
Abstract
Background and purpose
It is sometimes difficult to diagnose intracranial vertebral artery dissection in patients with headache as the only symptom. Knowledge of the characteristics of the headache would facilitate the diagnosis. In this study, we aimed to clarify the characteristics of intracranial vertebral artery dissection-related headache using our original self-administered questionnaire.
Methods
Via the questionnaire, we ascertained headache characteristics and investigated whether they differed between two types of unruptured intracranial vertebral artery dissection, headache type and ischemic type, based on analysis of the responses. Then, we tried to validate the consistency of commonly used criteria for intracranial artery dissection by comparing them with our results.
Results
Thirty-seven patients were analyzed. Our results identified the following seven headache characteristics in patients with intracranial vertebral artery dissection: (i) occurring in the occipitonuchal region (89%); (ii) unilateral (81%); (iii) pulsatile (70%); (iv) of acute onset (70%); (v) severe (73%); (vi) without nausea or vomiting (73%); and (vii) with concomitant clinical symptoms unrelated to ischemia (81%). Comparison of headache characteristics between the two types of intracranial vertebral artery dissection headache showed that the pain was significantly more severe in headache type than ischemic type intracranial vertebral artery dissection (p = 0.01). Concomitant clinical symptoms occurred significantly more often in ischemic type than headache type intracranial vertebral artery dissection (p = 0.03). Our results generally satisfied the established headache diagnostic criteria.
Conclusion
The pain characteristics of headache type and ischemic type intracranial vertebral artery dissection shown in our study may facilitate its diagnosis.
Keywords
Introduction
Spontaneous cervicocephalic arterial dissection is well known as an important cause of stroke in young adults (1–5). There are known ethnic differences in the affected arteries: internal carotid artery dissection (ICAD) is common in Caucasian populations, whereas vertebral artery dissection (VAD) is more common in Asian populations (2,6–8). Moreover, the frequency of intracranial VAD (IC-VAD) has been reported to be up to three- to 10-fold greater than that of extracranial VAD in Asian populations (2,6–8). Hence, the majority of cervicocephalic arterial dissections in Asia are IC-VAD. It is well known that headache is the most common initial symptom in patients with IC-VAD (6,9–13). IC-VAD is divided into three types based on the clinical symptoms: hemorrhagic type, ischemic type and headache type (14). In hemorrhagic type, or ruptured IC-VAD, the headache characteristics conform to those of subarachnoid hemorrhage. On the other hand, the headache characteristics of unruptured IC-VAD (i.e. ischemic and headache types) are not well known, and it is difficult to diagnose IC-VAD in patients presenting with only headache to the outpatient clinic or emergency department (6,9,10,15). The fact that it takes a long time to diagnose this condition also reflects the difficulty in its diagnosis (6,16). Understanding the headache characteristics would, thus, facilitate the diagnosis. However, only a few reports have focused on the characteristics of unruptured IC-VAD-related headache. Moreover, questions remain regarding whether the headache characteristics are the same or different between ischemic and headache type IC-VAD because no previous report has investigated the differences in headache characteristics between these two types of IC-VAD.
When patients presenting with headache are evaluated, physicians usually use The International Classification of Headache Disorders, 3rd edition (beta version) (ICHD-3 beta) to diagnose the cause (17). However, since the ICHD-3 beta clubs together the criteria for diagnosis of all types of intracranial artery dissection, there are no specific criteria for IC-VAD. The Clinical Practice Guideline for Chronic Headache 2013, which was published by the Japanese Headache Society, also lists together the headache characteristics of all types of intracranial artery dissection (18). However, since intracranial ICAD and IC-VAD differ in their pathophysiology (16), their headache characteristics are also likely to be different. Thus, the reliability of these guidelines may be low.
In this study, we aimed to clarify the headache characteristics of unruptured IC-VAD by using our original self-administered questionnaire. We also investigated whether headache characteristics differ between the two types of unruptured IC-VAD. Finally, we tried to validate the consistency of the criteria for intracranial artery dissection in the ICHD-3 beta and Clinical Practice Guideline for Chronic Headache 2013 by comparing them with our results.
Methods
This study was approved by the institutional review board of Eishokai Yoshida Hospital. The prospectively maintained database of our hospital was searched for patients with unruptured intracranial VAD between January 2011 and June 2017. Their medical records and radiographic studies were reviewed retrospectively.
Definition of unruptured intracranial VAD
We diagnosed IC-VAD by magnetic resonance imaging (MRI), such as 3-dimensional time-of-flight MR angiography and basi-parallel anatomical scanning. Unruptured IC-VAD cases were divided into two types: ‘headache type’ and ‘ischemic type’. Headache type was defined as cases presenting with only headache during the entire clinical course, while ischemic type was defined as cases presenting with ischemic symptoms with or without cerebral infarction on MRI during the clinical course. Hence, patients presenting with transient ischemic attack were included in the ischemic group.
Study design
Our original self-administered questionnaire.

Definition of headache intensity
We investigated headache intensity in Q5. Headache intensity, which was measured using a Numerical Rating Scale (NRS), was classified as mild (NRS = 1–3), moderate (NRS = 4–6), and severe (NRS = 7–10).
Definition of concomitant clinical symptoms with the headache
We investigated the presence of concomitant clinical symptoms besides headache in Q8. Clinical symptoms due to ischemia, such as visual field defects, dysarthria, double vision, ataxia, vertigo, and hemiparesis, which could have been indicative of ischemia, were excluded. We selected items such as irritated eyes, giddiness, transient dysesthesia, listlessness, fever, and neck stiffness. We selected these items based on a medical interview with the patients at the time of the initial visit.
Patient population
We treated 63 patients for unruptured IC-VAD at our institution between January 2011 and June 2017. All cases had unilateral lesions. We sent the questionnaire by mail to these 63 patients. Thirty-nine patients (61%) returned the completed questionnaire. Among these 39 patients, two patients with ischemic type IC-VAD responded that they had no headache and so were excluded. The interval between diagnosis and the current investigation ranged from 1 to 78 months (mean 38.6 months, median 43 months). Finally, 37 patients (59%) were analyzed (Figure 1).
Flow chart showing patient selection.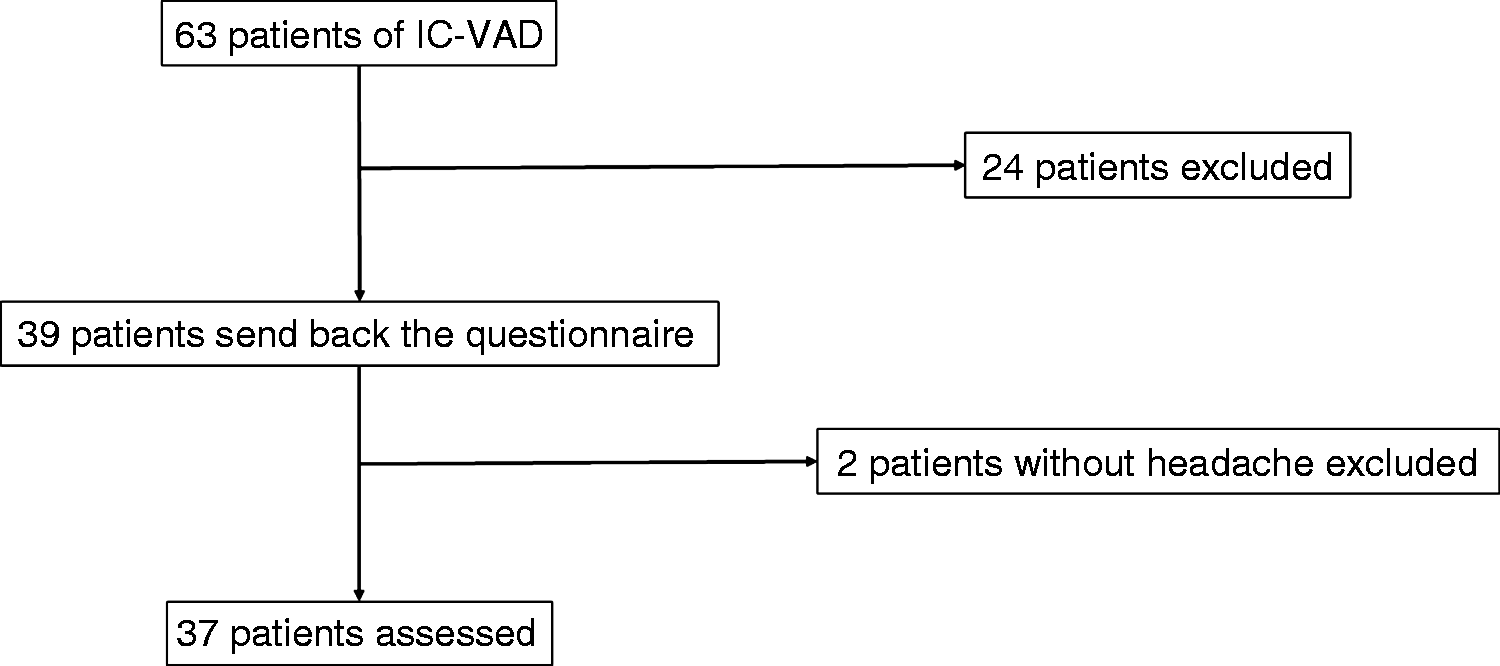
Scoring system for diagnosis of the headache of unruptured IC-VAD
We attempted to establish a scoring system for diagnosis of the headache. We considered items with either a positive or negative response rate of over 65% as the headache characteristics. We scored each characteristic as 1 point and investigated the total score in each patient.
Statistical analysis
To compare the headache characteristics between headache type and ischemic type IC-VAD, statistical analysis was performed using the Student's t-test, Mann–Whitney U-test, or chi-squared test of independence. Differences were considered significant for probability values of p < 0.05. All statistical analyses were performed using Statcel software, version 4 (OMS Publishing, Saitama, Japan).
Results
Summary of the clinical characteristics of patients with ischemic type intracranial vertebral artery dissection.
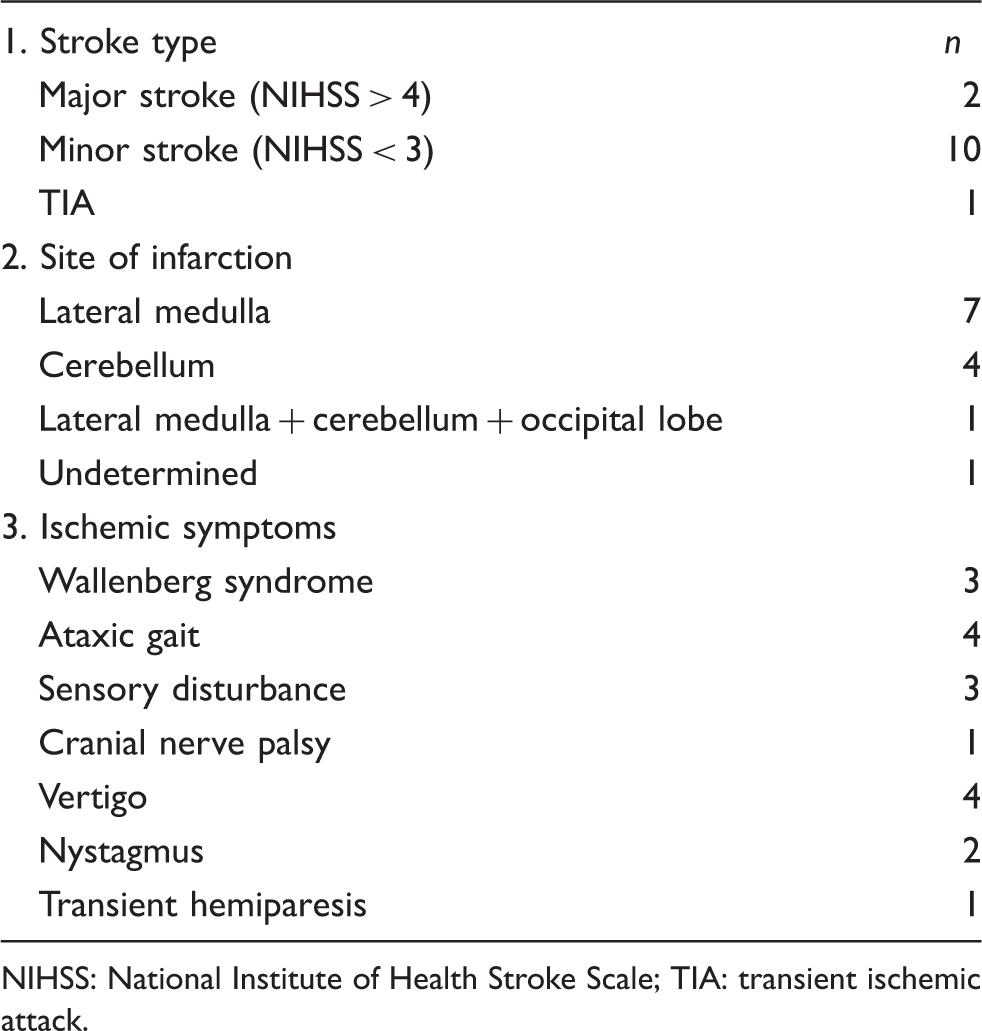
NIHSS: National Institute of Health Stroke Scale; TIA: transient ischemic attack.
General characteristics of headache due to unruptured IC-VAD
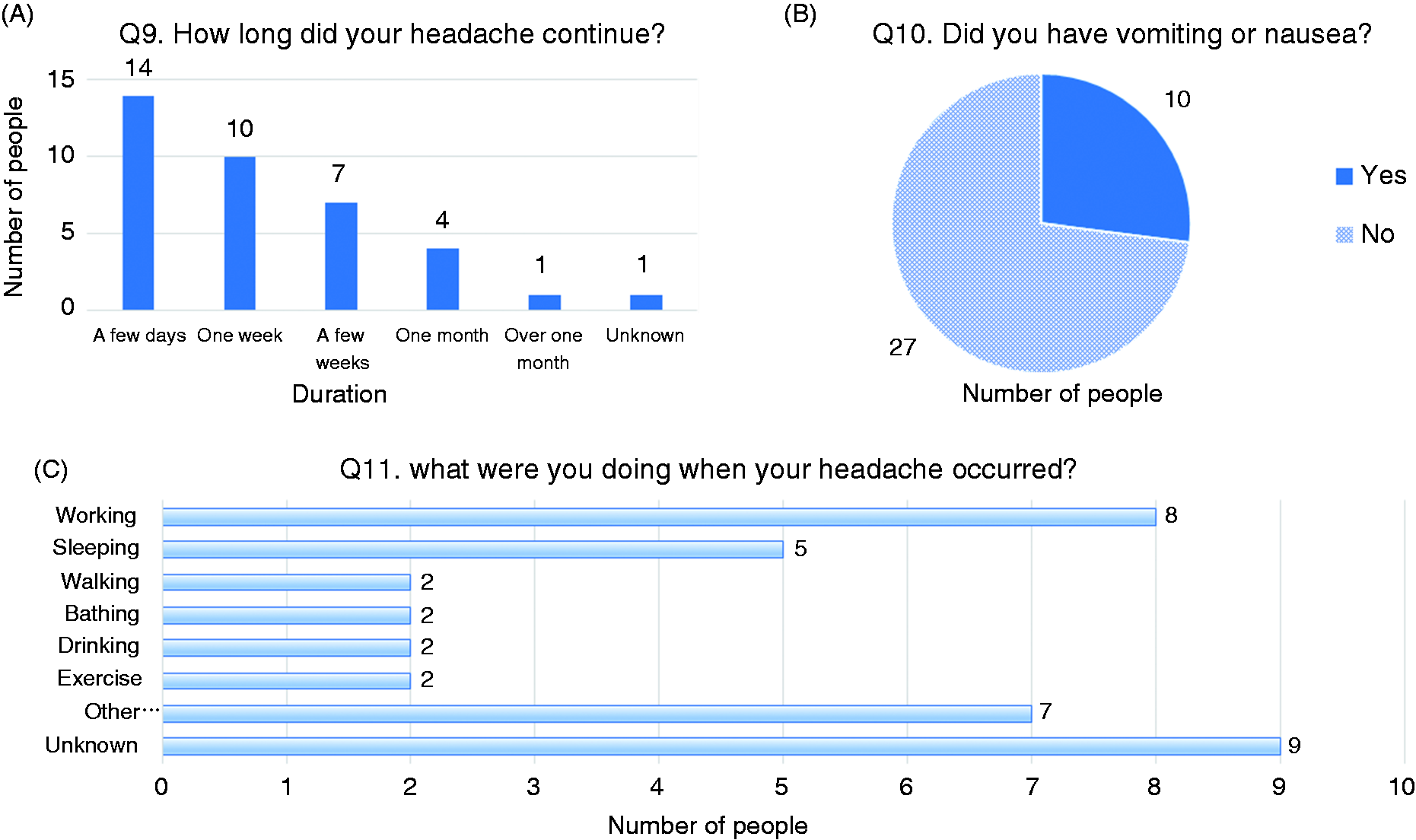
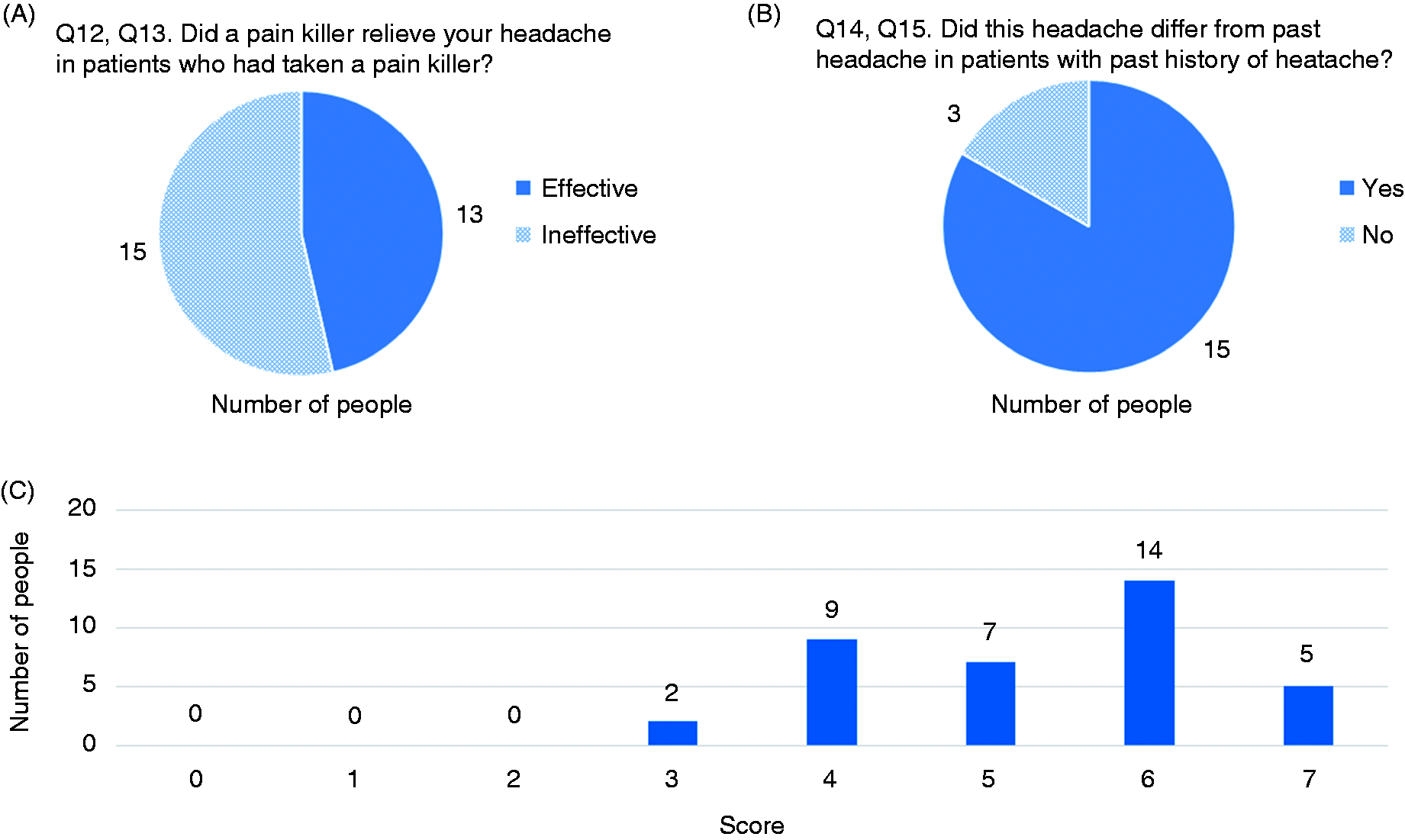
Headache occurred mainly in the occipitonuchal region (33/37, 89%), and spread to the temporal and parietal regions, forehead, and face (Figure 2A). However, some patients (4/37, 11%) did not have posterior headache, and instead had pain in the temporal region (n = 3) or the face (n = 1). Headache was mainly unilateral (30/37, 81%; Figure 2B). The rate of headache ipsilateral to the IC-VAD was 65% (24/37). The pain was most frequently described as pulsatile (26/37, 70%), followed by dull (4/37, 11%), constrictive (3/37, 8%), burning (2/37, 5%), and electrical (2/37, 5%) (Figure 2C). Most of the patients (26/37, 70%) had acute onset headache (Figure 3A). Twenty-four of 37 patients (65%) answered that it was the worst pain they had ever felt and 27/37 (73%) rated the pain intensity as severe (Figure 3B and 3C). Fifteen of 37 patients (41%) had aggravating factors for the pain, body motion being a major factor (Figure 4A). Thirty of 37 patients (81%) had concomitant clinical symptoms when the headache occurred, among which neck stiffness was most common (Figure 4B). In almost all patients (35/36, 97%), headache resolved within 1 month of its onset. Duration of headache in the remaining one patient was unknown (Figure 5A). Most of the patients did not have accompanying nausea or vomiting (27/37, 73%, Figure 5B). Although headache usually occurred while the patients were awake (19/28, 68%), some patients developed headache while sleeping and were woken up by the pain (5/28, 18%). On the other hand, the time of onset of the pain in the remaining nine patients was unknown (Figure 5C). Twenty-eight of 37 patients took painkillers. The number of patients who responded to painkillers was almost the same as those who did not experience a response (effective: 13/28, 46%, ineffective: 15/28, 54%) (Figure 6A). Although 18 of 37 patients (49%) had a previous history of headache, 15 of them (83%) answered that the present headache was different from their previous headache (Figure 6B).
Results of the questionnaire: (A) Q1; (B) Q2; (C) Q3. Results of the questionnaire: (A) Q4; (B) Q5; (C) Q6. Results of the questionnaire: (A) Q7; (B) Q8. Results of the questionnaire: (A) Q9; (B) Q10; (C) Q11. Results of the questionnaire: (A) Q12 and 13; (B) Q14 and 15; (C) patient scores in our scoring system based on the headache characteristics demonstrated by our patients.


Comparison of headache characteristics between headache type and ischemic type IC-VAD
Comparison of the characteristics of the headache between the two types of unruptured intracranial vertebral artery dissection.

IC-VAD: intracranial vertebral artery dissection; NRS: Numerical Rating Scale.
aStudent's t-test; bchi-squared test for independence; cMann–Whitney U-test.
Validation of the consistency of previous diagnostic criteria for intracranial artery dissection by comparing them with our results
Diagnostic criteria in the ICHD-3 beta and Clinical Practice Guideline for Chronic Headache 2013 and their consistency relative to the criteria in our study.

ICHD-3 beta: The International Classification of Headache Disorders, 3rd edition (beta version).
Scoring system for diagnosis of the headache of unruptured IC-VAD

Discussion
Recently, the detection and diagnosis of unruptured IC-VAD has increased due to advancements in MRI (19,20). A Japanese nationwide study on IC-VAD reported that unruptured IC-VAD accounted for 69.5% of IC-VAD cases (14). In that study, among the unruptured IC-VAD, 47.6% of cases were of the ischemic type and 52.4% of cases were of the headache type. In ischemic type IC-VAD, 56.9% of the cases presented with headache (14). Thus, the majority of unruptured IC-VAD cases experience headaches.
Pain caused by cervicocephalic arterial dissection is thought to be referred pain associated with the nerves innervating the vessels (9,18). The sites of headache and neck pain differ depending on the dissected vessels. In dissections in the vertebro-basilar arterial system, unilateral cervical pain and occipital pain are frequent. These pains can be triggered by stimulation of the artery. Nichols et al. (21) reported that balloon angioplasty in the vertebro-basilar arterial system caused localized ipsilateral occipital and posterior cervical pain. Hence, headache in the occipitonuchal region is considered as the major clinical symptom of IC-VAD.
Characteristics of unruptured IC-VAD-related headache
Our study showed that the characteristics of headache due to unruptured IC-VAD are as described below: (i) presenting in the occipitonuchal region (89%); (ii) unilateral (81%); (iii) pulsatile (70%); (iv) of acute onset (70%); (v) severe (73%); (vi) with no associated nausea or vomiting (73%); and (vii) with the presence of concomitant clinical symptoms (81%). Further, the headache resolved within 1 month of its onset in almost all our patients. Several previous reports have investigated the characteristics of headache due to unruptured IC-VAD (6,9,10). Their results almost completely corresponded with our results in terms of the headache characteristics. Kim et al. (6) reported that headache that is exacerbated or attenuated by head motion or a specific head position is a specific feature of extracranial VAD. However, this feature is not described in other reports, including in the ICHD-3 beta. Our results showed that 15 patients (40%) had factors that aggravated the pain. Although body motion exacerbated the headache in 10 patients, the headache was not exacerbated by head motion in any of our patients.
On the other hand, in our study, 30 patients (81%) had concomitant clinical symptoms when the headache occurred. This feature has not been described in previous reports. Since IC-VAD can cause ischemia in the posterior circulation, ischemic symptoms, such as visual disturbances, vertigo, ataxia, and sensory disturbances, can accompany the headache. However, the associated clinical symptoms in this study were unlikely to have been ischemic symptoms. Although the mechanisms of these clinical symptoms are unclear, asking patients about these symptoms might aid in the diagnosis of unruptured IC-VAD.
Differences in headache characteristics between the two types of unruptured IC-VAD
Our results showed that intensity of the headache in headache type IC-VAD was significantly more severe than in the ischemic type. Moreover, the number of patients describing the headache as the worst they had ever felt was significantly more in the headache type IC-VAD than in the ischemic type. Since headache intensity was measured by the patient's subjective assessment, concomitant ischemic symptoms might have masked the headache intensity in patients with ischemic type IC-VAD. On the other hand, concomitant clinical symptoms other than ischemic symptoms were observed significantly more often in patients with ischemic type than in headache type IC-VAD. However, over 70% of patients with headache type IC-VAD also showed concomitant clinical symptoms. Hence, the presence of concomitant clinical symptoms is a common characteristic in both types of dissection, despite the statistically significant difference.
Validation of the consistency of previous diagnostic criteria of intracranial artery dissection by comparing them with our results
The headache characteristics of unruptured IC-VAD shown by us corresponded mostly with those shown in ICHD-3 beta; each criterion of duration, intensity, and laterality was satisfied in over 65% of our patients. However, the mode of onset criteria may be controversial. In ICHD-3 beta, the mode of headache onset is described as ‘sudden or thunderclap onset’ (17). On the other hand, in the Clinical Practice Guideline for Chronic Headache 2013, ‘acute onset headache’ is cited as being characteristic (18). This raises the question as to whether the major mode of onset is ‘sudden’ or ‘acute’. Strictly speaking, ‘sudden onset headache’ means head pain reaching maximal intensity within seconds to a minute. On the other hand, ‘acute onset headache’ means head pain reaching maximal intensity within a few to several tens of minutes. Our results showed that 70% of the patients had acute onset headache. Maruyama et al. (9) also reported that 80% of their patients had acute onset headache. Kim et al. (6), who also validated the ICHD-3 beta criteria, showed low consistency in mode of onset criteria (7.1%). Their results showed that the headache in most patients had an acute onset (79%), and they suggested that inclusion of ‘acute onset’ should be considered to achieve better criteria performance. Strictly speaking, ‘acute’ and ‘sudden’ onset represents a different time course. However, the fine distinction between ‘acute’ and ‘sudden’ onset may make its differentiation based only on medical interviews difficult. If the question regarding mode of onset focuses on whether the onset was gradual or not, the description ‘acute or sudden onset’ may be suitable. Hence, we also suggest including ‘acute or sudden onset’ in the criteria.
In the Clinical Practice Guideline for Chronic Headache 2013, mode of onset, laterality, and pain intensity are combined as general headache characteristics (18). However, location and duration are independent characteristics. Our results showed that only 35% of our IC-VAD cases satisfied these general headache characteristics. However, the characteristics of location and duration were satisfied by 89% and 97% of the patients. When the general headache characteristics were considered separately, the criteria of mode of onset, laterality, and pain intensity were satisfied by 70%, 65%, and 73% of IC-VAD cases. Hence, our results indicate that the description of headache characteristics should probably be subdivided to increase the accuracy of the diagnostic criteria like ICHD-3 beta.
Differentiation of IC-VAD headache from primary headaches
It is very important to differentiate headache due to IC-VAD from primary headaches such as migraine, tension-type headache or cluster headache (6,17). In general, severe and unusually persistent occipitonuchal pain is suggestive of intracranial VAD. However, headache due to IC-VAD without neurological signs are often misdiagnosed as tension-type headache because tension-type headaches commonly occur in posterior locations (6,15). Severe and pulsatile headache in the occipitonuchal region may be misdiagnosed as atypical migraine. Our results showed that some patients had headache in the temporal region or face. In such cases, physicians may suspect migraine or cluster headache. Moreover, the diagnosis is even more difficult when patients with a past history of headache develop IC-VAD headache, since, in such cases, physicians may suspect recurrence of the past headache. In fact, there are some reports of difficulty in the diagnosis due to this reason (22,23). However, our results showed that IC-VAD-related headache was different from the previous headache in most patients (83%). This may be helpful in the diagnosis. Based on our indicated headache characteristics, we attempted to establish a scoring system for diagnosis of the headache. In the current study, none of the patients had scores of 0–2, while scores of over 4 points were seen in 95% of the patients. Hence, a score of over 4 points on this scoring system may enable the diagnosis of IC-VAD.
Limitations
This study has some limitations. First, our study involved only a small number of subjects; hence, our findings regarding headache characteristics need to be validated in a larger study. Therefore, we cannot give definitive suggestions for improvement of the ICHD-3 beta, which has been established after much research. Second, because this study covered a long time span, there is a possibility of recall bias. Third, although we suggested a scoring system for the diagnosis, we did not prove its accuracy. The scoring system needs to be tested in a non IC-VAD group with primary headache. Finally, investigation of the sensitivity and specificity of this scoring system using a prospective study is needed.
Conclusion
Our results identified seven headache characteristics in patients with IC-VAD. These headache characteristics almost completely corresponded with those shown in ICHD-3 beta and the Clinical Practice Guideline for Chronic Headache 2013. However, headache with concomitant clinical symptoms that are distinct from ischemic symptoms and headache without nausea or vomiting are not described in these previous tools. We believe that the headache characteristics shown in this study may be helpful in the diagnosis of IC-VAD.
Footnotes
Clinical implications
We clarified the characteristics of intracranial vertebral artery dissection (IC-VAD)-related headache using our original self-administered questionnaire.
Our results identified the following seven headache characteristics in patients with IC-VAD: occurring in the occipitonuchal region, unilateral, pulsatile, of acute onset, severe, without nausea or vomiting, and with concomitant clinical symptoms unrelated to ischemia.
Based on our evaluation, the presence of four or more of these characteristics may suggest the existence of IC-VAD.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.