
Abstract
Background/objective
Headache in pupils is underestimated and has a negative impact on learning and life. The aim of this study was to investigate headache prevalence and its collateral effects, in pupils of different ages and school types in a German city.
Methods
Anonymized questionnaires were distributed to 5419 pupils attending primary and secondary schools. Demographics, headache frequency, analgesic use, school absence and, for secondary school children, data on lifestyle were collected.
Results
The questionnaire was returned by 2706 children (49%), 1362 (50.3%) girls, 1344 (49.7%) boys. Of these, 36.6% indicated a frequency of 1, and 31.5% a frequency of ≥ 2 headache days per month within the last 3 months. Headache prevalence increased with school grade, age and secondary school type: 63.6%, 67.2% and 79.5% for primary school children, pupils attending 8-year and pupils attending 6-year secondary schools, respectively. With secondary school level I certificates, pupils are prepared for general professional training in 6 years. Secondary school level II results, after 8 years of training, in university entrance level II certificates, which are the precondition for university studies. Girls reported significantly more headache than boys (73% vs. 63.1%). A significant relationship has been observed between headache frequency and school absence and between headache intensity and headache frequency. Of pupils with headache at least twice a month, 48.1% reported analgesic intake. Ibuprofen (49.1%) and paracetamol (32.8%) were the most frequently used analgesics. Of those pupils with headache ≥ 2 days/month, 68.3% did not have a specific headache diagnosis. Concomitant diseases and regular drug intake, analgesic intake for another reason than headache, caffeine consumption and lack of participation in sports were positively correlated with headache.
Conclusions
The majority of pupils suffer from headache at least once a month. Since frequent headache results in educational and social limitations, pupils at risk should be identified and referred to headache education programs. Efforts are needed to improve the management of juvenile headache patients.
Introduction
Headache is the most frequent type of pain experienced in children and adolescents (1). A review of 50 American, European, Australian and Asian population-based studies performed between 1990 and 2007 estimated the prevalence of headache in 5- to 20-year-old pupils as 58.4% (2). Analysis of data gathered in Germany has demonstrated a 3-month headache prevalence of 69.4% (boys 59.5%, girls 78.9%), in those aged 12 to 15 years (3). In northern Europe, consecutive studies have assessed headache prevalence within the same community, longitudinally across time (4–7). These studies found that headache prevalence in school children has increased in the last 10 to 30 years. Given that genetic factors within this community can be considered stable, non-genetic factors can be adduced to explain earlier onset and more frequent headaches (8). Several known risk factors for headache include caffeine or alcohol ingestion, smoking and physical inactivity (9). Other risk factors include stress at school (10), emotional stress related to family conflicts and all forms of abuse (11).
Studies from different geographical locations show varying headache prevalence in school children.. For example, the prevalence of headache in children aged 7–14 years is 25.5% in central India (12). In Turkey, 47.5% of students aged 7–17 have experienced headache (13). In Japan, a school-based study of children aged 6–15 years found that 49.4% of students experienced headaches (14). Besides differences in methodology and study population, all studies show headache prevalence in a substantial part of the pupils.
The aim of this study was to determine the prevalence of headache over a 3-month period, in schoolchildren of different ages and school types, in a city with about 550,000 inhabitants (Dresden, Saxony, Germany). We anticipate that such data should help to increase awareness of headaches as a relevant health problem. Given the current lack of standardized international guidelines and availability of therapy programs, in addition to the significant impact of headache on quality of life, we believe that our results will show that this condition requires further attention from social and medical communities.
Methods
Design and patient population
The present study was designed as a school-based, cross-sectional study. It was conducted between March 2015 and March 2016 in 14 state schools in the city of Dresden, Saxony, Germany. The study protocol was approved by the local Ethics Board of the Faculty of Medicine, Technical University Dresden (EK 25012015). Detailed information about the study was given to all participants, and those who consented to inclusion were those who voluntarily completed the anonymous study questionnaire. All aspects of the study were performed in accordance with the Declaration of Helsinki. Among the participating schools were seven 4-year primary schools, three 8-year secondary schools (with educational achievement of university entrance level II certificates) and four 6-year secondary schools (achieving secondary school level I certificates). Schools within a radius of 10 km around our medical school were selected. In doing so, we spanned a wide area of the city including areas with diverse socioeconomic backgrounds. A correction for socioeconomic factors was not required at school level since socioeconomic differences are inherent to the school system in Germany. It has been shown before that socioeconomic factors at 6-year secondary schools are less favorable than at 8-year secondary schools (15). Accordingly, the questionnaire was distributed to 1969 elementary school children, 2060 students of 8-year secondary schools and 1390 students of 6-year secondary schools. In total, 5419 questionnaires were distributed to pupils from 7 to 19 years of age. All completed questionnaires were included in the analysis.
Questionnaire
The study questionnaire anonymously captured sociodemographic data, as well as information on occurrence, frequency, features, accompanying factors, effects and intensity of headaches. In addition, lifestyle factors were ascertained in secondary school students. Elementary school aged children were given a one-page questionnaire, including the Faces Pain Scale – Revised (FPS-R) to measure headache-related pain intensity ((16), Supplemental Figure 1). Pupils of secondary schools filled in a two-page questionnaire. With the exception of pain intensity assessment (which used a numeric analogue scale as opposed to the FPS), all items on page 1 were identical to the elementary pupil questionnaire. The FPS is a six-step scale for self assessment of pain intensities for children aged 4–12 years (16). In our study we used it to measure headache intensities in participating elementary school children. The numerical rating scale (NRS) is widely used to self-assess pain in different ages. In our study we used it to measure headache intensities in participating secondary school pupils. The NRS usually consists of 11 steps between 0 and 10. Here we modified the NRS to six steps between 0 and 10, by using the following steps: 0, 2, 4, 6, 8, 10. In this way, NRS values could be more easily compared with the six steps of FPS. Page 2 for secondary school students included additional items concerning lifestyle factors. The pupils had one week to fill in the questionnaires (Supplemental Figure 2). Each of the questionnaires was given with a short instructional letter that says why the study is being done: To get information on how many pupils suffer from headache, and that the questionnaire should be filled in at home within 1 week and returned to the class teacher. For elementary school children it is indicated that the questions should be answered together with a parent.
Statistical procedures and data analysis
The association between headache prevalence and single questionnaire items was assessed using the χ2 test. The effects of gender, age, comorbidities, and lifestyle factors on headache prevalence within the last 3 months were analyzed using binary logistic regression. For this analysis, only questionnaire items that were available for all secondary school pupils were used, namely age, sex, type of school, housing situation, sports, body mass index, smoking, caffeine or alcohol consumption, use of electronic devices such as smartphone, TV, or PC, positive family history of headaches, comorbidities, and frequent analgesics or medication intake. As a result, potential headache predictors in secondary school children were established. The data analysis was performed using SPSS vs. 22 (SPSS Inc., Chicago, Illinois). For hypothesis testing, p-values (two-tailed) less than 0.05 were considered statistically significant. In cases of multiple testing, we implemented Bonferroni corrections of the p-limit of 0.05.
Results
Study sample
A total of 2706 pupils from elementary, 6- and 8-year secondary schools returned the questionnaire. This is in keeping with an overall response rate of 49%. More specifically, 1254 elementary schoolchildren, 896 8-year secondary and 556 6-year secondary school pupils, corresponding to a response rate of 63.7%, 43.5% and 40.0% respectively, completed the questionnaires. The gender ratio was equally distributed, with 1362 girls (50.3%) and 1344 (49.7%) boys responding. This gender ratio was maintained irrespective of school type (for details see supplemental Figures 3, 4, and supplemental Table 1). On average, elementary school pupils were 8.3 years old (median 8 years, range 6–12 years), 8-year secondary school pupils were 13.9 years old (median 14 years, range 10–19 years) and 6-year secondary school pupils were 13.6 years old (median 14 years, range 10–17 years, supplemental Figure 4). The majority of students (73.3%) lived with both of their parents, whilst 23.8% lived with only one parent (90.2% of whom lived with their mother). Of the remaining children and adolescents, 1.9% lived alternately with one parent and the other 1% lived with grandparents, in a youth welfare housing group, or alone.
Headache prevalence
The presence of headache within the last 3 months was used to calculate overall prevalence. Of all 2706 participants, 31.9% denied any form of headache. However, more than two thirds (68.1%) of students reported headaches on a regular basis: 36.6% of the total reported headache one day a month and 31.5% of the total reported ≥ 2 days of headache per month (Figure 1(a)). Of pupils with ≥ 2 days’ headache per month, the headache frequency varied as follows: 55.5% ≥ 2 days and < 5 days; 27% ≥ 5 days and < 10 days; 10.5% ≥ 10 days and < 15 days; 7% ≥ 15 days per month.
Headache prevalence in pupils. (a) Headache prevalence, all pupils; (b) headache prevalence in pupils of different gender; (c) headache prevalence in pupils of different class level; (d) headache prevalence in pupils of different school types.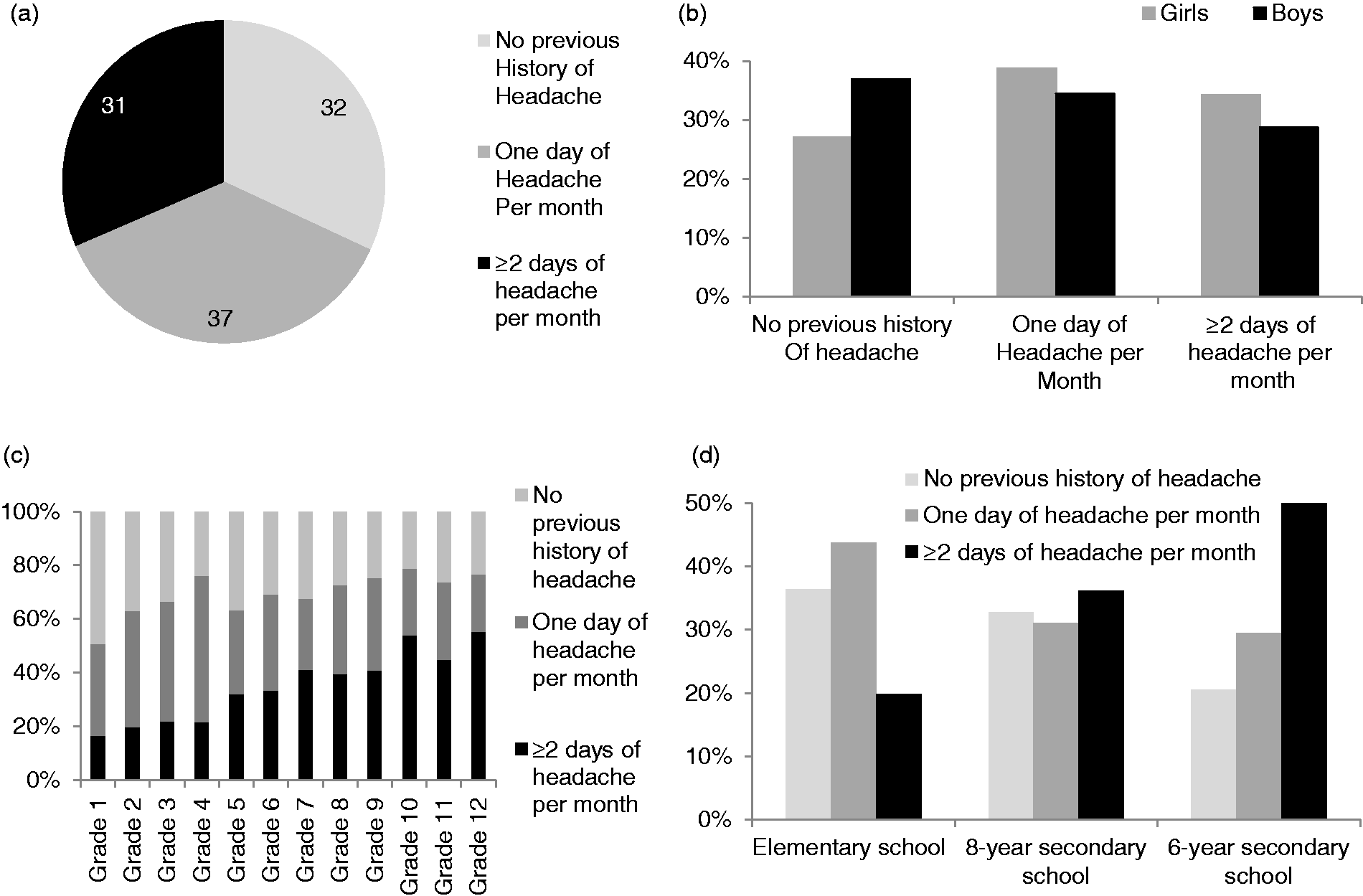
For prevalence calculations, categorial answers (never, rarely – 1 day per month, or frequently ≥ 2 days per month) have been used. Numerical values for headache days per month were obtained as an internal control. Of the pupils who reported one headache day per month, 98.3% classified themselves correctly as “rarely headache – 1 day per month”. All of the pupils (100%) with 12 headache days per month or more classified themselves correctly as “more frequent headache ≥2 days per month”. Of pupils with ≥3 to <12 headache days per month, 85% classified themselves correctly as “more frequent headache ≥2 days per month”. The group of pupils with two headache days per month showed the lowest rate of consistency: Only 60% of those who indicated two headache days per month classified themselves as “more frequent headache ≥2 days per month”. The other 40% categorized themselves in “rarely headache – 1 day per month”. Taken together, the self-classification of pupils in headache categories showed a high degree of conformance with numerical data. As was expected, girls (73%) experienced more headaches than boys (63.1%). Of those reporting headache, girls experienced ≥2 episodes per month more commonly than boys (34.2% and 28.7% respectively, Figure 1(b)). This difference was statistically significant (p < 0.001). Headache prevalence in all schoolchildren increased with class level and age (Figure 1(c)).
In total, 36.4% of elementary school pupils, 32.8% of 8-year secondary school pupils and 20.5% of 6-year secondary school pupils did not report headaches. Accordingly, 63.6% of pupils in elementary schools, 67.2% in 8-year secondary schools and 79.5% in 6-year secondary schools experienced headaches. With regards to headache frequency, a statistically significant difference in prevalence between school types was found. Headache for ≥ 2 days per month was reported by 19.9% of elementary school, 36.2% of 8-year secondary school and 50% of 6-year secondary school students (Figure 1(d)). This difference was significant (p < 0.001).
Headache prevalence in pupils with different housing situations.

Headache: Duration, intensity, accompanying factors
Of those pupils with headache, duration was as follows: 5% < 6 months; 5% 6 months to 1 year; 26.9% 1–3 years; 17.6% 3–5 years; 14.7% 5–8 years and 3.3.% 8–12 years (Figure 2(a)). A significant relationship between headache duration and headache frequency was not found.
Burden of headache, analgesics and doctor visits. (a) Time lived with headache; (b) individual burden of headache; (c) analgesic intake frequency; (d) doctor visits.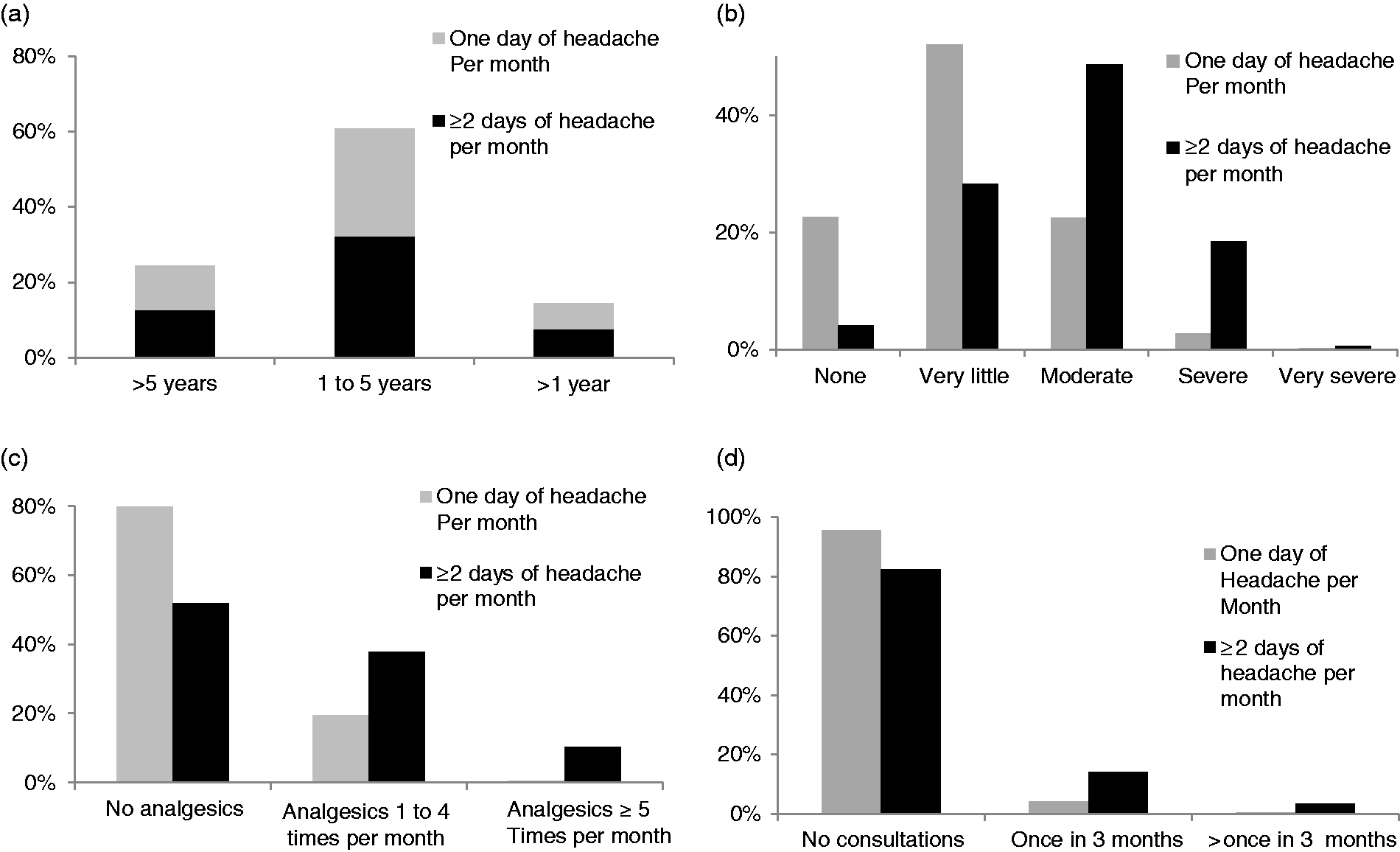
Headache and school absence within the last 3 months.

Headache: Medication and referral
Analgesics or homoeopathic mixtures for headache relief were used by 1186 pupils. In episodes with acute headache, ibuprofen (49.1%) and paracetamol (32.8%) were the most commonly used analgesics. Of students reporting headaches, 16% used other medications, for example homeopathic preparations or acetyl-salicylic acid. Only eight of them, five females and three males, used triptans. For detailed information see supplemental Table 2.
Almost 82% of children reported using analgesics when their pain was moderate to severe (6–10 points on FPS or NAS). There was no difference between those who experienced headache once a month or ≥2 days/month.
We found a significant correlation between frequency of headache and frequency of analgesic intake (p < 0.001, Figure 2(c)).
In the group with monthly headache, 19.6% of the pupils reported analgesic intake once a month, whilst 79.8% denied analgesic intake. In the group with headache at least twice a month, 48.1% of the pupils reported regular analgesic intake, while 51.9% denied analgesic intake for headaches in the last three months. Of those who reported analgesic intake, 37.9% used these medications once a month and 10.2% for at least five days a month.
Details for pupils who reported analgesic intake at least five days a month and patients with analgesic intake for other pain are shown in supplemental Table 3.
In total, 60 pupils reported ≥15 headache days in one month as the IHC criterion of chronic headache. Of these 60 pupils, 37 reported either analgesic intake ≥5 days a month, analgesic intake for other pain, or both. The remaining 23 of these 60 pupils reported neither. At this point it is not possible to differentiate whether analgesic overuse headache or another chronic headache is prevalent. Nevertheless, the group with ≥15 headache days in one month and analgesic intake ≥5 days a month or analgesic intake for other pain or both is suspected to include patients with analgesic overuse headache. We found a significant positive correlation between the frequency of headaches (≥2 days/month) and doctor visits per month (p = 0.001, Figure 2(d)). Of children with ≥2 days headache per month, 14.1% visited the doctor once and 3.5% visited several times in the last 3 months preceding participation in our study. In those with only monthly headaches, this was true in 4.2% and 0.3% of pupils, respectively. In 89% of all pupils with headache once per month, and 68.3% of all pupils with headache ≥2 days/month, a specific diagnosis of headache had not been made. Among pupils with headache ≥2 days/month, 14.9% had been diagnosed with migraine, 8% with tension type headache, and 8.8% with “other” headache types.
Children with higher headache frequency presented more often with a specific headache diagnosis compared with those with less frequent headache (p = 0.001).
Factors associated with headache and model for headache prevalence
Variables included in a binary logistic regression model for headache in pupils.

Univariate analysis of potential predictive factors for headache prevalence.

Classification of headache prevalence according to the model.

Positive family history of headache raised the frequency of headaches threefold compared to pupils with no such family history. The same applied for concomitant organic diseases, which increased the association with headache by 2.8 times. The largest effect on headache was analgesic intake for other diseases. This increased headache prevalence by 4 times. Regular medication intake (not limited to analgesics) more than doubled the frequency of headaches.
Discussion
Our results indicate that headache is a common source of pain and school absence in children and adolescents in an urban environment in Germany. Furthermore, we found that secondary school type significantly affects the likelihood of frequent headache. Based on potential risk factors for headache, a model was developed. In secondary school students, 91.6% of those with headache were correctly predicted using this model. Overall, for those with or without headache, 77.2% of students were correctly predicted.
Headache prevalence
This school-based study shows an overall 3-month headache prevalence of 68.1% in pupils aged 6–19 years. This confirms recent results demonstrated by a Germany-wide investigation of headache in schoolchildren, where 60 % of participants were affected (18). Further German data from 2005 describe a 3-month prevalence of headache, in adolescents aged 12–15 years, of 69.4% (3). A 2007 German investigation in children aged 7–14 years demonstrated a 6-month headache prevalence of 53.2% (19). However, this prevalence rate reflects the relatively young age of children investigated in this cohort. All of these studies describe increasing headache frequency with age. Our results clearly show that headache frequency increases between school grade 1 and grade 10 or 12. We also saw a clear difference in headache prevalence according to school type. Elementary school children reported the lowest headache frequency, in keeping with the rarity of headache at younger ages. At secondary school age, the type of school attended significantly affected headache prevalence. In pupils who attended 6-year secondary schools, a significantly higher percentage reported headache than in 8-year secondary schools. Furthermore, frequent headache (≥2 headache days/month) was more common in 6-year than 8-year secondary schools (50% versus 36.9% respectively). In Germany, the type of school attended often reflects the educational level and socioeconomic status of the child or adolescent’s family. In general, those from higher socioeconomic backgrounds attend 8-year schools. Furthermore, school type has been linked to general health, quality of life and health-related school absence (15). Accordingly, Heilmann et al. found in their study of 5790 German grade 6 pupils that those who attend 6-year secondary schools demonstrate poorer general health, reduced quality of life and more school absence than those who attend an 8-year secondary school. These findings are in keeping with our results, where students attending 6-year secondary schools reported headache more often than those attending 8-year schools (15).
In addition, we found higher headache prevalence in children and adolescents who lived with only one parent, or who lived alternately between parents. This adds to the impact of psychosocial factors on headache aetiology in children and adolescents. These findings support the published risk factors for recurrent headache, including dysfunctional families and individual stress in children (20–22).
Beside social criteria, our study points to the importance of biological factors: Female pupils report headache significantly more often than their male counterparts. According to the headache model introduced in this study, a positive family history of headache increases the likelihood of juvenile headache threefold. These data add to the existing observations concerning gender differences and genetic factors in primary headache (3,23–25).
Headache: Characteristics and impact
More than one third of pupils with headache reported a duration of greater than 3 years and 3.3% of pupils reported headaches for more than 8 years. The mean average age of all study participants was 11 years. These results appear to show that headache disorders manifest earlier in children and adolescents today than in the past (8).
We demonstrated no significant correlation between the duration of headache and frequency of headache. These results are in agreement with data gathered from pediatric migraine patients: Female patients present with a later onset of migraine and an overall higher burden of disease (24).
In this study, a significant positive correlation between frequent headaches and high headache-related pain intensity was found. A higher incidence of back and/or abdominal pain has been shown previously in children with headache compared with those without (19). Furthermore, a 2002 Swedish study found that two-thirds of adolescents with frequent headache reported at least one other area of bodily pain (26). These findings indicate higher pain sensitivity in children and adolescents with frequent headache. As mentioned, we found a significant correlation between high pain intensity and frequent headache.
School absence due to headache, particularly as a result of migraine, is well documented but usually underestimated (26). Up to one third of pupils with headache miss school days due to migraine. We demonstrated a clear link between headache frequency and school absence. A recent study from Norway found that, on average, nine school days were lost each year in adolescents with headaches (27). The psychosocial consequences of frequent headache due to absence from school or leisure activities can result in additional behavioral disturbances and isolation from peers. This can further impact education, and a correlation between frequent headache and academic underperformance has been shown (28). In line with this, reduced academic performance has also been found in university students suffering from frequent headache (29). Frequent headache also appears to affect quality of life. In our study, two thirds of pupils with ≥2 days of headache/month assessed their burden of headache-related disease as moderate to severe. Other studies have shown lower quality of life and underestimated socioeconomic burden in children and adolescents with headache (28,30).
Headache: Medication and doctor referrals
In our study, more than four out of five pupils who used analgesics for acute headache relied on ibuprofen or paracetamol. A recent Cochrane review of acute pediatric headache in migraine found some RCT-based evidence for ibuprofen but none for paracetamol (31).
Results from Italian tertiary headache centers have shown high percentages of triptan use in acute paediatric and adolescent migraine headache (32). This is in contrast to our study, where only 0.8% of pupils used triptans for acute migraine. This may be due to prescription practices in Germany, where triptans are only given when migraine is diagnosed. In our study, we found that only 15% of children with ≥2 headache days/month were diagnosed with migraine. Furthermore, almost 77% of those students with frequent headaches did not have a formal diagnosis. Nevertheless, we found a significant association between analgesic intake frequency and headache frequency.
Model for headache prevalence
Our model correctly identified >90% of students with headache. Overall, we hope that our model can help to identify those pupils who are at risk of frequent headache. Use of such a model poses no harm to children who are incorrectly identified as “at risk”. Therefore, the positive and negative predictive value of this model is useful. In addition, the single model variables highlight risk factors that need to be addressed in the treatment of students with headache.
Strengths and limitations
The use of voluntary questionnaires without supplementary diagnostic interviews in those reporting headache may potentially bias our results.
The aim of our study was to investigate the overall prevalence of headaches in pupils of different ages and school types. Therefore, in our questionnaire we did not differentiate common primary headache forms. To deepen our analysis, however, we asked which symptoms and lifestyle factors are associated with headache.
The questionnaires did not undergo a formal validation procedure. Questions have been developed by MR, RS and GG. The first preliminary versions of the questionnaires were distributed to colleagues, friends and neighbors with school pupils in their household to test for comprehensibility. The questionnaires were modified according to their comments and used in the paediatric headache clinic for collection of headache-related data. The reliability and validity of the questionnaires have not been tested. FPS and NRS, as components of the questionnaires, are very reliable and validated tools. The questionnaires have been in use in the paediatric headache clinic for >2 years. Comparison of data from the patient’s medical history, obtained in a doctor’s interview during the ambulant visit and data collected using the questionnaires show high consistency. This suggests validity without having set out an extra study for it. Nevertheless, there are limitations. For instance, there is no 100% accordance between the number of headache days per month provided by the pupils and the self-assessed categories of “rarely headache – 1 day per month” and “more frequent headache ≥2 days per month”. Furthermore, in the questionnaire for secondary school pupils the answer categories for lifestyle factors; that is, “Do you smoke cigarettes?” were incomplete since available answer options were only a) no, b) 1–2 times per week, and c) daily. Accordingly, pupils who smoke more than two times a week but not daily may have not been captured.
Briefly, an overall response rate of 49% meant that 51% of pupils did not return the questionnaire. Hence, the risk of bias exists. We did not send reminders to the pupils. Since the questionnaires were anonymous, we did not perform non-responder analyses. The questionnaires had to be completed at home and were collected at school 1 week after distribution. Consent was given by returning the questionnaires. All pupils were asked to fill in the questionnaire at home with one parent, albeit we could not control whether this was the case. The return rate for elementary school pupils was higher, being 63.7%. The overall headache prevalence data in our study is consistent with that of a recent Germany-wide investigation, which reported the frequency of headache in >40,000 pupils (18).
The implementation objectivity of the questionnaire should be guaranteed if pupils follow the instructions, which were given in a short letter attached to each questionnaire. The instructions indicated the purpose of the study (to get information on how many pupils suffer from headache) and specified that the questionnaire should be filled in at home and returned within one week to the class teacher. In the questionnaire for elementary school children, it was further indicated that the questions should be answered together with one parent. Lack of compliance with these instructions might have reduced objectivity. The cross-sectional methodology we used provided an overview of the headache prevalence at a given time point but it did allow conclusions to be drawn about the development of headache in pupils.
Clinical implications
In this study, we have shown that the majority of pupils have experienced headache and that approximately one third suffer from frequent headache. This highlights the need for new diagnostic and therapeutic approaches for children and adolescents with frequent headache.
Public health implications
Given the high prevalence of headache demonstrated in our study, public health education and preventive measures should be addressed. Continuing work with respect to headache in schoolchildren should address potential impact on future life, including career.
Conclusions
Our study demonstrates the existence of an unmet need for specific therapy programs for pupils with recurrent headaches in Germany and other industrialised countries. As concepts in technology, education and social structures have changed, school age children present with evolving health conditions. Among those, frequent headache plays a role in affecting wellbeing, education and social integration.
Public health relevance
The impact of headache on daily life and education in students should be reconsidered at the societal level. Public health education regarding headache in children and adolescents needs to be improved. Nonpharmacological methods for prevention of frequent headache in pupils should be implemented in school training.
Supplemental Material
Supplemental Material1 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material1 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material2 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material2 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material3 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material3 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material4 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material4 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material5 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material5 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material6 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material6 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Supplemental Material
Supplemental Material7 - Supplemental material for The prevalence of headache in German pupils of different ages and school types
Supplemental material, Supplemental Material7 for The prevalence of headache in German pupils of different ages and school types by Vera Nieswand, Matthias Richter, Reinhard Berner, Maja von der Hagen, Anna Klimova, Ingo Roeder, Thea Koch, Rainer Sabatowski and Gudrun Gossrau in Cephalalgia
Footnotes
Author contributions
GG, MR and RS: Study concept and design; VN, MR: Acquisition of data; VN, AK, GG: Analysis and interpretation of data; VN, MR, GG, RB, TK, MvH, AK, RS: Drafting and critical revision of the manuscript. All authors have read and agreed to the final version of the manuscript.
Acknowledgements
We thank the participants of this investigation. Furthermore, we would like to thank the directors and involved teachers of participating schools and the supervisory school authority in Dresden, Germany.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.