
Abstract
Aim
To investigate whether the self-treatment of migraine among neurologists and pain specialists corresponds to national medical guidelines and treatment of patients.
Methods
An email cross-sectional survey was sent to members of the German Society for Neurology, German Pain Society and German Migraine and Headache Society containing questions on demographics, professional experience and specialization and – in case participants suffered from migraine – questions about their migraine and its treatment.
Results
175/418 (41.9%) participants suffered from migraine (m: 29.3%; f: 55.2%, 45.9 ± 10.7 years). For acute migraine attacks, 96.6 % of them use a first-line treatment according to the medical guidelines. Seventeen (9.7%) are currently taking a migraine prophylaxis, 52.9% of these use a recommended first-line prophylaxis. In all, 21.7% are not taking a prophylactic treatment despite an indication (based on number of monthly migraine days) for it, due to fear of side-effects, low intensity of migraine attacks and a sufficient effect of acute medication. This group of participants was younger, less experienced and specialized and was mainly employed (vs. self-employed) compared to those taking a prophylaxis. A total of 96.6% reported treating their patients in line with current guidelines; 14.3% would treat themselves differently when they were their own patients.
Conclusion
The self-treatment of acute migraine attacks for the most part complies with the guidelines but, regarding the indication for a prophylaxis, a more divergent treatment approach was observed among younger, less experienced physicians. For the majority of physicians there is no difference between self-treatment and treatment of migraine patients.
Abbreviations
DGN: German Society for Neurology; DGSS: German Pain Society; DMKG: German Migraine and Headache Society; NSAID: non-steroid anti-inflammatory drug; ASA: aspirin; OTC: over-the-counter.
Introduction
Migraine is a common disease and has a higher prevalence among neurologists compared to the general population (1–4) where a 1-year prevalence of around 11% is reported (5,6). International studies have shown that the prevalence rate of migraine among neurologists is between 27.6–65.9% (1–3,7,8). Within Germany, a prevalence of 33.1% is reported (9).
Physicians often treat themselves without consulting a specialist colleague (10,11). In a large study conducted in the United States, migraine was identified as a disease diagnosed and treated by a large percentage of neurologists without consultation with a colleague (12). Reasons for the self-treatment might be being fully occupied with work, unavailability of family doctors after work, simplicity to treat and a pressure of being able to handle one’s own health problems (10). Especially under young doctors, who are often pressured in their early career, a medical culture of self-reliance exists, which may lead to inappropriate health behavior (11). This could for example result in medication overuse for those having frequent headache (12). In addition, doctors often work despite illness and rarely take sick leave (11,12) because they feel responsible for patients, do not want to leave colleagues alone, want to demonstrate a good commitment to their job or because they are afraid to be regarded as lazy or would be ashamed if anyone knew that they suffered from mental illness (10).
Since migraine is a common, well characterized and relatively easily diagnosable disease, this study was therefore intended to determine how the self-treatment of migraine among neurologists and pain therapists in Germany complies with current medical guidelines and whether it differs from the treatment of patients.
Methods
An email cross-sectional survey was sent to members of three selected German medical expert associations (the German Society for Neurology (DGN), German Pain Society (DGSS) and German Migraine and Headache Society (DMKG)). The survey was developed with a software solution to conduct automated surveys (13) and included a questionnaire which contained questions on demographics, professional experience and specialization, presence and frequency of migraine as well as its acute treatment, prophylaxis and non-medical treatment according to the national medical guidelines of the DGN for migraine treatment (14). Question types were single-choice, multiple-choice and open-ended (Supplemental material). The data were collected from September 2017 to April 2018. An ethics vote for the survey was obtained from the Ethics Committee of the University Hospital of Schleswig-Holstein, Campus Kiel, Germany (D 424/17). Before completion of the questionnaire, participants were informed that the survey was designed to learn more about the self-treatment among neurologists and pain therapists, that the results of this survey would be used for research purposes only, that the answers will be kept strictly confidential and that each participant has the right to terminate participation of the survey at any time. This reading had to be confirmed by clicking on a button to start the survey (Supplemental material).
Statistical analysis
Frequency, ranges, mean and standard deviation (SD) were used to summarize the characteristics of each group of participants. To determine statistical significance of differences between groups, analysis of chi-square tests of independence (categorical variables) were used. T-test was used to compare the difference between mean responses of two different samples (continuous variables). A two-sided p value <0.05 was considered statistically significant.
Results
Four hundred and eighteen participants completed the survey. The flowchart of the study selection can be seen in Figure 1. One hundred and seventy-five out of the 418 (41.8%) respondents reported having a personal history of migraine (Table 1). The respondents with migraine were more often female, slightly younger, and were more often neurologists compared to the group of non-migraineurs (Table 1). In addition, they worked part-time more often than respondents without migraine (Table 1), but this was not due to their migraine as only 2/54 (3.7%) part-time workers reported working part-time because of their migraine.
Flowchart of the study selection. Demographic characteristics of all respondents, n = 418. of the medical specialists.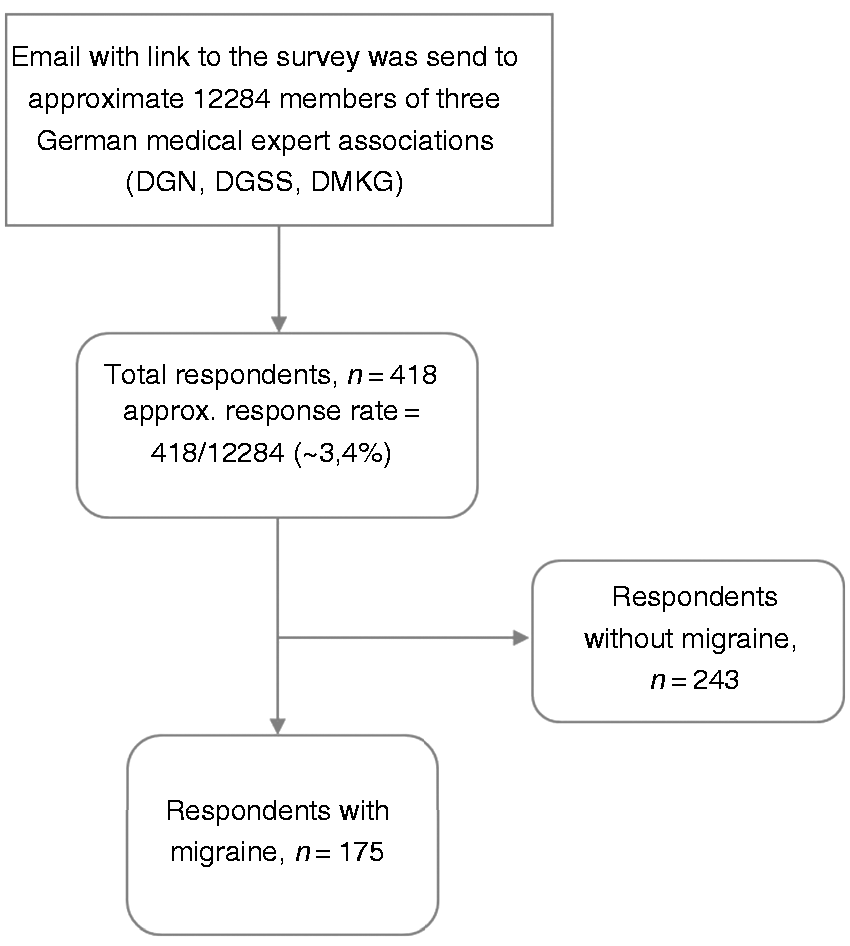

Characteristics of migraineurs
Characteristics of migraineurs.

within the last four weeks.
One hundred and thirty-two out of the 175 (75.4%) migraineurs reported that they had suffered from migraine attacks during the last 4 weeks. Despite having migraine complaints on an average of 3.1 ± 5.4 (0–28) days, 119/132 (90.2%) respondents stated that they had not had days of absence of work due to migraine. The two participants with chronic migraine were working full time.
Treatment of acute migraine attacks
Ibuprofen (61.6%) was most commonly used for acute migraine attacks, followed by triptans (28.5%), aspirin (ASA, 22.8%), metamizole (20.5%), paracetamol (17.1%) and antiemetics (13.1%, Figure 2). Fifty respondents (28.6%) used triptans, 12 (24%) of them as single-use, 38 (76%) in combination with ibuprofen (68.4%), ASA (23.7%), naproxen (5.3%), diclofenac (2.6%), metamizole (23.7%), antiemetics (18.4%), paracetamol (7.9%) or mixed analgesics (2.6%). Overall, 135/175 (77.1%) used a NSAID or ASA for the treatment of acute migraine attacks. One participant showed an overuse of analgesics, with an intake on 29 days during the last 4 weeks. Concordant with the mean value of migraine days, anti-migraine drugs were used on 2.1 ± 2.7 (0–28) days. Fourteen (8%) reported that the choice of the acute therapy is due to contraindications against medications usually used for the treatment of migraine attacks. Overall, 96.6% used a medical treatment which complies with the first-line therapy according to the medical guidelines of migraine treatment.
Substances taken for the acute migraine attack. The ordinate shows the number of mentions (n).
Pharmacological migraine prophylaxis
Seventeen (9.7%) respondents reported taking a migraine prophylaxis (Figure 3). Betablockers were the most commonly used migraine prophylaxis, followed by sartans, which were interestingly not approved for prophylactic treatment of migraine at the time of data collection. Only one out of the five patients taking sartans reported having arterial hypertension, which may explain the use of sartans in this case. Overall, approximately half of the group taking a migraine prophylaxis (52.9%) used a first-line recommendation (betablocker, flunarizine, valproate, topiramate).
Substances taken for migraine prophylaxis, n = 17.
Sixteen physicians (94.1%) confirmed their migraine got better by taking a prophylactic medication. The reported migraine days within the last 4 weeks within the group taking a prophylaxis were 4.9 ± 6.8 (1–29) days. Two participants (11.8%) reported that the choice of the prophylaxis was due to contraindications against medications usually used for prophylactic treatment. All of the 17 stated that they treated their patients in compliance with guidelines. Two out of the 17 (11.8%) would treat themselves differently when they were patients in their own treatment. [Please clarify this phrase ‘in their own treatment’, found here and towards the end of the next paragraph, as well as in the Abstract and elsewhere. Does it mean that these physicians would treat themselves differently if they were their own patients?]
Comparison between participants with and without migraine prophylaxis.

of the medical specialists.
Non-pharmacological migraine prophylaxis
A total of 85.7% stated that they used non-medical procedures for migraine prophylaxis. The most commonly used procedures were sports (49.1%), endurance sports (43.4%), a regulated lifestyle (45.1%), relaxation techniques (31.4%), stress management (25.1%), abstention from alcohol (18.9%), pain management strategies (6.9%), acupuncture (4.6%), psychotherapy (2.9%) and biofeedback (0.6%).
Self-evaluation
A total of 96.6% of the respondents stated that they treated their patients in compliance with guidelines. At least 14.3% would treat themselves differently when they were patients in their own treatment.
Discussion
Our hypothetical assumption was that doctors often do not behave according to the guidelines in their own treatment. However, this study shows that not only does the therapy of the patients seem to be usually guideline-compliant but also the self-treatment of their own acute migraine attack for the most part complies with recommended guidelines. However, regarding migraine prophylaxis of one’s own migraine, a more restrained approach can be observed in younger, less experienced doctors, where 23.7% would treat themselves differently when they were patients in their own treatment (and 13.2% did not provide any information for this question). This supports the observation that the self-care of younger doctors has room for improvement (11).
Similar to previous studies in other countries, we found a higher prevalence of migraine (41.9%) among neurologists. There are various explanations for this: On the one hand, it seems obvious that neurologists and pain therapists are particularly good at identifying and clinically diagnosing migraine as professional experts because they are more familiar with the diagnosis than, for example, non-neurologists, and thus have a sharper awareness and more appropriate recognition for migraine (2,3). This could mean that migraine is an underdiagnosed and undertreated disease in the normal population (3,5,6,15). On the other hand, their own migraine could have led to a special interest in neurology and the choice of specialization (2). In addition, a connection between a migraine personality and the interest in neurology is discussed (1), but the existence of such a migraine personality has not been verified so far (16).
Acute treatment of migraine
The present study has shown that the acute treatment of doctors’ own migraine attacks for the most part complies with the guidelines. The therapy of first choice for self-therapy of acute migraine attacks in our study was ibuprofen (61.6%), with 77.1% taking a drug from the group of NSAIDs or aspirin (ASA) for acute migraine attacks, whereas triptans were used by only about one third of patients. Similar findings were found in a study by Brockmann et al. with data from 2008, in which neurologists used NSAIDs/ASA for self-treatment of acute migraine attacks in 74.4% of cases (9) and triptans in only 23.3%, although over 95% of the participating neurologists in the study recommended them to patients. Thus, over time, data has not changed much. Other studies from Germany, Finland, Italy and Taiwan also showed low triptan use and predominant use of NSAIDs/ASA by patients (8,17–19). Possible reasons for a low use of triptans for self-treatment of acute migraine attacks might be fear of side effects (8,20) or contraindications, easier availability of over-the-counter drugs (as part of the private medicine chest) (8,20) and a rather lower symptomatology of migraine attacks that responds well to NSAIDs/ASA without the additional need for triptans. Since only 8% reported that the choice of treatment was due to contraindications to one of the drugs commonly used in the treatment of migraine attacks, contraindications might play a little role. Since we did not specifically address this item in the questionnaire, we cannot provide answers for the reasons with our data. The high rate of use of metamizole is probably explained by the fact that doctors get it in the pharmacy. As it is not an OTC drug in Germany, it plays a very subordinate role for non-medical migraine sufferers.
Prophylactic migraine treatment
Within our study, we found little use of prophylactics, especially among younger, less experienced doctors. A rather low use of drugs for prophylaxis was also demonstrated by Brockmann et al., where only 4.7% of neurologists and 13.3% of pain specialists took a prophylaxis (9). The question arises as to why so few participants take a prophylaxis. In a US survey, there was a 12.4% rate among migraineurs in the general population who took prophylaxis and 17.2% who were taking a substance for another medical reason that was simultaneously associated with antimigraine effects, such as betablockers (6). Another study from the USA showed that preventive medication is often not taken continuously, that there rarely is a switch to another treatment when necessary and that prophylaxis is often discontinued in the first year (21). Diamond et al. (6) also found that prophylactic use is more common in elderly patients, women, and in patients with a conscious perception of migraine and severe degree of sickness. The last point in particular could be one reason for a low frequency of migraine prophylaxis, as the frequency of migraine attacks in our study sample was rather low. However, we cannot conclude anything about the intensity of migraine attacks because this topic was not part of the questionnaire. Further, a prophylaxis aims to reduce migraine frequency and severity, but not to cure migraine completely (22). This means that a prophylaxis taken for episodic migraine with around 2–4 migraine days per month would only reduce the migraine days by around 1–2 days. Since effective prophylaxis usually also involves side effects (23), the benefits of a prophylaxis might be too low in comparison to the burden of side effects.
Similar to the findings of a study from Taiwan (8), betablockers were the first choice from the series of prophylactic drugs. This might be for their strong evidence, their effectiveness and their favorable side effect profile (22,24,25). The relatively frequent use of sartans in our study is interesting, because the new guideline of spring 2018 (26) only recommends sartans as a prophylactic if there is an arterial hypertension at the same time; however, at the time of our data collection, sartans were not the first choice for prophylactic treatment. It is conceivable that headache experts in particular already know and apply the latest studies before they have appeared in the revised guidelines.
Non-medical prophylactic treatment of migraine
In all, 85.7% of our participants used non-drug prophylaxis procedures. In the study by Brockmann et al. this rate was only between 15–35.1% of the participating physicians (9). A possible explanation for this discrepancy could be that the multiple-choice question in our survey also included answer options such as sports, endurance sports and regulated lifestyle – items that could be also carried out irrespective of the migraine prophylaxis and made up the three most common procedures. As a notable finding, we found that very time-consuming procedures such as psychotherapy and biofeedback that need to be scheduled into daily life were used very little. Whether this is due to lack of time or for other reasons needs to be elucidated in further studies.
Limitations
This study has limitations as a precise percentual response rate cannot be determined retrospectively, as the exact number of medical members of the three medical expert associations is unclear (around 12,284 total members); there may be dual memberships and it is uncertain whether all members have taken notice of the email with the invitation to participate in the survey. However, with 418 participants completing the survey and 175 migraine participants enrolled in the study, there is even a slightly higher participation rate compared to similar studies (1,8,9).
A potential response bias may have had an effect on the results of this study, especially since members with migraine may have felt particularly attracted by the survey. Furthermore, a selection bias cannot be excluded because only members of expert associations that explicitly deal with neurology/headache/pain/migraine were able to take part in the survey. This expertise could explain the high rate of patients and their own migraine attacks being treated in line with current guidelines. Furthermore, suffering from migraine might influence the migraine treatment of patients. This conclusion was also made by Evers et al. (20), who found in their study that suffering from the same disease for which one is a treating specialist influences not only the attitude towards this disease (in migraine, e.g. a rather somatic than biopsychosocial aetiological concept), but also the treatment of patients.
It should also be kept in mind that all except two participants suffered from episodic migraine. Results in participants with chronic migraine (27) might have been different.
Our questionnaire asked about the exact migraine frequency, but not the individual pain intensity and the duration of the migraine. These two aspects would have been of interest, as they might also have played an important role in the indication for prophylaxis. In addition, it was not asked exactly why a certain prophylaxis was taken and not another. Moreover, the questionnaire did not explicitly ask for the exact treatment of their patients, but only whether the participants themselves would be treated differently, when they were patients in their own medical treatment, and whether the participants treated their patients in accordance with the guidelines. Therefore, the comparison between self-treatment and treatment of their patients for guideline compliance is based solely on the self-assessment of these two questions.
Conclusion
The results of our study show medical guidelines are not only an important tool for quality assurance in patient care, but that for the most part, doctors are also guided by them concerning their self-treatment. However, data also give a slight hint that especially in younger doctors, self-care needs to be watched carefully in order to ensure a healthy and sustainable medical workforce.
Supplemental Material
CEP907593 Supplemental material - Supplemental material for Do doctors treat themselves differently than their patients? Study on the self-treatment of migraine among German neurologists and pain specialists
Supplemental material, CEP907593 Supplemental material for Do doctors treat themselves differently than their patients? Study on the self-treatment of migraine among German neurologists and pain specialists by Leonie C Hansen, Charly Gaul, Esther Pogatzki-Zahn, Ralf Baron and Janne Gierthmühlen in Cephalalgia
Footnotes
Clinical implications
Migraine has a much higher prevalence among neurologists than in the general population.
The self-treatment of acute migraine attacks of German physicians for the most part complies with the guidelines.
Regarding the prophylactic migraine treatment of German physicians, a more divergent treatment approach was observed among younger, less experienced doctors. However, when taking a prophylactic treatment this complies with current guidelines.
For the majority of German physicians, there is no difference between self-treatment and treatment of migraine patients.
Acknowledgements
The authors thank the German Society for Neurology (DGN), German Pain Society (DGSS) and German Migraine and Headache Society (DMKG) for advertising the survey on their member newsletters and emailing.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LH reports no conflicts of interest. CG has received honoraria for consulting and lectures within the past three years from Allergan Pharma, Bayer vital, Boehringer Ingelheim Pharma, Cerbotec, Desitin Arzneimittel, electroCore, Grünenthal, Hormosan Pharma, Lilly Germany, Novartis Pharma, Ratiopharm, Reckitt Benckiser, Sanofi Aventis, and TEVA. RB reports research funding from EU Projects: “Europain” (115007), DOLORisk (633491), IMI Paincare (777500), German Federal Ministry of Education and Research (BMBF): Verbundprojekt: Frühdetektion von Schmerzchronifizierung (NoChro) (13GW0338C), German Research Network on Neuropathic Pain (01EM0903), Pfizer Pharma GmbH, Genzyme GmbH, Grünenthal GmbH, Mundipharma Research GmbH und Co. KG., Novartis Pharma GmbH, Alnylam Pharmaceuticals Inc., Zambon GmbH; he has received speaker fees from Pfizer Pharma GmbH, Genzyme GmbH, Grünenthal GmbH, Mundipharma, Sanofi Pasteur, Medtronic Inc. Neuromodulation, Eisai Co. Ltd., Lilly GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, Astellas Pharma GmbH, Desitin Arzneimittel GmbH, Teva GmbH, Bayer-Schering, MSD GmbH, Seqirus Australia Pty. Ltd, Novartis Pharma GmbH, TAD Pharma GmbH, Grünenthal SA Portugal, Sanofi-Aventis Deutschland GmbH, Agentur Brigitte Süss, Grünenthal Pharma AG Schweiz, Grünenthal B.V. Niederlande and honoraria for consulting from Pfizer Pharma GmbH, Genzyme GmbH, Grünenthal GmbH, Mundipharma Research GmbH und Co. KG, Allergan, Sanofi Pasteur, Medtronic, Eisai, Lilly GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, Astellas Pharma GmbH, Novartis Pharma GmbH, Bristol-Myers Squibb, Biogenidec, AstraZeneca GmbH, Merck, Abbvie, Daiichi Sankyo, Glenmark Pharmaceuticals S.A., Seqirus Australia Pty. Ltd, Teva Pharmaceuticals Europe Niederlande, Teva GmbH, Genentech, Mundipharma International Ltd. UK, Astellas Pharma Ltd. UK, Galapagos NV, Kyowa Kirin GmbH, Vertex Pharmaceuticals Inc., Biotest AG, Celgene GmbH, Desitin Arzneimittel GmbH, Regeneron Pharmaceuticals Inc. USA, Theranexus DSV CEA Frankreich, Abbott Products Operations AG Schweiz, Bayer AG, Grünenthal Pharma AG Schweiz, Mundipharma Research Ltd. UK, Akcea Therapeutics Germany GmbH, Asahi Kasei Pharma Corporation, AbbVie Deutschland GmbH & Co. KG, Air Liquide Sante International Frankreich, Alnylam Germany GmbH, Lateral Pharma Pty Ltd, Hexal AG, Ethos Srl Italien. JG has received speaker fees and travel support from Pfizer, Novartis, Grünenthal, Sanofi Pasteur MSD GmbH, TAD Pharma and consultancy fees from Glenmark.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.