
Abstract
Background
The current study was designed to assess the effect of supplementation with a 14-strain probiotic mixture on episodic and chronic migraine characteristics.
Methods
Forty episodic and 39 chronic migraine patients who completed this randomized double-blind controlled trial received two capsules of multispecies probiotic or placebo. The migraine severity was assessed by visual analog scale (VAS). The number of abortive drugs consumed, migraine days, frequency and duration of attacks were recorded on paper-based headache diaries. Serum tumor necrosis factor alpha (TNF-α) and C- reactive protein (CRP) levels were measured at baseline and the end of the intervention.
Results
After a 10-week intervention, among episodic migraineurs the mean frequency of migraine attacks significantly reduced in the probiotic group compare to the placebo group (mean change: −2.64 vs. 0.06; respectively, p < 0.001). A significant reduction was also evident in the migraine severity (mean decrease: −2.14 in the probiotic group and 0.11 in the placebo group; p < 0.001). Episodic migraineurs who received the probiotic also showed significant reduction in abortive drug usage per week (mean change: −0.72; p < 0.001) compare to baseline, while there was no significant changes within the placebo group. In chronic migraine patients, after an 8-week intervention, the mean frequency of migraine attacks significantly reduced in the probiotic compared to the placebo group (mean change: −9.67 vs. −0.22; p ≤ 0.001). In contrast to the placebo, probiotic supplementation significantly decreased the severity (mean changes: −2.69; p ≤ 0.001), duration (mean changes: −0.59; p ≤ 0.034) of attacks and the number of abortive drugs taken per day (mean changes: −1.02; p < 0.001), in chronic migraine patients. We failed to detect any significant differences in the serum levels of inflammatory markers at the end of the study either in chronic or in episodic migraineurs.
Discussion
The results of this study showed that the 14-strain probiotic mixture could be an effective and beneficial supplement to improve migraine headache in both chronic and episodic migraineurs. Further research is required to confirm our observations.
Background
Migraine is accompanied by many comorbidities (1). Based on International Headache Classification (ICHD) III criteria, migraine has been divided into two subtypes: Episodic migraine (EM) and chronic migraine (CM). EM is more prevalent than CM, but severe headache-related disability is considerably higher among CM patients (2,3).
Although the pathophysiological mechanisms that lead to migraine attacks are yet to be determined, the role of “neurogenic inflammation” has attracted much attention. There is accumulating evidence showing an augmented inflammatory state marked by elevated pro-inflammatory cytokine concentrations, which contributes to trigeminal nerve activation and increased levels of vasoactive neuropeptides that could be involved in pain sensitization in the head (4–10). Also, migraine is a primary headache disorder and can be accompanied by gastrointestinal (GI) and autonomic symptoms (11). Several lines of research on the association between migraine and GI disorders have observed the higher prevalence of headache in patients who suffer from GI complaints (12–14). Moreover, migraine headaches might have a relationship with inflammatory bowel disease and celiac disease (15,16). Although the exact mechanism of the relationship between migraine and GI disorders remained unclear, the possible underlying explanation is attributed to increased gut permeability and inflammatory responses (12,17). Gut permeability and inflammation have a bidirectional relationship; not only can increased gut permeability trigger inflammation, but inflammation can also increase intestinal permeability (18,19). Pro-inflammatory cytokines can also act on the nociceptors of the trigeminal nerve, causing migraine (20,21). A strong trigger of pro-inflammatory immune responses is leakage of lipopolysaccharides from the intestinal lumen into the circulation (22).
As is well documented, probiotics can minimize inflammation, increase short-chain fatty acid (SCFA) levels in the gut, and attenuate intestinal epithelial cell permeability. Considering this known role of probiotics and neurogenic inflammation theory in migraine, we hypothesized that probiotic supplementation might have an effect in alleviating migraine attacks through various mechanisms including suppressing mitogen-activated protein kinase (MAPK) and nuclear factor kappa-B (NF-κB) pathways, reducing the concentration of pro-inflammatory biomarkers, improving the intestinal barrier defense and stimulating the production of tight junctional protein mucins (22–24). With this in mind, investigating the influences of probiotic supplementation on migraine features to establish a mechanistic pathway can be of great value.
So far, three studies have been conducted on the effectiveness of probiotic supplementation in migraine control. Two open-label studies reported that probiotic supplementation could result in significant improvement in a number of migraine-related outcomes (25,26). However, a randomized clinical trial investigating the effects of a probiotic mixture on migraineurs failed to show significant changes in migraine characteristic compared to the placebo group (27). Thus, the amount of previous research on this topic is limited and the results are controversial. However, it should be noted that the probiotic supplements in these studies consisted of seven bacterial strains and no study specified the migraine type.
Therefore, we designed a double-blind, randomized placebo-controlled trial to assess whether supplementation with 14 bacterial strains of probiotic is effective in alleviating the frequency, severity, and duration of attacks and the number of migraine days per month, in episodic and chronic migraine suffers, as the primary endpoints of the study. We also aimed to explore changes in the number of abortive drugs and pro-inflammatory cytokines including tumor necrosis factor alpha (TNF-α) and C-reactive protein (CRP) after the intervention, which were considered as secondary endpoints of the present research.
Materials and methods
Participants
A total of 50 EM (35 females and 15 males) and 50 CM patients (37 females and 13 males) were recruited for the current study. Participants were recruited consecutively among patients who visited a tertiary private headache clinic. The patients included were aged from 18 to 60 years old (mean age = 37.97 ± 8.86 years), suffering from EM and CM based on an expert neurologist headache specialist's diagnosis, according to the ICHD III criteria (beta version). Based on these criteria, patients who suffer from episodic migraine experience less than 15 headache days per month, while chronic migraineurs had more than 15 headache days per month (28).
Patients who had been taking any antipsychotic and/or antibiotic drugs or probiotic supplements or foods fortified by probiotic for 2 months prior to the beginning of the study, and pregnant or breastfeeding patients, were excluded.
This study protocol was reviewed and approved by the ethical committee of Shahid Beheshti University of Medical Sciences (SBMU) Tehran, Iran (ethic code: IR.SBMU.nnftri.Rec.1395.67, IR.SBMU.nnftri.Rec.1395.66). Informed consent was obtained from each participant. The trial was registered at the Iranian Registry of Clinical Trials (IRCT201706239157N6).
Study design
The current study was a randomized, double-blind, placebo-controlled trial. The enrollment of subjects was performed by study researchers. Chronic and episodic patients were randomly allocated to group A or B in a 1:1 ratio using a four-block randomization method both for the chronic and the episodic group. Only one of the staff on the development committee of Protexin, the company that supplied the probiotic or placebo, was aware of whether group A or B was intervention or control. Thus, both participants and researchers were blinded and the randomization codes (A or B) were kept confidential until all subjects had completed the study. Several previous studies showed beneficial effects of probiotics could be observed after 4 weeks' supplementation (29–31). Therefore, we conducted the present trial over 10 weeks in the EM group and over 8 weeks for the CM group.
Intervention
During the intervention, all subjects (group A and B), received two capsules of probiotic or placebo once a day, which had a completely similar appearance. Patients in group A received a multispecies probiotic product (Bio-Kult-protexin: 2 × 109 CFU/capsule) that contained 14 bacterial strains: Bacillus subtilis PXN 21, Bifidobacterium bifidum PXN 23, Bifidobacterium breve PXN 25, Bifidobacterium infantis PXN 27, Bifidobacterium longum PXN 30, Lactobacillus acidophilus PXN 35, Lactob. delbrueckii ssp. bulgaricus PXN 39, Lactob. casei PXN 37, Lactob. plantarum PXN 47, Lactob. rhamnosus PXN 54, Lactob. helveticus PXN 45, Lactob. salivarius PXN 57, Lactococcus lactis ssp. lactis PXN 63, and Streptococcus thermophilus PXN 66. The placebo capsule filler was microcrystalline cellulose in a vegetable capsule (hydroxypropyl methylcellulose).
All other types of probiotic products were forbidden during the study for both the intervention and placebo group. Patients were allowed to continue their prophylactic drugs for headache, but were asked not to change their prophylactic medications throughout the study period.
Demographic and anthropometric data
Prevalence of gastrointestinal problems among those studied.

Headache diaries
The migraine headache characteristics were recorded using a paper-based diary (designed by the senior researcher, Dr Togha) (19) that included onset time of attacks, duration of attacks, severity of attacks using a visual analog scale (VAS), and the daily number of abortive drugs consumed. A baseline diary was completed during the month prior to the beginning of the intervention. Then, all patients were asked to complete a headache diary during the study. The instruction for filling in the paper-based diary was given by our neurologist and if there was any question or problem about completion of the headache diaries, the participants could get in touch with our researchers.
Blood collection and inflammatory marker measurements
In order to assess C-reactive protein (CRP) and tumor necrosis factor alpha (TNF-α) levels in serum, blood samples (5 ml) were collected by a trained laboratory technician at the first visit and the end of the study. After centrifuging the blood samples for 10 minutes at room temperature, serum samples were stored at −80℃ until analysis. Serum level of TNF-α was measured using enzyme- linked immunosorbent assay (ELIZA), via a Diaclone kit. Turbidimetric immunoassay was also performed in order to measure serum CRP level.
Statistical analysis
Departure from normality was examined by the Kolmogorov–Smirnov distribution test. Descriptive data were presented for all variables. Comparisons between the four groups of patients and controls were made using a one-way analysis of variance (ANOVA) test in the case of continuous variables and the chi square test in the case of categorical data. Pre and post variables were compared using a paired t-test. Also, the Independent Student's t-test was applied in order to perform two-by-two comparison analysis.
The sample size was calculated based on considering α = 0.05, β = 0.2, and S = 8. Thus, at least 20 subjects in each group were estimated using 80% power with the aim of detecting a decrease of at least 5 in the number of attacks per month.
Furthermore, analysis of covariance (ANCOVA) models were applied to compare headache characteristics between groups, two-by-two (chronic migraineurs probiotic supplemented, chronic migraineurs placebo supplemented, episodic migraineurs probiotic supplemented, episodic migraineurs placebo supplemented). The models were adjusted for gender, age, BMI, dietary energy intake and headache characteristics at baseline. Then, changes in means for each of the headache characteristics are presented in the figures.
The test level for statistical significance of differences between and within the studied groups was defined as p-value = 0.05. Data were analyzed using Statistical Package for Social Sciences software (version 19, SPSS Inc., Chicago, IL, USA).
Results
Patient characteristics
The study sample consisted of 50 EM and 50 CM patients. Throughout the intervention, in episodic migraineurs, 10 patients were excluded from the study. Three patients in the intervention group were excluded (one became pregnant and two started to use antibiotic drugs because of infections). We also failed to follow up seven patients in the EM control group, because two patients started to take antibiotics due to an infection, and five subjects refused to continue the study because their headache attacks were not improved. In total, 40 episodic patients completed the treatment, corresponding to 80% of the samples (Figure 1). The episodic group consisted of 22 patients (15 females and seven males) in the probiotic and 18 patients (13 females and five males) in the placebo group.
Flow chart of studied participants.
Among chronic migraineurs, four patients from the intervention group (one patient because of antibiotic consumption and three patients who refused to continue because of personal problems) were excluded. Also, seven patients from the control group (three patients started to use antibiotics and four patients were not willing to continue) were lost to follow-up (Figure 1). At the end of the study, 21 probiotic-treated CM patients (17 females and four males) and 18 placebo-treated CM patients (12 females and six males) were evaluated.
Baseline demographic and anthropometric characteristics and dietary intakes of migraine patients enrolled in a trial of probiotic vs. placebo supplementation

#BMI: body mass index
Note: p-values for categorical variables were calculated from chi-squared tests; p-values for continuous variables were calculated from one way ANOVA tests. Letters represent significant differences between each variable and two other variables, calculated by Bonferroni test (post-hoc).
The prevalence of a history of gastrointestinal disorders among the studied groups is demonstrated in Table 1.
Changes in migraine characteristics
Migraine attack frequency
After the 10-week intervention, attack frequency significantly reduced in the EM probiotic-supplemented group compared to baseline; however, it did not change significantly within the placebo group (mean changes were −2.64; p < 0.001 in the probiotic and 0.06 for the placebo groups) (Table 3). Furthermore, after considering gender, age, BMI, dietary energy intake and mean attack frequency at baseline in the ANCOVA model, the effect of probiotics on reducing the mean frequency of migraine attacks was significant in EM patients (p < 0.001) (Figure 2).
Comparison of headache characteristics in the episodic migraineurs before and after 10-week supplementation with probiotic or placebo after considering gender, age, BMI, dietary energy intake and means of headache characteristics at baseline in ANCOVA model. Changes in the use of abortive drugs and in headache characteristics before and after supplementation with probiotic or placebo in a group of migraine patients. Note: Data are presented as mean ± standard deviation. The number of abortive drugs consumed was daily in CM and weekly in EM. Paired t-test was used to compare pre-post tests. #One-way ANOVA was used to compare between groups. a,b,c,d,eLetters represent significant differences between each variable and two other variables, calculated by Bonferroni test (post-hoc).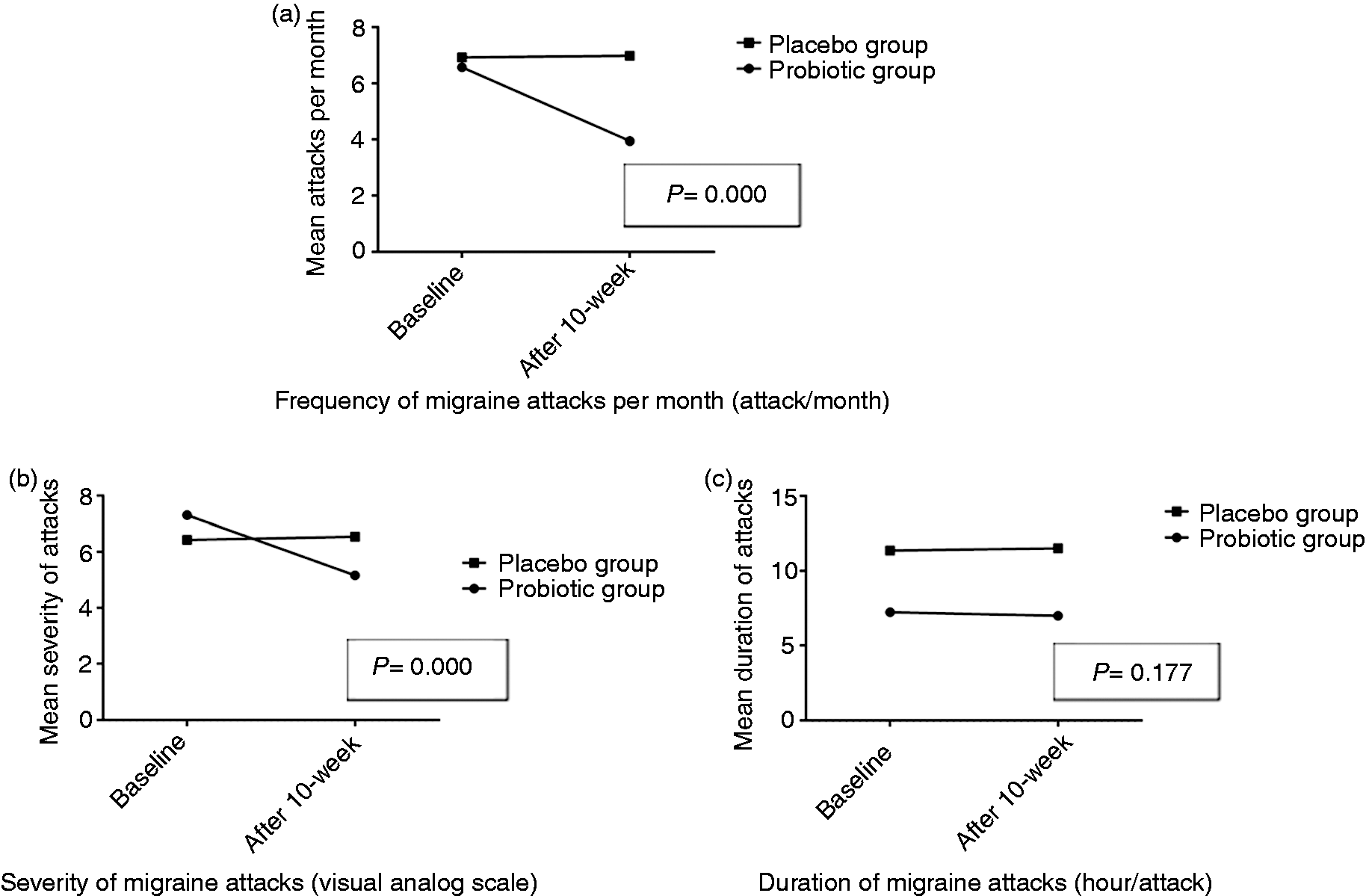

The frequency of migraine attacks significantly reduced in the CM probiotic-supplemented group compared to baseline, while no significant change was shown in their placebo controls (mean changes were −9.67; p < 0.001 in the probiotic and −0.22 in the placebo groups) (Table 3). Moreover, after considering the aforementioned confounders in ANCOVA model, migraine frequency in the CM probiotic-supplemented group significantly reduced compared to the placebo group (p < 0.001) (Figure 3).
Comparison of headache characteristics in the chronic migraineurs before and after 8-week supplementation with probiotic or placebo after considering gender, age, BMI, dietary energy intake and means of headache characteristics at baseline in ANCOVA model.
CM patients in the probiotic group had significantly higher mean changes in migraine attack frequency than other studied groups (p < 0.001) (Table 3).
Migraine days per month
EM patients in the probiotic group had a significant reduction in the number of migraine days per month compared with baseline, while the EM subjects in the placebo group had no significant changes over the study in terms of migraine days (mean changes: −3; p < 0.001; in the probiotic and 0.17 in the placebo group).
Unlike the CM patients in the placebo group, the CM probiotic-supplemented subjects had significant reduction in the number of migraine days per month compared to baseline (mean changes: −9.81; p < 0.001 in the probiotic and 0.06 in the placebo group).
The mean changes in migraine days per month were significantly higher in CM patients who supplemented with probiotic in comparison with the other three groups studied (p < 0.001).
Migraine severity
EM patients in the probiotic group had a significant reduction in migraine severity, while there were no significant changes observed in the EM placebo group (mean changes were −2.14; p < 0.001). Following adjustment of ANCOVA models for confounders including gender, age, BMI, dietary energy intake and mean severity of attacks at baseline, migraine severity in EM patients in the probiotic group significantly reduced compared to the placebo group (p < 0.001) (Figure 2).
There was a significant decrease in migraine severity in CM patients who received probiotic compared to baseline, while this significant change was not observed in the CM placebo group (mean changes were −2.69 in the probiotic group; p < 0.001 and −0.22 for the placebo groups). After adjustment for the mentioned confounders, the impact of probiotics on reduction of migraine intensity in CM patients remained significant (p < 0.001) (Figure 3).
After comparing the migraine severity between the four studied groups by ANOVA, it was shown that there was a significantly higher mean difference among CM patients in the probiotic group compared to the CM and EM placebo groups (p < 0.001).
Migraine duration
Neither EM patients in the probiotic group, nor EM patients in the placebo group showed a significant change in attack duration compared to baseline (mean changes were −0.24 in the probiotic and 0.15 in the placebo group) (Table 3). After considering gender, age, BMI, dietary energy intake and mean duration of attacks at baseline in the ANCOVA model, no significant difference in migraine duration was observed between EM patients in the probiotic and placebo groups (Figure 2).
Among CM patients, those in the probiotic group had a significant decrease in migraine attack duration at the end of the trial, while, no significant changes were observed in the placebo group (mean changes were −0.59; p = 0.034 in the probiotic and −0.20 in the placebo group (Table 3). Furthermore, after adjusting for the mentioned confounders, a significantly higher decrease in attack duration was observed in the CM probiotic group compared to the CM placebo group (p = 0.046) (Figure 3).
There was a significantly lower duration of attacks among the EM supplemented group than the other three groups, at baseline and at the end of the intervention (p < 0.001). However, the mean changes of duration of attacks between the four groups was not significant.
The number of abortive drugs
Changes in the number of abortive drugs consumed before and after supplementation with probiotic or placebo in a group of migraine patients.

Note: Data are presented as mean ± standard deviation. Letters represent significant differences between each variable and two other variables, calculated by Bonferroni test (post-hoc).
¥The number of abortive drugs consumed was daily in CM and weekly in EM.
€Independent sample t-test was used to compare groups two by two.
Paired t-test was used to compare pre-post tests.
#One-way ANOVA was used to compare between groups.
Unlike the CM subjects in the placebo group, CM patients in the probiotic-supplemented group had a significant reduction in the mean number of abortive drugs consumed per day (mean changes: −1.02; p < 0.001 for within-group comparison in the CM probiotic group; and 0.41 in the CM placebo group) (Table 4).
Consumption of medications in the studied groups at baseline.

Inflammatory markers
changes in the TNF-α and CRP level before and after supplementation with probiotic or placebo in a group of migraine patients.

Note: Data are presented as mean ± standard deviation. Letters represent significant differences between each variable and two other variables, calculated by Bonferroni test (post-hoc).
Paired t-test was used to compare pre-post tests.
#One-way ANOVA was used to compare between groups.
CM patients in the probiotic group had slightly increased serum levels of CRP after the intervention compared with baseline (from 1.77 mg/dl to 2.70 mg/dl), as did the CM placebo group (from 0.57 mg/dl to 0.74 mg/dl). The increment was significant only in CM patients who received probiotic supplementation (p = 0.005). TNF-α levels in the serum samples of CM patients had a non-significant increase compared to baseline in both the probiotic group (from 5.90 to 8.18 pg/ml) and the placebo group (from 3.12 to 5.73 pg/ml).
There were no significant differences between the four studied groups in terms of serum CRP and TNF-α level at baseline or at the end of the study.
Discussion
This randomized, placebo controlled, double-blind study investigated the effect of supplementing with 14 bacterial strains of probiotic mixture on episodic and chronic migraine characteristics. Significant improvements were seen both in episodic and chronic migraine headaches among those who supplemented with the probiotic mixture in terms of the frequency and severity of attacks, the number of migraine days per month and the number of abortive drugs consumed. A comparable effect was not observed in the placebo groups.
The results of the current study are consistent with the two previous open-label studies concerning the beneficial effect of probiotics on migraine parameters. In the first study, Sensenig et al. showed that a probiotic supplement plus minerals (magnesium aspartate, manganese glycerylphosphate, zinc gluconate, and copper glycinate), vitamins (thiamine mononitrate and pyridoxal 5-phosphate), and herbs caused near total relief of attacks in 60% of migraine patients after 12 weeks. Also, 80% of patients reported significant improvement in their quality of life (25). The second open-label study applied seven bacterial strains of probiotic mixture to migraineurs. They observed a 25% reduction in the frequency of migraine attacks and improved migraine disability after probiotic supplementation (26).
Our findings on episodic migraine subjects revealed that 10-week probiotic supplementation among episodic migraineurs resulted in a significant decrease in migraine frequency (mean change: −2.64), number of migraine days per month (mean changes: −3.00), attack severity (mean changes: −2.14) and abortive drugs consumed per week (mean change: −0.72). The reduction of the mean value of the mentioned characteristics in episodic migraine remained significant even after adjusting for potential confounders. Although the mean duration of attacks within both episodic groups did not change significantly during the trial, we observed significant differences between groups at both baseline and after the intervention. Based on ICHD III (beta version) criteria, each migraine attack can last from 4 to 72 hours (28). Thus, when studying migraineurs, it is not possible to match all headache characteristics including duration of attacks among study arms in this regard, but the mean duration of headache attacks in both groups was within the accepted range for diagnosis of migraine attacks.
Furthermore, the study of chronic migraineurs suggested that 8-week probiotic supplementation significantly reduced migraine attack frequency (mean changes: −9.67), number of migraine days per month (mean changes: −9.81) severity of attacks (mean changes: −2.69) and daily abortive drugs consumed (mean changes: −1.02) even after considering confounding variables. Unlike episodic migraineurs, we observed a significant mean reduction of 0.59 hours per attack in the mean duration of attacks in probiotic-supplemented chronic migraineurs compared to baseline.
According to the four group comparisons, CM patients in the probiotic-supplemented group had significantly higher mean reduction in the number and frequency of migraine days compared to the other three groups relative to baseline. The observed differences could be partially explained by the fact that, because migraine characteristics are more severe in chronic migraineurs, the effect of probiotic supplementation was more detectable in these patients.
The beneficial effects of probiotics on migraine may be related to their role in improving gut integrity (12). An imbalance in gut microbiota and an increase in pathogenic and gram-negative bacteria results in the leakage of lipopolysaccharides (LPS) from lumen to blood. LPS is a strong trigger of pro-inflammatory immune responses. Pro-inflammatory markers, such as TNF-α, IL-1β and IL-6, have been reported to be a pain mediator in neurovascular inflammation and they could stimulate the activation of trigeminal nerves (9,32–35).
Also, previous researches have reported a rise in the serum levels of pro-inflammatory cytokines like PPAR-γ, TNF-α and interleukin 1β during migraine attacks (9,20,36). Based on this hypothesis, we measured the serum level of TNF-α and CRP. However, only a slight, non-significant reduction in episodic patients and a slight increase in chronic migraineurs was observed after probiotic supplementation. We estimated the time since the last attack and the time that blood samples were collected from patients in order to check whether there is any relation between the last attack and the levels of inflammatory biomarkers in episodic migraine patients. It was shown that the mean time was about 9 days in the probiotic group and 7 days in the placebo arm, which were almost similar.
One of the other possible mechanisms for the beneficial effects of probiotics on migraine is the role of gastric stasis. Gastric stasis is one of the gastrointestinal conditions co-occurring with migraine. Migraineurs experience delay in gastric emptying during and between attacks, and this phenomenon may complicate migraine treatment (37). Probiotics can significantly increase the gastric emptying rate via neuroimmune interaction (38,39).
However, in contrast to our results, the only previous randomized clinical trial concerning migraine and probiotics by De Roos et al. reported different results. They showed that migraineurs who supplemented with a probiotic mixture of seven bacterial strains for 12 weeks did not have any significant improvement in migraine parameters compared to the placebo group (27). The observed difference could be in part explained by the number of bacterial strains and type of probiotic products. In the De Roos et al. study, a seven-bacteria strain consisting of Bifidobacterium bifidum W23, B. lactis W52, Lactobacillus acidophilus W37, Lactob. brevis W63, Lactob. casei W56, Lactob. salivarius W24, Lactococcus lactis W19 and Lactoc. lactis W58 was used. Our probiotic supplement consisted of 14 bacterial strains. For example, Lactobacillus plantarum in the currently used probiotic mixture is reported to have a protective effect against LPS-induced inflammation and inflammatory bowel disease (40–42). Furthermore, our probiotic mixture contained Bifidobacterium infantis, which according to previous results has a modulatory effect on systemic inflammatory biomarkers in both gastrointestinal and extra-intestinal inflammatory disorders (43). On the other hand, the female-to-male ratio in the current study was 2.7:1, which is similar to previously reported ratios for migraine prevalence in different studies (2:1 or 3:1) (44), while this ratio was 14:1 in the De Roos et al. study, which may not represent the female-to-male ratio of migraine prevalence in the general population.
The strengths of the current research are the prospective, double-blind, placebo-controlled design, using a 14 bacterial strain probiotic in episodic and chronic migraineurs for the first time, recruiting the subjects by expert neurologist headache specialist diagnosis, and obtaining a reasonable ratio of men and women in the study. Notably, we encountered no side effects (such as bloating, GI discomfort, diarrhea etc.) for this probiotic product throughout the study.
Limitations in our study were that we only measured serum levels of TNF-α and CRP as inflammatory markers, while we know that there are more inflammatory markers involved in migraine pathophysiology. Also, because the study was undertaken in winter and taking antibiotics was one the exclusion criteria, the drop-out rate (about 20%) was quite high.
However, the finding of elevated serum level of TNF-α either during attacks or attack-free intervals in migraineurs points to TNF-α as a potentially critical cytokine of migraine pathology (9,45,46). Furthermore, we did not assess the gut permeability because we were not able to collect the patients' urine samples in fasting condition for a lactulose/mannitol test. Although multiple studies have indicated the possible association between migraine and gastric stasis, the gastric emptying rate was not assessed in our participants.
Conclusion
The results of this study showed that a 14-strain probiotic mixture could be an effective and beneficial supplement for improving migraine headaches in both chronic and episodic migraineurs. More precise researches are needed to establish the place of probiotics in migraine treatment and find the underlying mechanism of the probiotic effect.
Footnotes
Article highlights
Several lines of research on the association between migraine and gastrointestinal disorders have observed the higher prevalence of headache in patients who suffer from GI complaints.
The possible underlying explanation might be attributed to increased gut permeability and inflammatory responses.
Our findings suggest probiotics as a beneficial supplement in episodic and chronic migraineurs due to their possible effect in improving migraine characteristics.
The beneficial effects of probiotics on migraine may be related to their role in improving gut integrity and modulating the gut-CNS axis.
Acknowledgements
We thank the participants of the present study. In particular, we extend our gratitude to Ms. Jabbari, and the staff of the National Nutrition and Food Technology Research Institute and Iranian Center of Neurological Research for their kind cooperation. This study was conducted as part of a Master’s thesis in Shahid Beheshti University of Medical Sciences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.