
Abstract
Background
Headache attributed to aeroplane travel (AH) is currently codified in Chapter 10.1.2 of the International Classification of Headache Disorders 3 beta (ICHD 3 beta). After our previous papers, the investigation was enlarged to 200 patients.
Material and methods
People affected by AH contacted us by mail and agreed to fill in a detailed anonymous questionnaire that allowed a thorough definition of the headache features.
Results
This extended case series allows us to confirm most of the clinical features of AH, reported in our previously published article, and to partially modify others. New results mainly regard the higher occurrence of accompanying symptoms and the presence of a long lasting mild headache phase, usually not exceeding 24 h, that follows the short lasting acute pain, the duration of which has been confirmed as less than 30 min. Moreover, headache attacks identical to those of AH are reported in a portion of patients, triggered by the ascent during free/snorkeling or scuba diving and rapid descent from high mountains.
Conclusion
The coexistence of AH with headache triggered by different environmental factors (ascent during free/scuba diving and descent from high mountains) indicates a common causal mechanism, that is, the imbalance between intrasinusal and external air pressure. We propose to classify them together, within Chapter 10 “Headache attributed to disorders of homoeostasis”, under a unique heading “Headache attributed to imbalance between intrasinusal and external air pressure”.
Keywords
Introduction
Headache attributed to aeroplane travel (AH) is currently codified in Chapter 10.1.2 of the ICHD 3 beta among other types of “headache attributed to disorders of homoeostasis” (1). After earlier observations (2,3), we described the first Italian case in 2007 (4). Since then, we have continued our research on this topic, which allowed definition of the peculiar features of AH in a series of 75 patients (5), contributing to attribute a nosological dignity to AH in the context of the current ICHD. The present article analyses AH features in an enlarged series of 200 patients. Furthermore, it investigates the features of headache attacks reported by two subgroups of AH patients, respectively during the fast descent from mountain altitude by car and the ascent during free/snorkeling or scuba diving.
Materials and methods
Due to the dissemination of our paper via the Internet, email messages were sent to us from people who reported headaches with the same features. Participants filled in a detailed anonymous questionnaire by mail (see Supplementary Material), which allowed a detailed investigation of AH features. Moreover, specific sections of the questionnaire permitted us to identify the concomitance of other forms of primary headache or the onset of headache attacks due to rapid descent from mountain altitude or rapid ascent during free/snorkeling or scuba diving. Of the 201 subjects who contacted us, 200 filled in the questionnaire. When needed, additional information was obtained either by email or by telephone. The present series includes the previous published 75 cases (5).
Results
Headache attributed to aeroplane travel
Age at onset
The patients’ mean age was 37.3 ± 10.9 years (range 8–63). Males were 58%, a percentage not statistically significant. The first flight experience and headache onset were reported at a mean age of 15.5 ± 8.6 and 29.1 ± 9.9 years, respectively. In the highest percentage of the cases (85.5%) AH did not occur during the first flight.
Upper respiratory tract disorders
A history of allergy was referred to by 37.5% of the sample (34 males and 41 females); in more detail, bronchial asthma was reported by 16 subjects (10 females and six males), while a previous sinus infection was indicated by 22.0% of patients (23 females and 21 males). Two male subjects had a recent occurrence of sinus infection. However, signs and symptoms of acute inflammatory sinus infection were consistently absent in all the subjects when AH attacks occurred. Almost a fifth of patients (18%) were smokers, with a slight female prevalence.
Coexistent primary headaches
Coexistent primary headaches in “Airplane headache” patients (n = 105/200, 52.5%).

Clinical features of AH
The characteristic features are as follows.
Timing
Onset of headache attributed to aeroplane travel in respect to flight timing.

First episode
In 29 patients (14.5%) AH onset occurred during the first flight (mean age: 20.1 ± 7.3 years; mean age at interview: 34.6 ± 10.4 years) (Table 2). In the remaining 171 cases, AH onset occurred at the age of 31.3 ± 10.9 years, with a mean interval of 17 years from the first flight, which was experienced at a mean age of 14.7 ± 8.0 years, their current average age at interview being 37.6 ± 11.0.
Intensity
Clinical features.

Duration
The severe pain phase typically did not go beyond 30 minutes (191 cases, 95.5%) and, more specifically (Table 3), it was shorter than 10 minutes in 12 patients (6.0%), and lasted 10 to 30 minutes in 179 cases (90.0%). In eight cases (4.0%), a severe pain persisted for more than 30 minutes up to a maximum of three hours (two cases). For one patient, the answer to this question was lacking.
Postictal, milder headache
In 55 subjects (27.5%) a postictal headache, easily recognisable as much milder, followed the acute phase of AH. In half of these cases (49.0%), it could persist several hours, lasting up to 24 h (3.6%) or 48 h (21.8%). In 25.6% of cases it disappeared within one hour.
Side and location
In the large majority of cases (176/200, 88.0%), the pain was strictly unilateral (Table 3). In 12%, the headache was bilateral or in the vertex, while one subject did not specify the side of the pain and two subjects did not specify the location. Among patients with unilateral pain, the headache persistently recurred on the same side throughout the attacks in 69.3% of cases, while in 25.0% a side shift was reported in following flights. Ten subjects (5.7%) reported a single AH attack.
The fronto-orbital region was more often involved (79.8%); strictly unilateral in 158 cases (right n = 53, left n = 47, side unspecified n = 8); unilateral with side shift in different attacks in 38 cases and bilateral in 12 cases. In 18 patients (9.1%) the headache, constantly unilateral in 17, was confined to the fronto-temporal region, (right n = 8, left n = 6, with side shift n = 3); in one case the pain was bilateral. The fronto-parietal region was involved in 10 cases (right n = 5, left n = 2, with side shift n = 3). Other pain locations, involving different areas (in particular, the occipital region and the vertex) were indicated by 12 subjects; nine of them reported the pain to be bilateral. Two patients did not specify the location.
Quality of pain
The headache (Table 3) was frequently defined as stabbing (n = 132, 66.0%). Other descriptions were jabbing (11.0%), pressing (9.0%), electric shock-like (7.5%), and pulsating (6.0%).
Accompanying symptoms
Accompanying symptoms, reported by 29.5% (59 patients) were: restlessness (n = 40, 20.0%), which was the most common; unilateral tearing (n = 28); conjunctival injection (n = 4); photophobia (n = 3), phonophobia (n = 2); nausea (n = 2). The combinations were: restlessness + tearing (n = 9); restlessness + tearing + conjunctival injection (n = 1); restlessness + phonophobia + photophobia (n = 1); restlessness + nausea (n = 1); restlessness + tearing + phonophobia + photophobia (n = 1); conjunctival injection + tearing (n = 3), phonophobia + photophobia (n = 1), conjunctival injection + photophobia (n = 1), conjunctival injection + phonophobia + photophobia (n = 1). No patient complained of vomiting, smell or perfume intolerance, ptosis, rhinorrhoea, nasal stuffiness, forehead sweating, miosis or aura. Anxiety was constantly present during the attacks.
Consistency of attacks
In 37/200 patients (18.5%) the same type of pain recurred constantly on landing after distinct flights; apart from one case, flight duration did not influence the AH occurrence. In two of these subjects the pain also started during take-off, and exclusively during take-off in one case. AH occurred in more than 50% of flights in 66/200 patients (33.0%), landing in 61, during both take-off and landing in two, during cruising in two and exclusively during take-off in one. AH occurred in less than 50% of flights in 37 subjects (18.5%): exclusively during landing in 34, also during take-off in two, and during the cruising phase in one. In 48 cases (24.0%), the attacks were occasional and unpredictable. Eleven (5.5%) patients experienced only one attack. One patient had suffered from two isolated attacks only in the last two flights, despite flying 6–8 times every year; when contacted, he was not able to provide further information.
Emotional impact
Effect of AH on attitude to flying.

Self-administered maneuvers
Reported efficacy of the spontaneously performed maneuvers (n = 103/200, 51.5%).
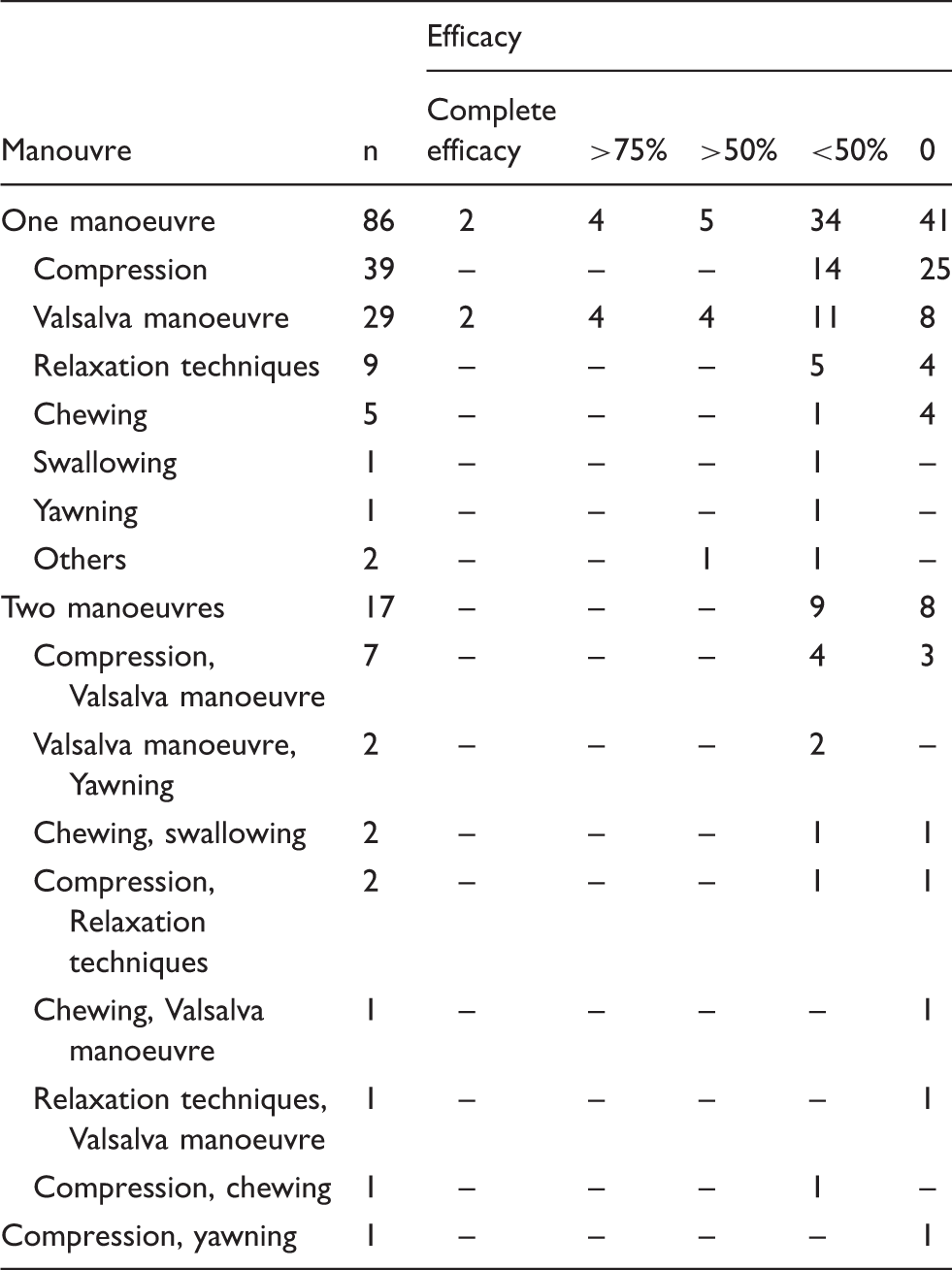
In descending rank, the spontaneously administered manoeuvres were (Table 4): compression on the pain site (n = 50; alone n = 39, in combination n = 11), Valsalva manoeuvre (n = 40; alone n = 29, in combination n = 11), relaxation techniques (n = 12; alone n = 9, in combination n = 3), chewing (n = 9; alone n = 5, in combination n = 4), yawning (n = 4; alone n = 1, in combination n = 3), swallowing (n = 3; alone n = 1, in combination n = 2), others (tractions of the lobes (n = 1), ear plugs (n = 1). The overall efficacy of these manoeuvres was minimal, apart from the Valsalva manoeuvre, with which 25% of patients (10/40) obtained a > 50% improvement: among them, four subjects achieved a relief of more than 75%, and two achieved a complete resolution of the AH attack.
Pharmacological treatment
Drugs’ efficacy (n = 78/200, 39.0%).

Free or scuba diving headache
Among subjects reporting diving experience (23.0%, 46/200), 45.6% (21/46) complained about a pain attack with characteristics that were indistinguishable from AH during the free/snorkelling or scuba diving ascent (free/snorkeling or scuba diving ascent headache) on at least one occasion (free/snorkeling diving, n = 14; scuba diving, n = 4; both, n = 3). In more detail, 14 subjects reported the onset of the attack during the ascent phase after free/snorkeling diving attaining the maximum depth of 5–8 m, and seven patients after scuba diving, with an average depth of 20 m. The pain began during or shortly after the ascent, attaining its apex in a few minutes and spontaneously disappearing within 30 min in all of the subjects. No airways disturbance was referred during diving. The pain occurred in > 30% of the dives in eight cases; one patient complained about a headache attack only on occasion; 12 patients did not specify the frequency.
Headache from rapid descent from altitude by car
Among the 120 subjects who were investigated for this, 20 (16.6%) reported headache attacks, with the same characteristics as AH, induced by the rapid descent from high mountain altitude (Mountain descent headache). Free/snorkeling or scuba diving ascent headache attacks were reported in five out of the six subjects who had diving experiences. It was not possible to determine precisely how many of the 120 subjects had experienced a rapid descent without suffering a headache attack. In all the cases, the headache began shortly after the rapid descent by car from a medium altitude of 1920 m (range 1800–2400), the apex of intensity having a development of a few minutes. All of them reported the end of the pain within 20 minutes from the fast way down. No airways disturbance was referred to during the travel. Five of them had experienced similar attacks also during the ascent from diving (free/snorkeling diving, n = 3; scuba diving, n = 1; both, n = 1). Moreover, the rapid descent in a skyscraper elevator triggered similar attacks in two cases.
Discussion
This extended case series corroborates most of our previous observations on AH features (5), allowing better characterisation of some of its aspects; and to identify AH-like attacks triggered by two different circumstances, the ascent after free/snorkeling or scuba diving (diving ascent headache) and rapid descent from a mountain (mountain descent headache).
Headache attributed to aeroplane travel
The main components of the clinical profile of AH are confirmed, with particular regard to duration of the acute phase, unilaterality and intensity of the pain, mainly related to landing and, less frequently, to take off. The prevalence of unilateral/anterior location and the rarity of vertex and posterior locations are in favor of the involvement of a frontal sinus. A postictal mild or moderate headache, following the acute severe phase and lasting up to 48 hours, was reported by about a quarter of patients. However, even in these patients the severe headache phase never exceeded 30 min in duration. Such a result indicates that a mild headache phase is present more frequently than previously reported by us (5), confirming the observation of a possible persistence of the pain longer than 30 min (6,7), but also highlighting a clear-cut difference in intensity between the severe, typically short-lasting, AH pain and the mild, long lasting headache that may follow. This finding is quite relevant, since the distinction between the acute severe and the postcritical mild phases avoids a possibly confounding aspect of AH duration in its differential diagnosis versus other forms of headache.
A coexistent primary headache was present in more than half of the cases, the most common being TTH and MO. In this perspective, also the occurrence of accompanying symptoms in the present case series is relevant in the differential diagnosis of AH versus MO: indeed, AH accompanying symptoms, reported by 29.5% of patients, were mostly represented by restlessness and lacrimation. The typical accompanying symptoms of MO were rare and represented by phonophobia, photophobia, and nausea, whereas vomiting and osmophobia were absent.
In respect to the differential diagnosis of AH versus CH, considering that the isolated presence of only one accompanying symptom, along with pain intensity and duration, would allow a diagnosis of CH (1), in more than a quarter of subjects with AH (58/200, 29 presenting restlessness alone, 18 vegetative symptoms without restlessness, 11 restlessness and vegetative symptoms) the clinical features of their attacks would formally fulfill the ICHD3 beta diagnostic criteria for CH. Therefore, in the differential diagnosis of AH versus CH, the relevance for the AH diagnosis of the criterion ICHD 3 beta 10.1.2 C, “Evidence of causation demonstrated by at least two of the following: 1. headache has developed exclusively during aeroplane travel; 2. either or both of the following: a) headache has worsened in temporal relation to ascent after take-off and/or descent prior to landing of the aeroplane, b) headache has spontaneously improved within 30 minutes after the ascent or descent of the aeroplane is completed” is critical.
The negative AH influence on the attitude to flying was notable. Most patients (80.0%) were concerned with the fright of incurring a further attack, and consequently the emotional impact of AH negatively predisposed them to future flights. Among them, about a quarter decided to fly only if strictly required or gave up flying. Moreover, during the acute phase of the attack, about a third asked for help. Considering the emotional impact of AH, passengers should be adequately addressed and informed about this severe headache, its non-harmful and self-limiting nature, and the means of potentially preventing it. A higher concentration of cortisol has been documented during a simulated flight in a group of anxious AH sufferers but not in the control group, raising the question of the possible role of anxiety in the pathogenesis of AH (8). Anxiety is not uncommon in flight passengers, but it appears to be independent from the risk of developing of AH, since otherwise it would be reasonable to expect that AH attacks would be much more widespread. On the contrary, the negative attitude to the flight referred to by AH sufferers is reported as a consequence of the fear of developing a further attack.
About half of AH patients performed one or more spontaneous self-administered manoeuvres attempting to obtain some relief, as previously reported in patients with primary headaches (9). In descending order, the most common were pressure on the pain site and the Valsalva manoeuvre. The overall efficacy appears unremarkable, apart from the benefit reported with the Valsalva manoeuvre by more than 70% of patients who used it; among them, more than one third reported a greater than 50% improvement. Although very limited, these results would possibly support the causative role in AH of an imbalance between intrasinusal and external air pressure.
An unexpected result concerns the resort to pharmacological treatment. Despite the unbearable intensity of the pain and the emotional impact that negatively predisposes for future flights, a pharmacologic approach is reported only by 39% of patients. NSAIDs and analgesics were most frequently used, being utilised by about 40% of these subjects, followed by nasal decongestant and polytherapy (mostly a combination of nasal decongestant and NSAIDs/analgesics). As a whole, these drugs are reported to prevent the attack in 1/3 of the cases, where the vast majority take the drugs about 30–60 minutes ahead of the estimated triggering phase of the air travel. Triptan use is referred to in two cases. In more detail, the sole patient who used the long acting triptan frovatriptan during a four-landing journey reported that AH occurred only when she took an NSAID alone instead of in association with frovatriptan (10). The sole patient who used sumatriptan reported a benefit of 50–75%. These results are in keeping with previous observations (11); however, any statement about triptans’ effectiveness needs to be further investigated. More in general, the real efficacy of the drug therapy has to be proven, as it was self-reported. Due to the unpredictability of the attack and the absence of a placebo control, the relatively best information comes from the anecdotal experience of the subjects who present AH on each flight and regularly use a medication; among them, the complete prevention of AH attacks is reported in 5/18: the scarcity of the sample does not allow a definitive conclusion.
The concomitant use of pharmacological therapy and self-administered manoeuvres, reported by one third of the patients, obtained relief that was not superior to pharmacological therapy alone.
Headache attributed to the rapid descent from high altitude
Headache is acknowledged as a potential complication of ascent to altitude. But, whereas high-altitude headache, related to hypoxia, is officially included in the ICHD-3beta (1), Chapter 10.1.1 “Headaches attributed to disorders of homoeostasis”, the fast descent from high altitude is not recognised as a potential cause of headache.
Mountain descent headache (MDH) case reports are scarce (12,13). Nevertheless, in our investigation, MDH occurred in almost a fifth of AH cases. Therefore, even though the exact recurrence of AH is unknown, it appears to be quite a frequent condition (14,15). Our preliminary, unpublished research on five Italian headache centres gives a figure of about 5% of AH patients among those with flying experience; hypothesising that around 20% of AH patients could virtually suffer from MDH too, this latter headache should not be uncommon (14,15). In MDH, beside the difference in level, the speed of the descent is the causal factor, inducing a headache attack in predisposed subjects only when it occurs rapidly. In this perspective, unlike in AH, MDH could not necessarily require drug treatment since just reducing the speed of descent should be sufficient to avoid the attack. The consistency of MDH attacks on distinct descent from altitude was not investigated.
Headache attributed to the ascent after free/snorkeling or scuba diving
Headache is acknowledged to be a potential complication of diving. But, whereas diving headache, related to hypercapnia occurring when the dive goes below 10 m, is officially inserted in the ICHD-3 beta (1), Chapter 10.1.3 “Headaches attributed to disorders of homoeostasis”, headache related to the ascent after diving, possibly due to causal conditions other than hypercapnia, is not considered. Only anecdotal case reports of headache related to free/snorkeling or scuba diving ascent (DAH) are described in the literature. In our series, DAH is reported by about 46% of the AH subjects who had experienced such a condition, and therefore DAH should not occur infrequently (14). From the therapeutic perspective, should the anecdotal report of triptans’ efficacy on AH (10) be confirmed, in order to prevent DAH (which shares with AH the imbalance between external and intrasinusal air pressure as the causative mechanism), a long lasting triptan could potentially be preferable, since it could warrant an extended protection during repeated dives.
Conclusion
This extended case series allows us to re-affirm the clinical features of AH (5). New results regard mainly the higher occurrence of accompanying symptoms and of a long lasting mild headache phase following the short lasting acute pain, whose duration has been confirmed as inferior to 30 min.
AH-like attacks triggered by two different circumstances, the ascent after free/snorkeling or scuba diving and rapid descent from a mountain had been reported previously only as anecdotal observations (12,13,21). In this paper, they are described in detail.
Although the pathophysiology of AH remains speculative (5–8,13–26), its principal mechanism appears to be an imbalance between the pressure in the sinuses and the environmental pressure modifications occurring during aeroplane travel, mostly during landing and take off (5). The occurrence of headache attacks having the same clinical features, in three distinct conditions of rapid external pressure variations (aeroplane travel, fast descent from a mountain, free/snorkeling or scuba diving ascent), strengthen the hypothesis that a common causative mechanism, that is, the imbalance of intrasinusal air pressure vs the external air pressure, is shared by these conditions. However, the relation between AH, MDH and DAH and the possibility that the presence of one could predispose to suffer the other forms could not be established from this case series and needs further studies.
In conclusion, attacks featuring peculiar yet identical characteristics prompted by these distinct situations, a) landing or take off by airplane, b) descending from a mountain by car, and c) free/snorkeling or scuba diving ascent, would support the recognition of these three forms as the common clinical presentation of the same causative factor in different environmental situations.
Therefore, we confirm the proposal, already advanced (13), to classify them together, within the Chapter 10 “Headache attributed to disorders of homoeostasis” under a unique headline “Headache attributed to imbalance between intrasinusal and external air pressure”, with the following sub-types:
Headache attributed to aeroplane travel (AH) Headache attributed to fast descent from mountain (MDH) Headache attributed to free/snorkeling or scuba diving ascent (DAH).
Key findings
This extended case series confirms most of the clinical features of AH previously reported by us, with particular regard to duration of the acute phase, unilaterality and intensity of the pain, mainly related to landing and, less frequently, to take off. New observations mainly relate to the higher occurrence of accompanying symptoms and the possible presence of a long lasting, mild headache, usually not exceeding 24 h, that follows the short lasting acute pain, whose duration has been confirmed as inferior to 30 min. About a fifth of AH subjects decides to fly only if strictly necessary or gives up flying, 80% fly with fear. Considering the negative emotional impact of AH, passengers should be appropriately addressed and informed about this severe headache, on its non-harmful and self-limiting nature and on the means of potentially preventing it. Subgroups of AH subjects refer to the occurrence of headache attacks with similar features to AH during rapid descent from a mountain and/or during free/snorkeling or scuba diving ascent. The first non-anecdotal description of these two types of headache is given. Headaches occurring during a rapid descent from a mountain, or during free/snorkeling or scuba diving ascent appear to share with AH the same causative factor, that is, the imbalance of intrasinusal air pressure versus the external air pressure. Therefore, we propose to classify them together, within Chapter 10 “Headache attributed to disorders of homoeostasis” under an unique headline “Headache attributed to imbalance between intrasinusal and external air pressure”.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.