
Abstract
Objectives
The authors have previously tried to develop a model for the testing of novel drug candidates for migraine, using the headache and migraine provoking agent cilostazol. Previous studies have used sumatriptan tablets as the validating drug, but they were not sufficiently effective. In this study we test the effect of subcutaneous sumatriptan on cilostazol induced headache in patients with migraine without aura.
Method
Thirty patients with migraine without aura received 200 mg cilostazol on two different study days. The induced headache was treated with subcutaneous sumatriptan in a randomized, double-blind cross-over design. The patients filled out a self-reported headache questionnaire until 12 h after cilostazol.
Results
All 30 patients experienced headache (range 3–10) on both study days and the headache fulfilled the criteria for a migraine-like attack in 73% on the sumatriptan day and in 77% on the placebo day. Sumatriptan injection reduced the headache score 2 h after treatment (p = 0.003). The difference between headache intensity on the sumatriptan day and the placebo day was significant at both 2 h (p = 0.01) and 4 h (p = 0.0007) after treatment.
Conclusion
Subcutaneous sumatriptan reduces cilostazol induced headache in migraine patients. The cilostazol model may be useful as a tool to test the potential of new anti-migraine drugs.
Introduction
Experimental migraine provocation models have been extremely useful in discovering migraine mechanisms and in the understanding of the effects of migraine treatments (1,2). In the model, substances are administered to both healthy volunteers and migraine patients to study the headache- and migraine-generating properties of the drugs and the complex events during the headache and migraine phase.
If a substance induces migraine, targeting that molecule or its receptor may be an efficient treatment for migraine. In that way, the models have promoted the development of novel medications such as calcitonin gene-related peptide (CGRP) antibodies (3).
It would be beneficial to also have a model that could be used to test new drug candidates where volunteers come to the hospital for migraine induction followed by treatment with the new potential drug. In that way, the new drug can be tested in standardized settings at the hospital with the opportunity to not only measure the therapeutic response, but also take blood samples for pharmacokinetics, do neuro imaging and monitor safety. Our own group has conducted a series of studies using cilostazol (which induces headache in healthy volunteers and migraine in migraine patients (4–6)), aiming to develop such a model (7–9).
The cilostazol induced headache in healthy and migraine (without aura (MO)) patients was treated with sumatriptan tablets in a double-blind cross-over design to validate the model. Sumatriptan tablets stopped the headache from developing further in both healthy volunteers and in migraine patients, but the effect was not strong enough to reduce the headache significantly (7–9). Thus, the effect of sumatriptan tablets on cilostazol induced headache and migraine was not sufficient for a useful model.
The poor effect of sumatriptan may be due to the pharmacokinetics of tablets, which is inferior to injected sumatriptan. The bioavailability of tablets is 14% compared to 96% of injections (10). The tablets reach a Tmax after 2 h, whereas Tmax is only 10 min for injections (10). The therapeutic effect on spontaneous attacks is also known to be superior using subcutaneous sumatriptan compared to tablets (11). To investigate the most effective formulation of sumatriptan against cilostazol induced headache we therefore conducted the present double-blind randomized cross-over study of subcutaneous sumatriptan. The hypothesis was that subcutaneous sumatriptan could reduce cilostazol induced headache in MO patients.
Method
An almost identical method has previously been described by the authors (7,9).
Participants: Thirty patients with MO were included. Sixteen of the patients were self-reported triptan responders and the last 14 were triptan-naïve. Inclusion criteria were: Patients fulfilling IHS criteria for migraine without aura of both sexes, aged 18–60 years and weighing 45–95kg. Females were requested to use effective contraception.
Exclusion criteria were: Patients fulfilling any other type of headache than MO (except episodic tension-type headache <1 day per week), self-reported triptan non-responders, serious somatic or psychiatric disease, pregnancy, and intake of daily medication (except oral contraceptives).
Two participants dropped out after the first study day. Both got severe headache on day 1 and did not wish to come back for a second day. They were excluded from the analyses and replaced with new participants.
Standard protocol approvals
All participants gave written, informed consent to participate in the study. The study was approved by the Ethics Committee of Copenhagen (H-17026731), the Danish Medicines Agency and the Danish Data Protection Agency. The study is registered on clinicaltrials.gov (NCT03422796).
The study was conducted at the Danish Headache Centre, Rigshospitalet Glostrup, Denmark, over the period from November 2017 to July 2018.
The central pharmacy of the Capital Region of Copenhagen performed the randomization of the experimental drug in a balanced fashion. The randomization code did not leave the hospital during the study and was not available to the investigators until after termination of the study. We did not break the code until data management took place.
Study procedure: The study was a double-blinded, randomized, balanced, placebo-controlled, cross-over study. The patients had to be headache free 48 h prior to the study and to not have taken any type of painkillers 12 h before the beginning of the study. A pregnancy test was taken at the beginning of each study day for all fertile female participants. All participants attended two separate study days at least 5 days apart. They arrived non-fasting at the clinic between 8:00 am and 12:00 pm. Full medical history, physical examination, electrocardiography (ECG), vital signs and baseline headache were collected on arrival. All participants received cilostazol 200 mg orally on both study days. The participants stayed at the hospital until they reached headache intensity 4 on a numerical rating scale (NRS, corresponding to moderate headache intensity), where they received a subcutaneous injection with 6 mg sumatriptan or placebo (administered by a doctor or medical student). If the participant did not reach headache score 4 on NRS 6 h after cilostazol, the treatment was administered at that timepoint. Time of treatment was chosen as a trade-off between treating early enough and not treating before migraine mechanisms were activated. In case of severe headache not responding to the experimental treatment, the participants were allowed rescue with their usual anti-migraine medication or over-the-counter analgesics but not before 2 h after placebo or sumatriptan. During the study, an emergency phone was always open where patients could call if they experienced severe headaches or discomfort.
Headache parameters: Headache parameters and accompanying symptoms were recorded by the investigator at baseline on a headache questionnaire. Afterward, headache intensity, characteristics (unilateral/bilateral, quality and aggravation by physical activity), accompanying symptoms (nausea/vomiting, phono- and photophobia) and side effects were scored on a self-administered questionnaire. The patients had to fill out the questionnaire every 30 min for the first 6 h after cilostazol and thereafter every hour until 12 h after cilostazol. The intensity was scored on an NRS from 0 to 10, 1 representing a very mild headache (including a feeling of pressing or pulsation), 5 a headache of medium severity, and 10 the worst possible headache.
Missing data were filled in using last observation carried forward.
The following criteria were used for a migraine-like attack induced 0–12 h after administration of cilostazol:
Headache fulfilling criteria C and D for migraine without aura according to the IHS criteria (12).
C. Headache has at least two of the following characteristics:
Unilateral location Pulsating quality Moderate or severe pain intensity (moderate to severe pain intensity is considered ≥4 on NRS) Aggravation by cough or causing avoidance of routine physical activity
D. During headache at least one of the following:
Nausea and/or vomiting Photophobia and phonophobia.
Statistical analysis: Calculation of sample size was based on the detection of a difference in headache intensity between two experimental days, at 5% significance with 90% power. We estimated that placebo had an effect on 20% of patients and sumatriptan had an effect on 60%. Standard deviation was estimated based on previous data. The correlation between the 2 days was estimated conservatively at 0.5. We also assumed no carry-over effect. We calculated that at least 18 participants should complete both study days. Due to uncertainty regarding these assumptions we decided to include 30 participants. The area under the curve (AUC) for headache score was used as a summary measure for analyzing differences between the groups and was calculated according to the trapezium rule (13). Our primary endpoints were a) difference in median headache intensity between the sumatriptan day and the placebo day at 2 h after treatment, and b) difference in AUC 0–4 h post treatment between the two study days. Secondary endpoints were difference in pain intensity difference (PID) between the sumatriptan day and the placebo day (PID is the difference in pain intensity at the various time points versus baseline. This will take headache score at time of treatment into account (headache score varied from 2 to 6 with a median headache score at 4)), difference in median peak headache score, difference in median headache intensity at 4 h after treatment between the two study days, AUC 0–2h post treatment after sumatriptan/placebo and accompanying symptoms such as nausea, photo- and phonophobia.
We chose our endpoints prior to study start. We chose reduction in headache score at 2 h as our primary endpoint, instead of pain freedom (FDA guidelines) since cilostazol is present in the body for many hours and thus it is unlikely to gain complete reduction of headache score after 2 h. Because the effect of sumatriptan is higher at 4 h than at 2 h, we also included AUC 0–4 h post treatment as a primary endpoint.
Headache intensity scores are presented as medians (range). Differences in AUC for headache scores were tested using the Wilcoxon signed rank test. Difference in pain intensity difference between the sumatriptan day and the placebo day were also tested using the Wilcoxon signed rank test. The incidence of headache and associated symptoms were analyzed as binary categorical data with McNemar’s test. Age and weight are presented as means. All analyses were performed with GraphPad Prism version 7.0.
A p value < 0.05 was considered significant.
Results
Thirty patients with episodic migraine without aura (25 female, five males) completed both study days. Mean attack frequency of spontaneous attacks was two per month (range, one attack every 3rd month to six attacks per month). Mean age was 30.8 years (range 20–59 years) and mean weight was 69 kg (range 60–92 kg). Sixteen participants were known triptan responders and 14 participants were triptan naïve. None of the participants used preventive migraine treatment.
Characteristics of the induced headache
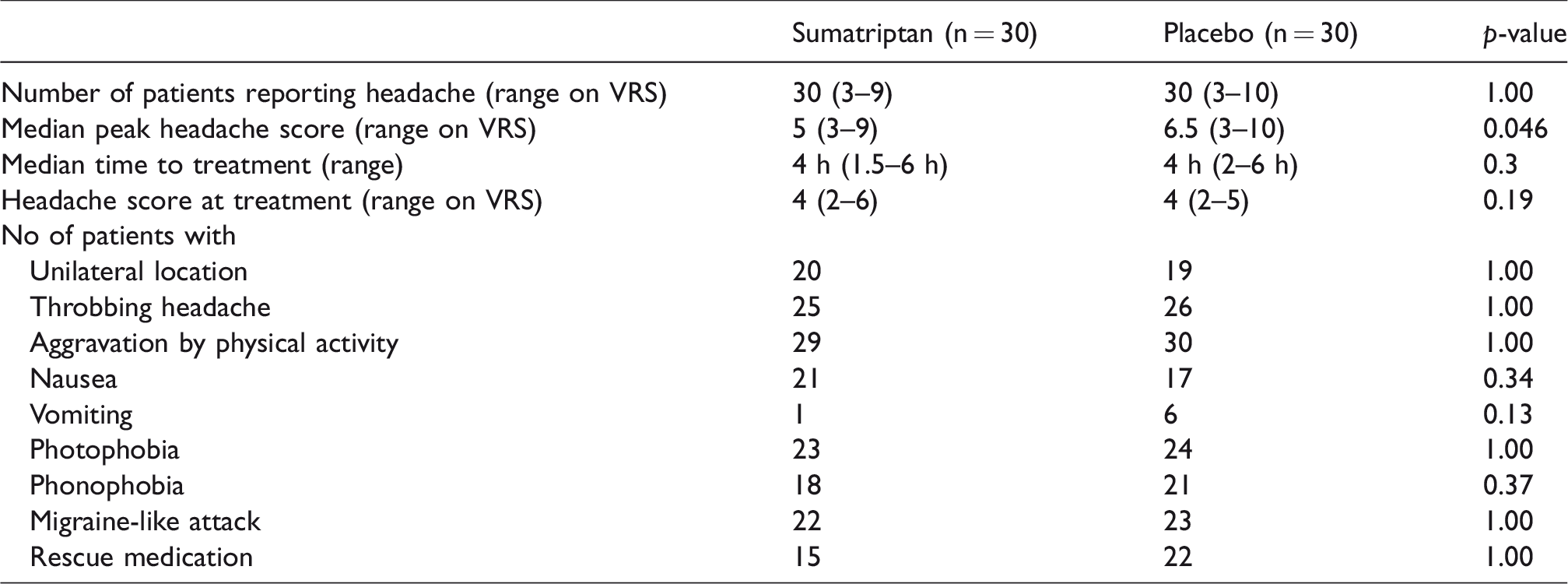
Cilostazol induced a headache in all 30 patients on both provocation days (range 3–10 on NRS). Median peak headache score was 5 on the sumatriptan day and 6.5 on the placebo day (p = 0.046, secondary endpoint).
The induced headache had several migraine features (see Table 1) and cilostazol induced migraine-like attacks in 22 patients (73%) on the sumatriptan day and in 23 patients (77%) on the placebo day. Median time for migraine-like attacks was 3.5 h on the sumatriptan day and 4 h on the placebo day (range 1–10h). Eighteen patients fulfilled the criteria at time of treatment on the sumatriptan day and 17 did on the placebo day. There was no difference between the two study days in headache characteristics or accompanying symptoms (Table 1).
Headache intensity, headache characteristics and accompanying symptoms on the two study days.
The effect of sumatriptan on the induced headache
The patients received treatment (sumatriptan or placebo) when they reached a headache score at 4 on NRS or at 6 h after cilostazol if they did not reach this severity of headache. Median time to treatment was 4 h in both groups (range 1.5–6 h, Table 1). Median headache score at the time of treatment was 4 in both groups (range 2–6, Table 1). Figure 1 illustrates median headache score 0–6h after treatment on both days.

Median headache score on the sumatriptan day and the placebo day 0–6 h after treatment. The thin dotted lines represent median time of rescue medication.
Our primary endpoint, difference in median headache score 2 h after treatment between the 2 days, was statistically significant (p = 0.01, Figure 2). The difference at 4 h became even more significant with a p-value of 0.0007 (secondary endpoint, Figure 2). The reduction in headache score on the sumatriptan day from 0 h to 2 h was also significant (p = 0.0003). Our other primary endpoint, difference in AUC 0–4 h post treatment between the two study days was also significant (p = 0.01, Figure 3).

Median headache score at different timepoints after treatment. There was a significant difference in headache score between the sumatriptan day and the placebo day at both 2 h (p = 0.01) and 4 h (p = 0.0007). The reduction in headache score on the sumatriptan day from 0 h to 2 h was also significant (p = 0.0003).

The area under the headache score curve 0–4 h after treatment with sumatriptan and placebo. The difference between the two days was significant (p = 0.01).
We found a highly significant difference at both 2 h (p = 0.0017) and 4 h (p < 0.0001) in our secondary endpoint: Difference in pain intensity (difference in delta headache scores) between the sumatriptan day and the placebo day. However, there was no difference in our other secondary endpoint AUC 0–2 h post treatment (p = 0.22).
Post-hoc analyses showed that there was no difference in treatment response between known triptan responders and triptan naïve patients, between the two genders or between patients who fulfilled the criteria for a migraine like-attack and those who did not.
The patients were allowed to take rescue medication (their usual migraine treatment or over-the-counter drugs) 2 h after the “study-treatment” (sumatriptan or placebo). Fifteen patients did so on the sumatriptan day and 22 did on the placebo day. Median time to rescue medication was 10.5 h after cilostazol on the sumatriptan day and 8.5 h after cilostazol on the placebo day (range, 4–12 h), Figure 1.
Other side effects 0–12 h after cilostazol
In addition to the symptoms described in Table 1, the participants registered the following side effects during the study (Table 2).
Side effects reported by the participants in the questionnaire, 0–12 h after cilostazol.

Discussion
Our study confirmed that cilostazol is a highly efficient headache- and migraine-provoking substance. Subcutaneous sumatriptan significantly decreased the induced headache compared to placebo and, thus, the cilostazol model responds to migraine-specific treatment.
Cilostazol–induced migraine
In our study, 18 patients fulfilled the criteria for a migraine-like attack at time of treatment on the sumatriptan day, and 17 patients did so on the placebo day. The rest of the patients experienced a headache with several migraine characteristics; a further four patients developed an attack after administration of the treatment on the sumatriptan day and six patients did so on the placebo day. The development of a migraine attack is an ongoing process, and we believe that genuine migraine mechanisms were activated by cilostazol. Other studies have found a migraine induction of 86% in MO patients (5,6) and perhaps more patients would have developed an attack in our study if the treatment had been further postponed.
However, we cannot be completely sure that cilostazol does not also induce another type of headache than migraine. Other migraine-provoking substances such as CGRP and GTN induce a two-phase headache with an initial mild (maybe vasodilatory) headache, which diminishes but is followed by a migraine-like attack (3,14). Perhaps cilostazol also induces an initial vasodilatory headache and a delayed migraine with no headache-free phase in between.
Response of the induced headache to sumatriptan
We found a significant reduction in headache score 2 h after sumatriptan and a significant difference in treatment response between sumatriptan and placebo.
Our own previous studies showed that sumatriptan tablets only had a trend of efficacy in the same study design (7–9). Thus, when sumatriptan is administered as subcutaneous injections it becomes more powerful. The same phenomenon is seen when treating spontaneous attacks, where subcutaneous sumatriptan is also more efficient than oral sumatriptan (11). This mechanism is not completely clarified but is probably explained by the fast peak in plasma concentration after the injections.
Clinical migraine trials define a sufficient treatment response as a 50% reduction in headache score 2 h after treatment. In our study, the median headache score was only reduced from 4 on NRS at the time of treatment to 2.75 on NRS (corresponding to 31% reduction) at 2 h after treatment. Trials treating spontaneous attacks with subcutaneous sumatriptan showed a decrease from moderate-severe to mild or no headache already within the first hour after treatment (15) but this was not observed in the present study. Hence, we do not see quite as good effect on cilostazol induced headache as on spontaneous migraine attacks. This was expected before study start because the migraine-generating properties of cilostazol are ongoing for more than 12 h. Therefore, we chose reduction in headache score at 2 h (difference between the sumatriptan day and the placebo day) instead of total pain relief as one of our primary endpoints.
In addition to the ongoing migraine generation after cilostazol, another explanation of the modest effect of sumatriptan (both tablets and injections) could be that sumatriptan acts on the cell membrane whereas cilostazol acts intracellularly. Since we do not measure the cellular response in our study, this is only speculation. Another hypothesis is that our study and previous studies using Nitric oxide (NO) donors (described below) indicate that when the intracellular level of second messenger molecules such as cyclic adenosine monophosphate (cAMP) and cyclic guanosine monophosphate (cGMP) are high at time of treatment, sumatriptan cannot exert its effect properly. The explanation could also be that cilostazol bypasses sumatriptan in the migraine cascade, and thus generates migraine downstream from sumatriptan’s site of action.
Sumatriptan disrupts the migraine generating process during spontaneous attacks, but during migraine induced by cilostazol it can only counteract the process to some degree. The mechanisms behind this are complex and might not be explained by a single mechanism.
If cilostazol induces an initial vasodilatory headache, we cannot rule out that some of the treated headaches in our study were not converted into migraine at time of treatment, and thus we might have treated vasodilatory headache. However, in a post-hoc analysis we found no difference in response between patients who fulfilled the criteria for a migraine-like attack and those who did not.
Other provocation studies have given sumatriptan after cilostazol induction in an open label fashion. One study used sumatriptan in tablet formulation (5) and the other study used subcutaneous sumatriptan (16). Both studies reported over 50% reduction in headache intensity 2 h after treatment (tablets: From 6 to 2 on NRS. Subcutaneous: from 7 to 3 on NRS) (5,16). Since all patients in these studies knew that they were given an effective anti-migraine drug, we suggest that the bigger reduction in headache intensity, as compared to the present study, is a result of the combination of drug effect and placebo effect.
We found no difference in migraine induction between the two study days (73% on the sumatriptan day and 77% on the placebo day). This is probably because migraine induction already occurred at 3.5 h (sumatriptan day) and 4 h (placebo day) after cilostazol and hence before administration of treatment (median 4 h).
Rescue medication
Median time to rescue medication was 10.5 h after cilostazol on the sumatriptan day (corresponding to 6.5 h after sumatriptan administration) and 8.5 h after cilostazol on the placebo day (corresponding to 4.5 h after placebo), Figure 1.
Fifteen patients took rescue medication on the sumatriptan day (six patients took sumatriptan, five took an NSAID, three took Treo and one took paracetamol). Ten out of the 15 patients did not have any initial effect on headache score after sumatriptan and their headache had increased (or stayed the same) from time of sumatriptan to time of rescue medication. These 10 patients had a median headache score of 6.5 at time of rescue medication. The last five patients had an initial reduction of headache score from sumatriptan. Their headache was reduced at time of rescue medication (to median headache score 2) compared to time of sumatriptan (median headache score 4).
The 10 patients who did not have an initial effect from sumatriptan had no special characteristics. Both genders were represented, there was no difference in family disposition to migraine, five patients did and five did not fulfill the criteria for a migraine-like attack at time of treatment, and the group included six known triptan responders and four who were triptan naïve.
The use of rescue medication on the sumatriptan day was thus not because of a recurrence of headache, but rather an insufficient initial response of sumatriptan (or a continuous mild headache). The demographic could not explain the lack of effect in this group. It would be interesting to examine these patients further using, for example, RNA sequencing during provoked and treated attacks.
On the placebo day, 22 patients took rescue medication (nine patients took triptans, nine took NSAID, two took Treo and two took paracetamol. In addition, many patients supplemented the initial treatment with, for example, paracetamol). Nineteen of the 22 patients had no initial effect of placebo treatment and their headache increased or stayed the same from time of placebo to time of rescue medication. Their median headache score was 7 at time of rescue medication. Three patients had an initial effect of placebo and their headache score was only 3 at time of rescue medication.
Is cilostazol–induced headache a useful model for future drug testing?
The CGRP and GTN models have been extensively studied and are both well-established migraine models. The GTN model has previously been used as an attempt to develop a model for drug-testing. The model has shown some utility, but with mixed results: Propranolol (17) and tonerbasat (18) as pre-treatment did not reduce GTN-induced headache. Valproate (19) and prednisolone (20) pre-treatment showed positive results, as did pre-treatment with 6 mg subcutaneous sumatriptan (21). When GTN-induced headache was fully developed, it did not respond to aspirin or zolmitriptan (22). Another study tried to modify the GTN model and used an oral NO donor, isosorbide-5-mononitrate (5-ISMN). The 5-ISMN induced headache did not respond to oral sumatriptan treatment (23). The CGRP model cannot be used to test new drugs either, since a study showed that pre-treatment with sumatriptan did not antagonize any CGRP-induced symptoms (24).
Even though the GTN model has shown some utility for drug testing, we chose to modify the model using cilostazol instead. Cilostazol is a more powerful migraine inducer than both GTN and CGRP, with an induction potential of 86% in MO patients (5), compared to 80% (GTN) (14) and 30–75% (CGRP) (3,25,26). Furthermore, cilostazol has been shown to have a 100% reproducibility in migraine induction (6). But most importantly, GTN and CGRP are administered intravenously, complicating the study design, in contrast to cilostazol which is a tablet formulation and thus makes the study very pragmatic.
In our aim to develop a model for drug testing using cilostazol, we optimistically started out with sumatriptan tablets as treatment in healthy volunteers but with a negative result (9). Next, we pre-treated with tablets to compensate for slow onset of the effect of the tablets – the headache was prevented from developing as intended, but the induced headache was too mild on the placebo day to see a difference between the days (8). Then we used tablets in MO patients with a trend of efficacy (7). Finally, we have now used a less pragmatic design with sumatriptan injections in MO patients, which significantly decreased the headache score at both 2 h and 4 h after treatment.
The model has thus been validated, but is it a useful model for novel drug testing? We have shown that sumatriptan injection decreases headache score significantly in a study population of 30 participants. This is not a large sample size to test the effect of acute migraine treatments. Thus, the standardized setup compensates for the somewhat smaller effect size as compared to spontaneous migraine attacks.
We believe that we have developed a model that could be used as a screening tool to test if a new drug has potential as a migraine drug. One should not expect complete reduction in headache score because of the ongoing migraine-generating effect of cilostazol. If the new drug shows just some efficacy in the cilostazol model, there is a strong chance that the drug will have a very good effect in spontaneous attacks.
There are several advantages of the model. If a company/research group already has enough paid volunteer migraine patients, then the recruitment time is short and, more importantly, completion time will be short. Furthermore, the standardized experimental model allows close monitoring of safety, pharmacokinetics and, if relevant, even neuroimaging. Thus, a wealth of information can be collected in addition to the therapeutic response.
If new test drugs act intracellularly or deeper in the cascade of migraine mechanisms than sumatriptan, it seems likely that the effect size would be larger and that the cilostazol model will be more powerful. For example, it is predicted that the model will be excellent for testing new drugs acting on ion channels. It must be up to pharma companies to decide if they want to test their new drugs in a fast and standardized setting via our experimental model or if they want to rely only on clinical trials, as they do today.
Perspectives
Our own group has previously shown that pre-treatment with sumatriptan tablets prevented cilostazol induced headache in healthy volunteers (8). However, the placebo group did not develop much headache either, and thus the results were not statistically significant. One could modify the pre-treatment model by taking the lower headache induction in a pre-treatment design into account; for example, by increasing the number of subjects. The model could also be modified using other migraine-provoking substances than cilostazol, such as PACAP-38, levcromakalim, histamine and sildenafil. Modifications of the existing GTN model might also be useful. One could also use another migraine abortive treatment as the validating drug; for example, the new CGRP antibodies.
Conclusion
Subcutaneous sumatriptan reduced cilostazol induced headache in MO patients compared to placebo. We suggest that the drug industry can use the cilostazol model in MO patients to test new drug candidates for migraine, especially if the drugs acts deeper in the migraine cascade than sumatriptan.
Strengths and limitations
We were limited to choosing a specific time of treatment that was a trade-off between treating early enough, where sumatriptan is most effective, and not treating before the migraine cascade was triggered. Regarding the usefulness of our model, it is a limitation that we had to give sumatriptan as injections. Tablet formulation would have been preferred, but we have previously shown that this did not work. The headache response was self-reported, and it would have been better to have kept the participants in the laboratory; however, this was not feasible.
The strengths of our study are a robust study design with standardized circumstances regarding room, equipment, time of day and trained staff, in addition to a randomized, double-blind, placebo-controlled cross-over design.
To develop a model for drug testing, we must keep in mind that migraine is a heterogenic disease and thus has unclarified pathophysiological mechanisms. Hence, the development and biological mechanisms of new migraine treatments is also complex, and maybe several models for migraine drug testing are needed.
Impact of the study findings
We believe that we have developed a human model that the drug industry can use as part of a program to test new potential migraine drugs. Our model can save the drug industry both time and money and hopefully it will promote the development of new anti-migraine drugs.
Clinical implications
Subcutaneous sumatriptan reduces cilostazol induced headache in MO patients. The cilostazol model is a useful model for the drug industry to test new drug candidates in the future.
Footnotes
Acknowledgement
We thank all the volunteer migraine patients who participated in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Candys Foundation and Lundbeck Foundation.