitively permitted drawing up of the current ICHD-3 beta diagnostic criteria.
Despite the fact of the unquestionable existence of this form of headache, data regarding the extension of the phenomenon are actually lacking. Therefore, we conducted a survey with the aim of evaluating the prevalence of AH in a sample of patients referring to six Italian headache centres.
Material and method
Six Headache Centres (Venice, Padua, Brescia, Turin, Pietra Ligure, Pavia) affiliated with the Italian Society for the Study of the Headaches were involved in the survey. The data of 869 consecutive patients referred for a first consultation to the outpatient headache centres over a 6 month period (October 2013 to March 2014) were collected during the normal interview; no one in the sample requested the visit for a headache with AH features. Patients who had never flown (n = 136; 15.6%) were excluded from the study. The remaining 733 patients (f = 586, m = 147; age 39.1 ± 17.3) were asked to refer to the occurrence of headache attack during flight. The features of each attack were accurately investigated according to the ICHD-3 beta diagnostic criteria. Patients provided oral informed consent.
Results
Headache attacks during flight were reported by 34/733 subjects; four of these presented attacks fulfilling ICHD-3 beta criteria for migraine without aura (MO) (1) and therefore were not further considered. The features of the remaining 30 completely fulfilled the ICHD-3 beta criteria for AH.
Other primary headaches
All the subjects were referred because of the coexistence of other primary headaches (MO: 24; TTH: 4; MO + TTH: 2). None spontaneously reported AH, as they considered it mainly an ear-nose-throat (ENT) problem.
Age at onset and gender distribution
The mean age at observation was 36.4 ± 9.5 years (range: 12–65); the first flight took place at a mean age of 16.7 ± 4.8 and headache onset occurred at 28.4 ± 5.9 years. In all the patients, AH onset did not coincide with the first flight experience. Gender distribution showed a preponderance of males (m = 18, f = 12). We are convinced that when answering such questions, people reported the data with good approximation, as both the events (first flight, first AH attack) represent easily remembered events in a life. Accordingly, despite the fact that the answer “I don't remember” was offered as a possible choice for those questions, this item was not indicated by the participants.
Upper respiratory tract disorders
None of the 30 subjects with AH referred to the presence of inflammatory sinus disorders when experienced AH attacks. As AH is a really striking experience, sufferers are able to carefully describe the entire episode and to deny the possible coexistence of other disease or symptoms, such as flu or sinusitis. Moreover, whereas this information should be carefully evaluated in the case of a single AH attack, it could be assumed as reliable when AH repeatedly recurs in the same subject, with the same features. Nine patients reported a previous self-diagnosis of acute sinusitis. Allergy was reported in five cases; no cases of bronchial asthma were found in the sample. Eleven subjects (36.6%) were smokers.
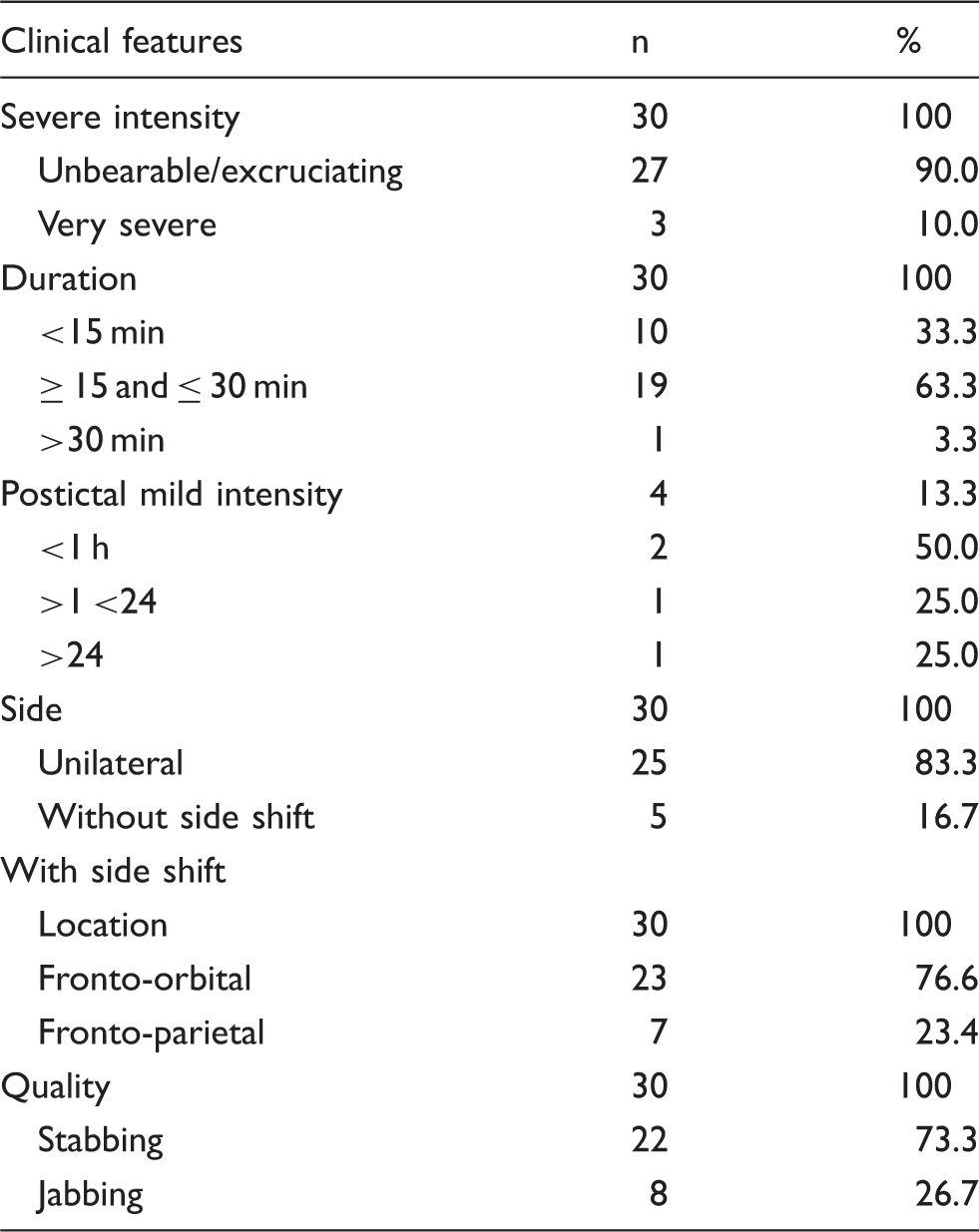
Clinical features of AH
Headache attributed to aeroplane travel: Clinical features (n = 30).
Timing
All the patients reported landing as the phase of the air travel in which AH attack occurred. In one subject, AH could also appear during take-off. None of the patients indicated a specific airport as a possible trigger factor for the onset of AH attack. Therefore, we inferred that the altitude of the airport does not represent a trigger factor for the occurrence of AH.
Duration
In almost all of the subjects (n = 29, 96.6%), the duration of the AH attack was up to 30 min (<15 min: n = 10; 15–30 min: n = 19); in just one patient the mean duration was 45 min. A second phase of a much milder headache, easily distinguished from the acute phase of AH, could persist for several hours in four patients (13.3%), lasting up to 24 hours in one case.
Intensity and quality of pain
The pain intensity was defined as very severe/unbearable by all the patients. On a visual severity scale (where 0 represents no pain at all and 10 represents unbearable pain) the mean score was 9.6. Furthermore, the quality of pain was defined as stabbing (n = 22, 73.3%) or jabbing (n = 8, 26.7%).
Side and location
The pain was unilateral in all cases (fronto-orbital: n = 23; fronto-parietal: n = 7). A strict unilaterality in subsequent flights was referred to by the majority of subjects (n = 25, 83.3%), while in five patients (16.7%) a side-shift of the same localization could occur. Among the four patients who reported a persistent milder headache for several hours after the acute phase, in three cases the pain became bilateral.
Consistency of attacks
Consistency of attacks and average number of flights per year (n = 30).

Patients 4 and 5 did not fly in the last year, due to the fear of a possible AH attack.
Accompanying symptoms
Accompanying symptoms (n = 8/30, 26.7%).

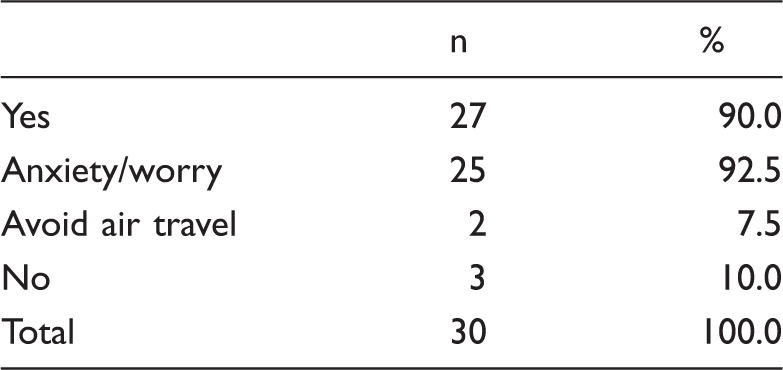
Emotional impact
Effect of headache attributed to aeroplane travel on attitude to flying (n = 30).
AH-like attack triggered by different situations
Headache attacks with the same features as AH but triggered by different situations were reported in six cases. In more detail, among the 13 subjects with experience of free/snorkelling or scuba diving, four (30.7%) reported the sudden onset of headache during the decompression phase of diving (scuba, n = 1, free/snorkelling, n = 3) at an average depth of 5 m. Moreover, two subjects experienced the same pain during rapid descent from altitude by car (average altitude 1850 m); one patient reported both of these situations as trigger factors. In all cases, the pain disappeared within 30 min respectively after the ascent or the fast descent were ended.
Spontaneous manoeuvres
Reported efficacy of the spontaneously performed manoeuvres (n = 18/30, 60.0%).

Pharmacological treatment
Drug efficacy (n = 10/30, 33.3%). A single patient could have consumed different kinds of drugs (more than one drug) in monotherapy or combination of drugs on subsequent flights. A single patient could have consumed different kinds of drugs (more than one drug) in monotherapy or combination of drugs on subsequent flights.

Discussion
In this multicentric study, the prevalence of AH in an adult outpatient population referred to headache centres for other primary headaches was assessed. Among the 733 consecutive patients enrolled, AH was found in 30 cases (4.0%). Despite the extremely severe intensity of the pain and the negative propensity for subsequent flights, none of the subjects spontaneously reported AH during the interview, as they attributed the pain to an ENT competence. This survey confirmed the previously reported and peculiar clinical features of AH (2,10–12), included in the ICHD-3 beta classification (1) and corroborated in the current version (13). Moreover, the presence of accompanying symptoms during AH attack in one fourth of the sample, which could mimic a cluster headache attack according to the ICHD criteria (13), is in line with recent observations (11). It stresses the importance of the onset of pain during aeroplane travel (criterion B of 10.1.2 Headache attributed to aeroplane travel) (13), which allows the differential diagnosis between AH and cluster headache along with other clinical features, among which was spontaneous remission shortly after landing.
Despite the severe intensity of the pain, only one third of this sample spontaneously reverted to a pharmacological treatment; the data on drug efficacy are based on the subjective experience of patients who noticed a reduction in the recurrence of AH attacks after the introduction of a self-made therapy. In those who reported an efficacy >50%, the most useful strategy combines a decongestant nasal spray plus the intake of a simple analgesic 30 min before the estimated attack. More frequently, people suffering from AH applied spontaneous manoeuvres in order to reduce the intensity of the pain, but with very poor results in terms of efficacy. Both the percentage of AH patients who revert to pharmacological treatment and spontaneous manoeuvres, and their respective referred efficacy, are in line with previous observations (10,11). The use and efficacy of triptans for treating AH attack have been previously reported (14,15) and are confirmed by three subjects in the present sample. Similarly to a previous report (15), a migrainous patient, who usually treats her attacks with frovatriptan and presents with AH in more than 75% of flights, spontaneously took the long-acting triptan before take-off and reported a >75% prevention of AH occurrence. Even if the reports on the use of triptans for AH appear to indicate an overall efficacy in treating the attack, further investigations are needed to confirm their real effectiveness and safety.
In a percentage of subjects, AH-like attacks were triggered by free/snorkelling or scuba diving (diving ascent headache, DAH) and rapid descent from high altitude (mountain descent headache, MDH). These situations were previously reported to be associated with AH, leading to the hypothesis of a common causal mechanism involving the imbalance between intrasinusal and external air pressure (11). The involvement of the trigeminovascular system, which could explain the efficacy of triptans in treating AH attacks, would be the result of the mechanical activation of the nociceptors of the ethmoidal artery, stimulated by the physical changes in the paranasal sinuses due to the modification of external pressure according to Boyle's law (10). Albeit an alternative pathogenetic hypothesis has been proposed (16) and the exact mechanisms are still not fully understood, the imbalance between intrasinusal and external air pressure appears to be the main condition, strengthened by the occurrence of similar headache attacks triggered by sudden modification of internal and external air pressure, such as in DAH and MDH.
Prior to this survey, an attempt to estimate the prevalence of AH was performed by using an online questionnaire, which was administrated through the Facebook pages of Scandinavian airlines; among the 254 subjects who answered, 21 (8.3%) satisfied the ICHD-3 beta criteria for AH. Moreover, a self-diagnosis of migraine was more frequently reported from AH than non-AH sufferers (17). This high prevalence could reasonably be attributed to a bias in the higher motivation of AH subjects in answering the online questionnaire. In the same study, MO was found to be the most common primary headache both in subjects reporting AH and in those unaffected by the condition. Whereas this result could be expected in an outpatient population referred to headache centres, since migraine is the most common cause of consultation among headache sufferers, it is surprising in a general population, in which tension-type headache is known to be more frequent. Indeed, in a large series of AH patients, in which the diagnosis of concomitant primary headaches was ascertained by a questionnaire based on the ICHD criteria, the more frequent concomitant primary headache was found to be TTH, reflecting the distribution found in the general population, despite the sample being gathered through spontaneous reports from AH sufferers (11).
An additional interesting observation is that, after the six-month observational period was ended and during the preparation of the present manuscript, some patients spontaneously started to refer to headache centres asking for help for their AH, perhaps indicating a growing awareness regarding this particular form of headache.
Conclusion
AH was found in 4.0% of a large multi-centre sample of patients with flight experiences. As previously reported, the possible coexistence of similar attacks, but triggered by different situations (the decompression phase of diving and rapid descent from altitude by car), has been confirmed in a portion of patients, suggesting the imbalance between intrasinusal and external pressure as a possible common pathogenesis. Although limited to a sample of patients followed in six Italian headache centres, to the best of our knowledge, these are the first epidemiological data on AH gathered by direct interview in an adult population. If properly investigated, AH seems to be a not infrequent condition, which could be probably be prevented in many cases.
Clinical implications
These are the first epidemiological data on headache attributed to aeroplane travel (AH) gathered by direct interview in an adult population referring to headache centres. AH was found in 4% of eligible patients (30/733), confirming its peculiar clinical features with particular regard to duration of the acute phase, unilaterality and intensity of the pain, mainly related to landing. Moreover, the negative propensity to take future flights has been confirmed. The possible coexistence of similar attacks, but triggered by different situations (decompression phase of diving and rapid descent from altitude by car), has been confirmed in a portion of patients, suggesting the imbalance between intrasinusal and external pressure as a possible common pathogenesis. AH seems to be a not-infrequent condition, which could be probably prevented in many cases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.