
Abstract
Objective
Glossopharyngeal neuralgia (GPN) is a very rare condition, affecting the patient’s quality of life. We report our experience in drug-resistant, idiopathic GPN, treated with Gamma Knife radiosurgery (GKRS), in terms of safety and efficiency, on a very long-term basis.
Methods
The study was opened, self-controlled, non-comparative and bicentric (Marseille and Lausanne University Hospitals). Patients treated with GKRS between 2003 and 2015 (models C, 4C and Perfexion) were included. A single 4-mm isocentre was positioned in the cisternal portion of the glossopharyngeal nerve, with a targeting based both on magnetic resonance imaging (MRI) and computed tomography (CT). The mean maximal dose delivered was 81.4 ± 6.7 Gy (median = 85 Gy, range = 60–90 Gy at the 100% isodose line).
Results
Twenty-one patients (11 women, 10 men) benefited from 25 procedures. The mean follow-up period was 5.2 ± 3 years (range = 0.9–12.1 years). Seventeen (81%) were initially pain-free after GKRS. At three months, six months and one year after radiosurgery, the percentage of patients with good outcome (BNI classes I to IIIA) was 87.6%, 100% and 81.8%, respectively. Ten cases (58.8%) from the initial pain-free ones had a recurrence, after a mean period of 13.6 ± 10.4 months (range = 3.1–36.6 months). Only three patients (14.2%) had recurrences (two for each one of them) requiring further surgeries. Three patients underwent a second GKRS procedure; one case needed a third GKRS. The former procedures were performed at 7, 17, 19 and 30 months after the first one, respectively. Furthermore, two patients needed additional interventions. At last follow-up, 17 cases (80.9%) were still pain-free without medication. The actuarial pain relief without new surgery was 83%. A transient complication (paraesthesia of the edge of the tongue) was seen in one case (4.8%).
Conclusion
GKRS is a valuable, minimally invasive, surgical alternative for idiopathic GPN, with a very high short- and long-term efficacy and without permanent complications. A quality imaging, including T2 CISS/Fiesta MRI and bone CT acquisitions for good visualisation of the nerve and the other bony anatomic landmarks, is essential for targeting accuracy and successful therapy.
Introduction
Glossopharyngeal neuralgia (GPN) is an uncommon painful condition of the ninth cranial nerve. It is characterised by short episodes of severe paroxysmal pain, affecting the throat, tongue and ear, and can be also associated in severe cases with haemodynamic instability, vasomotor changes leading to syncope, cardiac arrhythmias, bradycardia, hypotension or even asystole (1). Patients may also present with malnutrition and weight loss, due to triggering of the pain by swallowing (2). The incidence is around 0.4 in 100,000 inhabitants (3). The aetiology remains unknown but, as in the case of idiopathic trigeminal neuralgia (TN), vascular compression is considered a possible cause (4).
The first line of treatment is pharmacological. Carbamazepine is frequently used (5), as well as other types of anti-epileptic drugs, including Gabapentine. When the drug treatment becomes ineffective and/or is subject to major side effects, surgical treatment is considered, including microvascular decompression (MVD), percutaneous thermocoagulation (6), neurotomy by sectioning of the glossopharyngeal nerve and the upper rootlets of the vagus nerve (7), or Gamma Knife radiosurgery (GKRS) (8). Microvascular decompression is considered to treat the possible cause (i.e. the vascular compression) and its use in GPN has been pioneered by Laha and Janetta (4), and further confirmed in terms of initial efficacy (up to 80–90%) by several studies (9–12). However, it yields also the risk of lower cranial nerve injuries, in the range of 8–19% depending on the published series (9–16). GKRS is accepted nowadays as a minimally invasive treatment in medically refractory TN, with a high rate of initial efficacy, as high as 90%, and very low complication rates, mainly hypoesthesia (17,18). Based on the previous, GKRS has been also considered for GPN, being pioneered in this indication by Stieber et al. (8) and further confirmed by other teams, including ours, with similar initial results and no complications (8,19–26)
We report our bi-centric experience (Marseille, France and Lausanne, Switzerland) in 21 patients (benefitting from 25 procedures) with medically refractory idiopathic GPN. We analyse the initial efficacy, the possible appearance of any side effects, as well as the probability of maintaining pain relief on a very long-term basis.
Material and methods
Study design and patients
Our study was designed to be open, self-controlled and non-comparative. A case-report form (containing the same items in both centres) was created and prospectively foiled in. All cases were evaluated by a neurologist to confirm the diagnosis, according to the criteria established by the International Headache Society (1) and drug resistance. Brain magnetic resonance imaging (MRI) revealed no structural abnormality and no extrinsic compression, such as benign or malignant intracranial tumours, multiple sclerosis, vascular malformation, etc., allowing the exclusion of secondary GPN.
During 2003–2015, 21 patients (25 procedures) suffering from GPN were treated by GKRS and followed up in Marseille and Lausanne University Hospitals, respectively.
Radiosurgical technique
After application of the Leksell Model G stereotactic frame (Elekta Instruments AB, Sweden) under local anaesthesia, all patients underwent MRI and computed tomography (CT) imaging for target definition. Two volumetric stereotactic three-dimensional (3D) MRI sequences were used to identify the glossopharyngeal nerve: sub-millimetric non-contrast T2-weighted constructive interference steady state (CISS) pulse sequences and millimetric contrast-enhanced T1-weighted images, with and without Gadolinium injection. A skull-base CT scan routinely supplemented these neuroradiological investigations in order to correct any distortion errors in the MRI studies and to visualise the glossopharyngeal meatus (18).
During 2003–2015, Gamma Knife models C, 4C and Perfexion (Elekta Instruments AB, Sweden) were successively used. A single 4-mm isocentre was used in all patients and a cisternal target was positioned in the anterior cisternal portion of the glossopharyngeal nerve (Figure 1) close to the glossopharyngeal meatus. The mean maximal dose delivered was 81.4 ± 6.7 Gy (median = 85 Gy, range = 60–90 Gy). The mean maximal dose received by the brainstem was 2.5 ± 1.5 Gy (0.5–7.1), with no necessity of using beam channel blocking, according with our previously published methodology, regarding dosimetry constraints for the brainstem for TN (18). The mean targeting isocentre distance was 14.6 ± 3 mm (range = 9.3–23.5 mm) anterior to the emergence of the nerve. The variation of the range is the reflection of the anatomical nerve variability.
Radiosurgical targeting positioned in the anterior cisternal portion of the glossopharyngeal nerve, close to the glossopharyngeal meatus, using a sub-millimetric non-contrast T2-weighted CISS pulse sequence fused with CT.
Follow-up measures and monitoring
The patients and the referring doctors were advised to continue the medication unchanged for at least one month after radiosurgery. Furthermore, if the patients had become pain-free, they were able to decrease their drug doses progressively. Follow-up consisted of a neurological evaluation at regular intervals of three, six, nine and 12 months and on a yearly basis thereafter.
All patients had at least six months of follow-up. Initial pain relief was scored using the Barrow Neurological Institute pain scale (27): I = no trigeminal pain with no medication; II = occasional pain that does not require medication; IIIa = no pain with continued medication; IIIb = persistent pain controlled by medication; IV = some pain not adequately controlled by medication; and V = severe pain with no relief. Outcome measures also included time to initial pain relief, the onset and timing of any possible complication and the recurrence of pain (27). A recurrence was defined as change from class I to a lower outcome class. A minor recurrence was considered as one well tolerated by the patient (lower frequency and intensity of the pain) and not necessitating a new surgical therapy. A major recurrence was defined as one requiring an additional open, percutaneous or radiosurgical procedure.
Results
Basic demographic data
Demographic data.
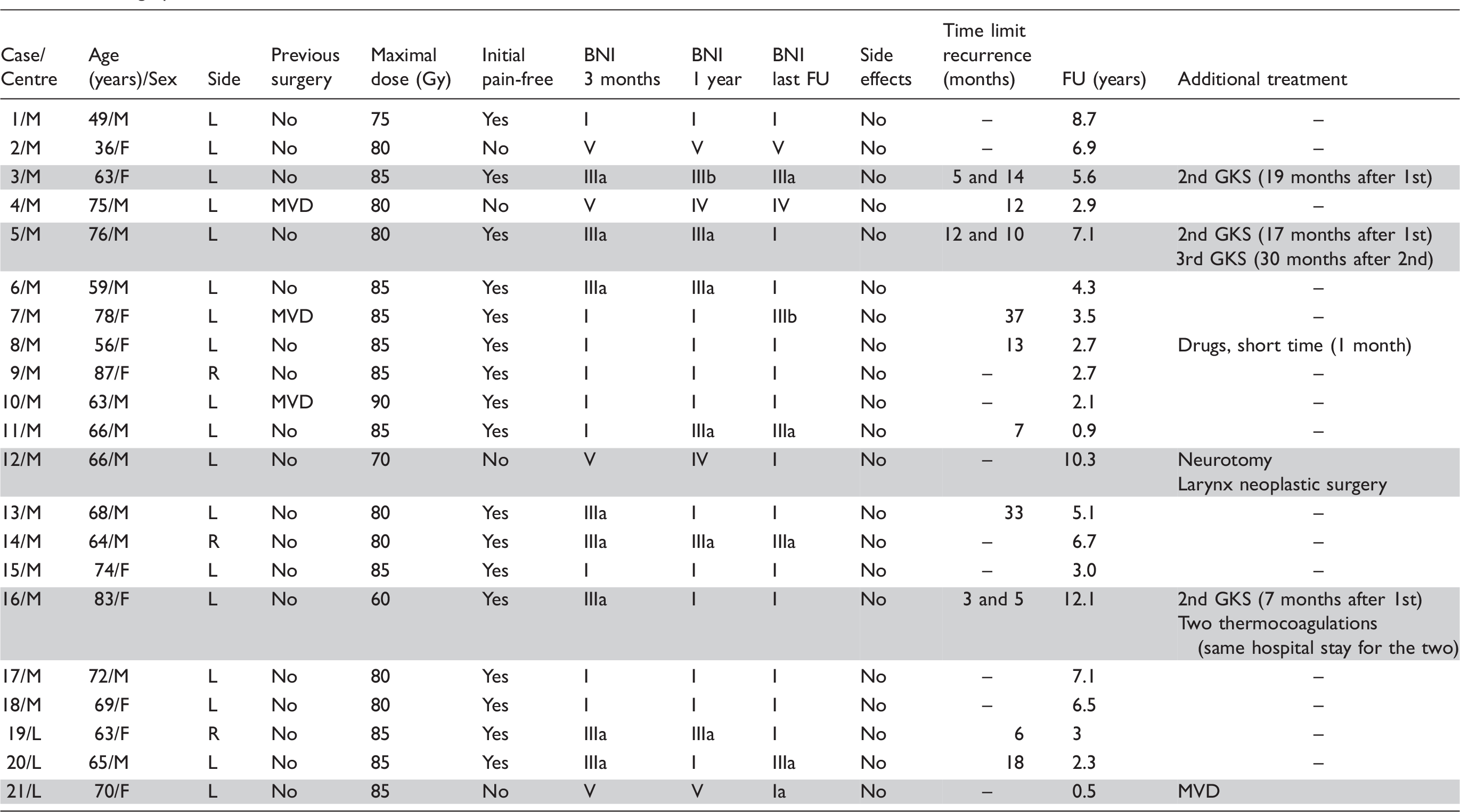
Three patients have had a previous MVD procedure, which was efficient for a period of two, eight and 13 years, respectively, before recurrence. One patient had three GKRS and two patients had two GKRS, for a total of 25 procedures. MVD was further performed in one patient (4.8%), who did not experience pain relief after first GKRS.
One patient died 3.5 years after GKRS after without causal relationship with radiosurgery.
Initial efficacy
Seventeen patients (81%) were initially pain-free after GKRS. Three months after radiosurgery, nine patients had no pain and were medication-free (BNI I) and eight patients (12 if we consider all GKRS procedures) had no pain but continued their treatment (BNI IIIa). Thus, initial good outcomes (BNI I + IIIa) were achieved in 81%. The mean time to pain relief was 25 days (median = 15 days, range = 1–120 days). Three patients did not improve.
Secondary effects
No permanent neurological complications were noted (no swallowing phonation disorders or dysgeusia). Only one patient (4.8%) presented with transient paraesthesia of the edge of the tongue, during one month following GKRS, that spontaneously disappeared.
Recurrence of pain and its management
Main results in our series.

Of the four patients who did not improve after GKRS (BNI IV or V), one patient had a neurotomy, whose effectiveness had been relative and of short duration (only four months). This same patient was operated on four years after GKRS for a neoplasia of the larynx; following this procedure, he was pain-free (BNI class I). For this case, the oncological context could have been responsible for his GPN.
At last follow-up, of the 17 patients with initial good outcomes, seven showed no recurrences and ten patients (58.8%) had a recurrence, occurring on average at a mean duration of 14.9 ± 12.2 months (range = 3.1–36.6 months) after GKRS. Six patients with recurrence were controlled by a chronic or punctual pharmacological treatment.
Three patients needed a new GKRS; one patient needed a third GKRS. The new GKRS procedures were performed at 7, 17, 19 and 30 months after the first one, respectively. One patient underwent a second GKRS 19 months after the first one and was BNI IIIa at his last FU. One patient underwent a second GKRS seven months after the first one and was not improved; she was treated nine months after the second GKRS by thermocoagulation, allowing her to become pain-free (BNI class I). One patient underwent a second GKRS at 17 months after the first and then a third GKRS 30 months later. For this patient, there were no side effects and he is still pain-free without medication (BNI class I). One patient who did not improve after GKRS had an MVD, with further pain relief with no medication (BNI Ia).
The actuarial rate of patients clinically improved after GKRS who did not need further surgery was 83.3% (see the Kaplan–Meyer curve in Figure 2).
The actuarial rate of patients clinically improved after GKRS (Kaplan–Meyer curve).
Discussion
The surgical management of medically refractory GPN involves both ablative and non-ablative procedures. Taha et al. (7) reported their results with ablative procedures, including extracranial sectioning of the superior laryngeal nerve, percutaneous radiofrequency rhizotomy at the jugular foramen or intracranial sectioning of the glossopharyngeal nerve and upper rootlets of the vagus nerve, the former with or without a concurrent MVD. In a series of 14 patients, 12 were still pain-free without medication at a mean follow-up interval of ten years. The only reported complication was dysphagia in one case (8%). Along the same line, Rushton et al. (28) reported a surgical experience of 129 patients (71 with sectioning at the level of the jugular foramen), treated over a period of 50 years, with 85% experiencing good pain relief. However, 19% developed transient or permanent dysphagia after surgery. MVD addresses the cause (i.e. the neuro-vascular compression, if one exists) and was developed by Janetta, including in cases of GPN. Laha and Janetta reported a series of six cases (three with additional concurrent nerve sectioning), with only one case experiencing complete pain relief (4). Other authors also reported their results after MVD. Resnick et al. (11) described a cohort of 40 cases, with complete or almost complete pain relief in 79% of the patients, with 76% still pain-free after a mean follow-up of 48 months. Patel et al. (10) presented a large series of 217 cases, with an overall immediate pain relief rate of 90%. Ferroli et al. (13) published a cohort of 31 patients, with 90.3% of them being pain-free after a mean follow-up of 7.5 years. In the whole MVD series, mortality is in the range of 0–5.8%, with a permanent cranial nerve palsy rate of 8–28.5% (6,7,9–16,23,28,29). In the series of Patel et al. (10), thanks to advances in microsurgery and in intensive care, the mortality decreased to 0% after 1987 and the cranial nerve palsy rate decreased from 28.5% to 3% after 1995.
Main series of the literature and their respective results.
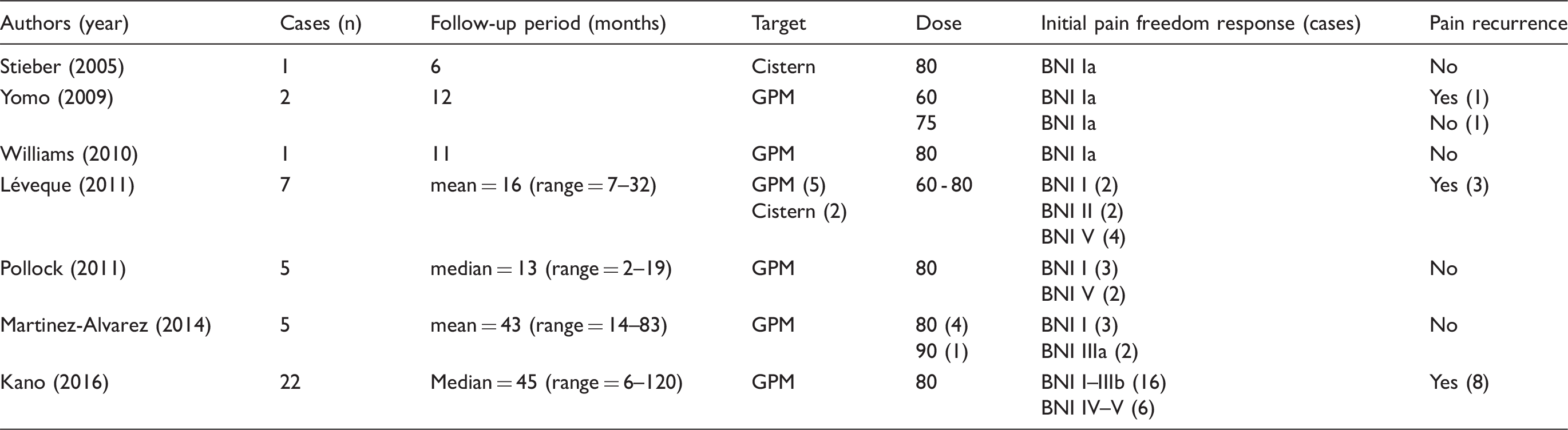
The present series of GKRS for GPN, along with the one of Kano et al. (32), is the largest one (21 cases with 25 procedures), with a very long-term follow-up of up to 12 years. There are two important technical aspects related to the use of GKRS in GPN: one is related to the visualisation of the glossopharyngeal nerve; the second is related to the prescribed therapeutic dose. The radiosurgical targeting is much more difficult compared with TN, due to the complex anatomy of lower cranial nerves, of the jugular foramen and the necessity of using a sub-millimetric T2-CISS/Fiesta images for clear visualisation of the target (33). Additionally, there is a very close distance, of 0.5–4.9 mm, between the 9th and 10th nerve. Also, CT is useful when identifying the bony landmarks, allowing for optimal targeting. The prescribed therapeutic dose has to be a minimum of 75 Gy, as we previously suggested, for better efficacy (26). In our more recent experience, we prescribed doses as high as 90 Gy, similar to the one used in TN (18), and with a median dose of 85 Gy. Our targeting method provides a sufficiently large distance reported to the exit of the nerve from the brainstem. This distance allows a high prescription dose, which ensures higher rates of freedom from pain. We were the first to demonstrate a relationship between a higher dose and improved rates of freedom of pain response in GPN, with a cutoff at 75 Gy. Additionally, placing a shot far from the brainstem allows being below the theoretical threshold of brainstem toxicity, which is considered 12 Gy at the margin (or maximum 15 Gy received by the first 10 mm3) in our experience. In the current paper, we report our experience with up to 12 years of follow-up, with no particular toxicity. The initial efficacy was high (81%). The actuarial rate of patients clinically improved after GKRS and did not need further surgery was 83.3%. In case of drug-resistant recurrence, several factors are taken into account, mainly the patient’s age, co-morbidities or the eventual presence of a neurovascular conflict. Usually, if the first GKRS had been effective for at least 12 months, a second procedure is proposed to the patient. However, MVD or thermocoagulation can be also proposed (as advocated in Table 1) depending on the individual context.
Conclusion
We report a large series of 21 patients, treated with GKRS for drug-resistant GPN, with a long follow-up period of up to 12 years. In our experience, this approach proved to be safe and effective, with minimal invasiveness and high long-term pain relief, without permanent complications. We consider that the therapeutic options for drug-resistant GPN, in the light of our experience and of the published series, should go from the non-invasive options (GKRS) to the more invasive options (MVD and neurotomies), so as to avoid major postoperative problems, while providing a similar efficacy. Further studies are needed giving the rarity of this medical condition and, so far, the limited GKRS experience in this indication. A quality imaging, including T2 CISS/Fiesta MRI and bone CT acquisitions for good visualisation of the nerve and other anatomic landmarks is essential for targeting accuracy and for successful therapy.
Clinical implications
Gamma Knife radiosurgery is a valuable, minimally invasive, surgical alternative for glossopharyngeal neuralgia with high short- and long-term efficacy and without any permanent complications. A quality imaging, including T2 MRI and CT acquisitions, is essential for targeting accuracy and successful therapy
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.