
Abstract
Objective
To examine the relationship between white matter hyperintensities and headache.
Methods
White matter hyperintensities burden was assessed semi-quantitatively using Fazekas and Scheltens scales, and by manual and automated volumetry of MRI in a sub-study of the general population-based Nord-Trøndelag Health Study (HUNT MRI). Using validated questionnaires, participants were categorized into four cross-sectional headache groups: Headache-free (n = 551), tension-type headache (n = 94), migraine (n = 91), and unclassified headache (n = 126). Prospective questionnaire data was used to further categorize participants into groups according to the evolution of headache during the last 12 years: Stable headache-free, past headache, new onset headache, and persistent headache. White matter hyperintensities burden was compared across headache groups using adjusted multivariate regression models.
Results
Individuals with tension-type headache were more likely to have extensive white matter hyperintensities than headache-free subjects, with this being the case across all methods of white matter hyperintensities assessment (Scheltens scale: Odds ratio, 2.46; 95% CI, 1.44–4.20). Migraine or unclassified headache did not influence the odds of having extensive white matter hyperintensities. Those with new onset headache were more likely to have extensive white matter hyperintensities than those who were stable headache-free (Scheltens scale: Odds ratio, 2.24; 95% CI, 1.13–4.44).
Conclusions
Having tension-type headache or developing headache in middle age was linked to extensive white matter hyperintensities. These results were similar across all methods of assessing white matter hyperintensities. If white matter hyperintensities treatment strategies emerge in the future, this association should be taken into consideration.
Keywords
Introduction
Tension-type headache (TTH) and migraine are the two most common primary headache disorders (1,2). Those who experience migraine seem to have more white matter hyperintensities (WMH) than those who are headache-free (3–8). WMH refer to hyperintense lesions in the white matter visible on T2-weighted magnetic resonance imaging (MRI) (9). A limited WMH load is reported in more than 90% of individuals older than 60 years (10), and is considered normal among the elderly population (11). However, larger amounts of WMH, especially in the deep white matter, may indicate cerebrovascular disease, as the lesions often reflect histopathological changes and molecular markers typical of ischemia (12). A high WMH load is associated with cardiovascular risk factors (13), as well as increased risks of dementia, stroke, and death (14). The impact on the brain of having migraine has been addressed more in previous studies than the impact of having non-migrainous headaches. The few published studies on WMH in non-migrainous headache in adults are contradictory, showing both increased (3,7) and equal amounts (8) of WMH in comparison with controls. The longitudinal MRI studies in adults with headache are also few and conflicting, as findings of both a progressing (6,15) and stable (8) WMH load are reported.
We have previously shown that individuals with headache, and especially with TTH, have increased odds of having minor intracranial abnormalities. WMH determined by a Fazekas score >1 was the predominant pathology in that study (16). In the current study, brain MRI was used to assess the amount of extensive WMH in a random selection of individuals from the general population. Since conflicting reports in the literature may result from the varying methodology used for assessing WMH, we implemented several different methods of assessing WMH; Fazekas and Scheltens semi-quantitative scales, automated WMH volumetry, and for the first time in research investigating relationships between WMH and headache, manual delineation of WMH was performed. Self-reported headache data over a 12-year period from the Nord-Trøndelag Health Study (HUNT) (17–19) was used to examine associations between the most common headache disorders and WMH, and to investigate what effect temporal evolution of headache had on WMH.
Methods
Participants and the MRI examination
Scan parameters for the MRI sequences.

IR-FSPGR: inversion recovery prepared fast spoiled grass; FLAIR: fluid attenuated inversion recovery; NSA: number of signal averages; TR: repletion time; TE: Echo time; FOV: field of view.
Measurement of WMH
Using FLAIR images, WMH were independently evaluated by two experienced neuroradiologists using the semi-quantitative Fazekas (22) and Scheltens (23) scales. The Fazekas scale rates WMH on a four-point scale: Absent (0), periventricular caps or thin lining or punctuate foci in deep white matter (1), periventricular halo or beginning confluence in deep white matter (2), and periventricular WMH extending into deep white matter or large confluent areas of WMH in deep white matter (3) (22). The Scheltens scale rates periventricular WMH from zero to six, and deep WMH from 0 to 24 (23). According to the standards of the neuroradiology lab of Barkhof and Scheltens, WMH less than 10 mm from the ventricular system were categorized as periventricular. Only lesions with a diameter ≥2 mm were categorized as WMH. Infratentorial hyperintensities or those located in the basal ganglia were not included, as this is normal reading procedure in our clinic and recommended in a position paper on neuroimaging of small vessel disease (9). Differences in opinion regarding the Fazekas score were resolved by consensus following discussion. Manual volumetry was performed in all participants with a Fazekas score above 0. This was performed by a specially trained research assistant who delineated the WMH on the FLAIR images using the software tool Multi-image Analysis Graphical User Interface (MANGO) (24). Each transverse slice was analyzed separately, and the volume of WMH in mm3 was calculated (WMH area × 5 mm slice thickness) and combined across slices. In the main volumetric analyses, individuals with WMH graded as 0 on the Fazekas scale by both neuroradiologists were counted as not having WMH (0 mm3) on manual volumetry. Cerebral infarctions, perivascular spaces, and microbleeds were excluded from visual and manual volumetric measurement of WMH. Automated volumetry was based on white matter hypointensity volumes obtained from T1-weighted volumes using the FreeSurfer 4.50 suite (25). Limited WMH are common in older populations (10). Therefore, to compare those who probably had a clinically relevant amount of WMH to those with findings within normal limits, WMH were categorized as limited and extensive in the current study. This dichotomization also made no assumption of a linearity of the data. The cut-off score for the Fazekas scale for extensive WMH was set to ≥2 according to normal clinical practice (11). For the Scheltens scale and WMH volumetry, there is no consensus on what cut-off should be used to indicate an extensive amount of WMH. The cut-offs for extensive WMH were therefore a priori set to WMH load in the upper quartile, to have groups sizes that allow reasonable statistical power. Using a method based on the Statistical Parametric Mapping (SPM) software package, intracranial volumes were calculated using the adapted reverse and automatic reverse brain-masking techniques (26).
Headache classification
The headache classifications in HUNT3 were described in an earlier paper (16). In short, answers to HUNT3 questionnaires were used to categorize respondents into one of four validated (18) and mutually exclusive groups: Headache-free, TTH, migraine, or unclassified headache (Figure 1). As the “infrequent TTH” criteria (headache <1 day a month) had low specificity (18,27), only those reporting frequent or chronic (≥1 day/month) headache were categorized as having TTH in the main analyses. Those reporting infrequent TTH were categorized as having unclassified headache in the main analyses. Longitudinal headache classification was based on identical and validated headache screening questions in HUNT2 and HUNT3 (18,17). Respondents were classified into four mutually exclusive groups according to the temporal evolution of headache over the approximately 12-year period from HUNT2 to HUNT3: Stable headache-free (reporting freedom from headache in both surveys), past headache (headache in HUNT2 but not in HUNT3), new onset headache (no headache in HUNT2 but headache in HUNT3), and persistent headache (reporting headache in both surveys) (Figure 1).
Flowchart describing the cohort.
Demographics, health-related information, and clinical measurements
Total Hospital Anxiety and Depression Scale (HADS) score and self-reported information on sex, employment status, alcohol habits, health, smoking, and history of ischemic heart disease (myocardial infarction and angina pectoris) were derived from HUNT3. A value above zero on the CAGE questionnaire (28) (a screening test for alcoholism) was counted as potential alcohol overuse. Body mass index, blood pressure, total serum cholesterol, serum triglycerides, and non-fasting serum glucose were measured at the medical examination that was a part of the HUNT surveys. Blood pressure was measured three times, with the mean of the two last measurements being used. The age used in the analyses was that at the time of MRI acquisition. Those with cerebral infarctions on examination of the MRI were categorized as having suffered a cerebral infarction (20).
Statistical methods
HUNT3 background data for respondents and non-respondents to the headache questionnaire, and for the different headache groups in the MRI study.

Ninety subjects with TTH had headache 1–14 days per month, and four had headache > 14 days per month.
Forty-six subjects with migraine reported visual aura, and sixteen reported sensory aura.
TTH: tension-type headache ≥ 1 day per month; Alcohol consumption: positive response to a CAGE question; Fair or poor health: fair or poor self-perceived health; Ischemic heart disease: self-reported myocardial infarction or angina pectoris; HADS: Total Hospital Anxiety and Depressions Scale; BMI: body mass index; SBP: systolic blood pressure in mmHg; DBP: diastolic blood pressure in mmHg; Cholesterol: total serum cholesterol in mmol/L; Triglyceride: serum triglyceride in mmol/L; Glucose: non-fasting serum glucose in mmol/L.
Numbers and percentages of eligible individuals answering the headache screening questions (862) who did not answer the respective questions or did not undergo the measurement procedures: Employment status (n = 7, 0.8%), body mass index (n = 1, 0.1%), alcohol consumption (n = 73, 8.5%), self-reported health (n = 13, 1.5%), HADS (n = 6, 0.7%), mean systolic blood pressure (n = 9, 1.0%), mean diastolic blood pressure (n = 8, 0.9%), and cholesterol/triglycerides/glucose (n = 49, 5.7%). The question regarding daily smoking was asked in such a manner that missing data were most sensibly interpreted as a negative answer.
HUNT3 background data for respondents and non-respondents to the headache screening question in HUNT2 and HUNT3, and for the different longitudinal headache groups.

Alcohol consumption: positive response on a CAGE question; Fair or poor health: fair or poor self-perceived health; Ischemic heart disease: self-reported myocardial infarction or angina pectoris; HADS: total Hospital Anxiety and Depressions Scale; BMI: body mass index; SBP: systolic blood pressure in mmHg; DBP: diastolic blood pressure in mmHg; Cholesterol: total serum cholesterol in mmol/L; Triglyceride: serum triglyceride in mmol/L; Glucose: non-fasting serum glucose in mmol/L.
Numbers and percentages of eligible individuals answering both headache screening questions (778) who did not answer the respective questions or did not undergo the measurement procedures: employment status (n = 7, 0.9%), body mass index (n = 1, 0.1%), alcohol consumption (n = 67, 8.6%), self-reported health (n = 12, 1.5%), HADS (n = 5, 0.6%), mean systolic blood pressure (n = 6, 0.8%), mean diastolic blood pressure (n = 5, 0.6%), cholesterol/triglycerides/glucose (n = 41, 5.3%). The question regarding daily smoking was asked in such a manner that missing data were most sensibly interpreted as a negative answer.
Prevalence of white matter hyperintensities according to headache groups.

TTH: Tension-type headache ≥1 day per month; IQR: Interquartile range.
Note: Due to missing responses, the cut-offs defining the upper quartile varied slightly for cross-sectional vs. longitudinal data for manual volumetry (≥834 mm3 vs. ≥847 mm3), and automated volumetry (≥2680 mm3 vs. ≥2682 mm3), but cut-offs were identical for cross-sectional and longitudinal data for the Scheltens score (≥7).
Headache status and odds ratios for extensive white matter hyperintensities.

TTH: Tension-type headache ≥ 1 day per month.
White matter hyperintensities measured with Fazekas or Scheltens scale, or manually, or automated as dependent variable. Headache status (headache-free as reference), age, and sex included as categorical covariates.
As a, but also with daily smoking, responses to CAGE questions, ischemic heart disease, and cerebral infarction included as categorical covariates, and total HADS score, total serum cholesterol, serum triglyceride, non-fasting serum glucose, body mass index, and mean systolic blood pressure included as continuous covariates.
p value < 0.05.
Ethical approval
The study was approved by the Norwegian Data Inspectorate, the Norwegian Board of Health, and the Regional Committee for Ethics in Medical Research. All participants provided written informed consent.
Results
Subjects responding to the headache questionnaire in HUNT3
Of the 862 MS-free respondents to the HUNT3 headache questionnaire, 11% had TTH ≥ 1 day per month, 11% had migraine, and 15% had unclassified headache (Table 2). Of the 126 with unclassified headache, eight had medication-overuse headache and 52 had TTH < 1 day per month. Compared with the respondents to the HUNT3 headache questionnaire, the 141 individuals who did not answer the headache questions (non-respondents) were somewhat more likely to smoke and to give a positive answer to the CAGE questions (Table 2). Compared with the headache-free subjects, those reporting headache showed a larger proportion of females, reported worse general health, and were less likely to give a positive answer to CAGE questions (Table 2).
Subjects responding to the headache questionnaires in both HUNT2 and HUNT3
Of the 778 MS-free individuals answering the headache screening question in both HUNT2 and HUNT3, 44% were classified as stable headache-free, 19% as having past headache, 8% as having new onset headache, and 29% as having persistent headache (Table 3). The respondents who answered the headache questionnaires in both HUNT2 and HUNT3 reported better general health and a lower number of them smoked in comparison with the 225 subjects who did not answer both headache questionnaires. Stable headache-free subjects were more likely to be male and to report good general health than those having headache at any time point (Table 3).
Measurement of WMH
The WMH were graded with the Fazekas and Scheltens scales for all respondents (Figure 2). Thirty seven individuals were excluded from both automated and manual WMH volumetry because of motion or image artifacts. Automated measurements were therefore obtained in 825 individuals. Manual measurements could not be performed on a further 13 individuals, as FLAIR images were either not available or of poor quality. Of the remaining 812 individuals, manual volumetry was performed on 407 individuals who received a Fazekas score ≥1 from at least one neuroradiologist.
Examples of white matter hyperintensities of Fazekas grade 1–3.
Cross-sectional headache data and WMH
Individuals with TTH had the highest prevalence of extensive WMH of all the groups (Table 4). In both the A and B regression models (Table 5), those with TTH had increased odds of having extensive WMH compared with headache-free subjects, with this being the case across all measuring methods: Fazekas odds ratio (OR), 3.07 and 95% CI, 1.51–6.21; Scheltens OR, 2.46 and 95% CI, 1.44–4.20; manual volumetry OR, 2.00 and 95% CI, 1.13–3.55; automated volumetry OR, 2.64 and 95% CI, 1.49–4.67. No association was found between the other headache types and extensive WMH in the main analyses (Table 5). In the sub-analyses of deep and periventricular WMH (Supplemental Tables 1–2), individuals with TTH had increased odds of extensive WMH in the deep (OR, 2.01; 95% CI, 1.18–3.44), but not periventricular, white matter. Respondents with migraine were less likely to have extensive periventricular WMH than those who were headache-free (OR, 0.48; 95% CI, 0.24–0.98). Sensitivity analyses treating participants without manual volumetry (Fazekas = 0) as missing, and analyses including those with infrequent TTH in the TTH group, produced similar results to the main analyses (Supplemental Tables 2–4). Excluding 25 individuals with hemispheric infarctions from analyses using automated volumetry, and excluding eight individuals with medication-overuse headache from cross-sectional analyses, did not change the main results substantially (data not shown).
Longitudinal headache data and WMH
Longitudinal headache groups and odds ratios for extensive white matter hyperintensities.
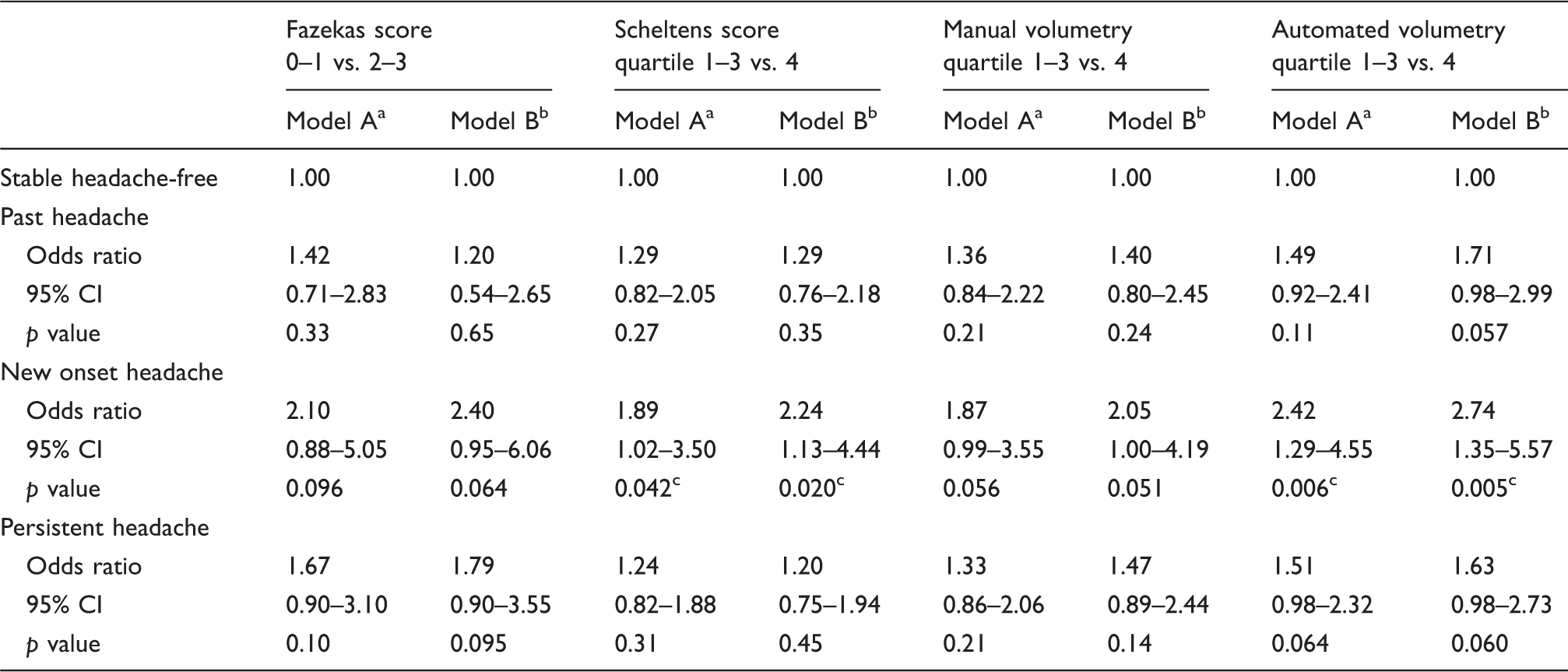
White matter hyperintensities measured with Fazekas or Scheltens scale, or manually, or automated as dependent variable. Temporal evolution of headache (stable headache-free as reference), age, and sex included as categorical covariates.
As a, but also with daily smoking, responses to CAGE questions, ischemic heart disease, and cerebral infarction included as categorical covariates, and total HADS score, total serum cholesterol, serum triglyceride, non-fasting serum glucose, body mass index, and mean systolic blood pressure included as continuous covariates.
p value < 0.05.
Discussion
The main findings of this study were that individuals with TTH had more extensive WMH than those who were headache-free, while individuals with migraine or unclassified headache did not have more extensive WMH than headache-free subjects. Analyses using longitudinal headache data revealed that those reporting onset of headache in adult life had more extensive WMH than individuals who were stable headache-free. The results were similar when using semi-quantitative and volumetric methods of measuring WMH.
Comparison with earlier studies on WMH in headache populations
Our findings with regard to the association between extensive WMH and TTH are in line with a case-control study that specifically included individuals with TTH (3), as well as a population-based study on non-migrainous headache (7). However, they differ from another population-based study that did not find a difference in WMH occurrence between people with non-migrainous headache and those who were headache-free (8). Our finding of a lack of association between migraine and WMH is in line with another population-based study (30), but differs from four other population-based studies that did report more WMH in individuals with migraine (4,6–8). The age ranges in these previous studies and the present study are quite similar and cannot explain the discrepant results. There were, however, differences in sample size, and previous studies that detected an association between WMH and migraine included more people with migraine than in this study (4,6–8). Therefore, we may have lacked the power to detect a potentially increased risk of WMH in people with migraine. Nevertheless, the sizes of the TTH and migraine groups were similar, and we found a significant association between TTH and WMH, and not between migraine and WMH. It therefore appears that WMH are more strongly associated to TTH than to migraine. This underlines the importance of including individuals with non-migrainous headache in future research.
We found that WMH had a stronger and more consistent association with new onset headache (after the age of 40) than with persistent headache. This suggests that headache starting in adulthood have a greater impact on white matter than headache starting in younger years, rather than there being a dose-response relationship between headache burden and WMH over time. This finding is at variance with the previously reported WMH progression in people with migraine (6,15), which suggests a dose-response relationship between headache and WMH. However, others have also reported that WMH are stable in individuals with migraine (8). The current findings imply that different pathophysiological mechanisms may be involved in headache during the lifespan. Headaches that start later in life are more likely to be secondary to other diseases, which may explain their relation to WMH.
Potential pathophysiological mechanisms
WMH may have a vascular etiology (12), and cerebral ischemia is usually highlighted as a potential cause of WMH in individuals with headache (4,6,7). Interestingly, it has also been reported that those who experience migraine are more likely to be affected by cerebral infarctions than those who are headache-free (4,7,31), but this finding is not consistent across all populations (32). The finding of more extensive WMH in TTH in the current and previous studies (3,7) suggests that ischemic and inflammatory processes in white matter are either caused by or accompany TTH. The fact that WMH in this study were more pronounced in deep white matter indicates a vascular cause. However, vascular factors are currently not viewed as a major factor in the pathophysiology of TTH. Furthermore, we attempted to adjust for cardiovascular risk factors in the present study, which supports the notion that WMH in TTH is not associated with cardiovascular health in general. WMH may also have non-ischemic causes such as degenerative changes, blood-brain barrier leakage, inflammation, and amyloid angiopathy, as seen with histopathological investigations of WMH in autopsy studies (12).
WMH measuring methods
In the present study, semi-quantitative scales and volumetric methods provided very similar results. Our findings imply that the easily available semi-quantitative methods for WMH assessment, which are often a standard part of the neuroradiological reading above a certain age, are acceptable measures to use in cross-sectional headache research. The more advanced Scheltens scale provides additional information by separating lesions into periventricular and deep WMH, which can improve accuracy since the latter are associated with ischemic histopathology and molecular markers of hypoxic injury (12). Analyses based on automated volumetry produced higher odd ratios than those based on manual volumetry. Automated volumetry was performed on more individuals than manual volumetry, which may explain the difference in the results. However, we would like to point out that the results were overall comparable, and that, in general, these methods are difficult to compare as they estimate WMH in different ways. WMH measuring methods cannot explain the difference in results between the present study and the previous studies, as similar methods used in earlier studies were explored in the current study, that is, automated volumetric methods (6–8,30) and visual grading (3,4,6,8).
Clinical relevance
WMH burden is associated with several negative outcomes in aging (14), and the mechanisms behind the association between WMH and TTH need to be elucidated to optimize population brain health. The previous finding in HUNT of a significantly increased risk of later dementia in people with non-migrainous headache further supports the notion that this headache type is linked to detrimental pathophysiological changes in the brain and needs closer scrutiny (33). As there are no established strategies on how to manage WMH, the present results do not imply that brain MRI is warranted in individuals with headache to map WMH. However, correcting cardiovascular risk factors have been shown to delay the progression of WMH (34), and treatment strategies may emerge in the future. In that case, having TTH or late onset headache should strengthen the indication of performing an MRI examination. Since headache affects approximately 50% of the adult population during the course of a single year (35), the results of this study have public health relevance.
Strengths and limitations
This study has several strengths. It has a population-based design and includes a large number of participants. The study population is representative of the middle-aged Norwegian population (21), and the results are therefore generalizable to similar populations. Furthermore, participants in the HUNT MRI study were selected at random, independently of headache status, and the questionnaires allowed for categorization of respondents into headache groups on the basis of validated primary headache diagnoses (18,27,17). Also, documentation of headache at two time points is probably more reliable than a single retrospective description of both periods. The MRI protocol was standardized, and several methods for measuring WMH were used in the analyses. Manual volumetry gives the most accurate measurement of WMH volume, and this is the first population-based study where manual volumetry was used to investigate associations between WMH and headache.
The study also has several limitations. Participants had fewer cardiovascular risk factors than those who did not participate (21). This could result in a systematical underestimation of the prevalence of WMH (13). However, the differences in risk factors, and therefore their potential effect on our estimates, were small (21). There is no consensus on what cut-off should be used to indicate an extensive amount of WMH when using volumetry and Scheltens scale, which make it difficult to compare results across studies. Continuous data was dichotomized based on the assumption that limited and extensive WMH have different clinical relevance. This approach leads to a loss of data, which reduces statistical power and limits our potential to correct for confounding factors. As some reports indicate that the association between WMH and migraine is specific for women (4,6), it would have been interesting to stratify for sex. However, as only 24 men had migraine, this sub-analysis would have low power in the current cohort. The measurement of headache by a self-administered questionnaire is inferior to a clinical interview performed by a trained physician, although the headache criteria had fair sensitivity and specificity (18,27). The migraine diagnosis was highly specific (95%), but had a sensitivity of only 50% (18). Therefore, some respondents with migraine were probably categorized as having TTH or unclassified headache. Our questionnaire also allowed for only one primary headache diagnosis per respondent. If WMH have a dose-response relationship with duration of pain, selecting those with TTH ≥ 1 day/month may exaggerate the association between TTH and WMH. However, sensitivity analyses that included those with infrequent TTH in the TTH group did not give different results. In the main analyses, each headache group was compared with the headache-free group using two models across four methods of measuring WMH. Performing multiple comparisons raises the likelihood of making type I errors. We have tried to make a judicious evaluation of the results instead of performing a correcting procedure that increases the likelihood of performing type II errors. The association between TTH and WMH appears to be genuine, as only TTH was significantly associated with WMH in the cross-sectional analyses. Furthermore, this association was consistently observed in every analysis, making it unlikely to be a spurious finding. In longitudinal analyses, associations were less clear, and some could represent spurious findings. The modest number of individuals with TTH and migraine reduces the statistical power of some analyses. This could also mean that model B is overfitted, which limits our potential to correct for confounding factors.
Conclusion
In this population-based neuroimaging study, individuals with TTH and those who developed a new headache in adulthood had more extensive WMH than headache-free subjects. These results were similar across all methods of assessing WMH. Our findings suggest that these headaches are accompanied by structural alterations in the brain. This underlines the importance of differentiating between headache sub-types and taking changes in headache occurrence over time into consideration when future investigations into the relationship between WMH and headache are undertaken.
Supplemental Material
Supplementary tables -Supplemental material for White matter hyperintensities and headache: A population-based imaging study (HUNT MRI)
Supplemental material, Supplementary tables for White matter hyperintensities and headache: A population-based imaging study (HUNT MRI) by Lasse-Marius Honningsvåg, Asta Kristine Håberg, Knut Hagen, Kjell Arne Kvistad, Lars Jacob Stovner and Mattias Linde in Cephalalgia
Footnotes
Article highlights
Having tension-type headache or developing headache in adulthood were linked to the occurrence of extensive white matter hyperintensities.
The increased risk of extensive white matter hyperintensities was observed across all methods of WMH assessment.
There were no associations between white matter hyperintensities and migraine or unclassified headache.
Acknowledgements
The staff at the Department of Radiology, Levanger hospital, performed the MRIs. Neuroradiologists Kjell Arne Kvistad and Jana Rydland at the Department of Radiology and Nuclear Medicine read all MRIs. Research assistant Axel Kvistad manually delineated the WMH. The Nord-Trøndelag Health Study (HUNT) is a collaboration between the HUNT Research Centre, the Faculty of Medicine at the Norwegian University of Science and Technology (NTNU), the Norwegian Institute of Public Health, and the Nord-Trøndelag County Council.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, but was supported by NTNU Norwegian University of Science and Technology; National Norwegian Advisory Unit for functional MRI; and St. Olav's University Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.