
Abstract
Cluster-tic syndrome is a rare, disabling disorder. We report the first case of cluster-tic syndrome with a successful response to stereotactic radiosurgery.
After failing optimal medical treatment, a 58-year-old woman suffering from cluster-tic syndrome was treated with gamma knife radiosurgery. The trigeminal nerve and sphenopalatine ganglion were targeted with a maximum dose of 85 and 90 Gy respectively. The patient experienced a complete resolution of the initial pain, but developed, as previously described after radiosurgical treatment for cluster headache, a trigeminal nerve dysfunction. This suggests that trigeminal nerve sensitivity to radiosurgery can be extremely different depending on the underlying pathological condition, and that there is an abnormal sensitivity of the trigeminal nerve in cluster headache patients. We do not recommend trigeminal nerve radiosurgery for treatment of cluster headache.
Introduction
Trigeminal neuralgia (TN) has been described in patients with other concomitant headaches. The association of cluster headache with TN is known as cluster-tic syndrome. This rare syndrome has not yet been included in the second edition of the International Classification of Headache Disorders (ICHD-2) published by the International Headache Society. Several forms of cluster-tic have been described. The tic and cluster components of this syndrome can occur concurrently or separately in time, in the same patient (1). Cluster-tic syndrome may be primary or secondary (the latter due to pituitary adenoma, basilar artery ectasia) (2,3). Patients are usually treated with a combination of drugs for TN and cluster headache (4), or with microvascular decompression of the trigeminal nerve (5).
This report documents a case of intractable cluster-tic with complete resolution of the initial pain after gamma knife radiosurgery (GKR), but complicated by the development of deafferentation pain syndrome. This confirms the particular sensitivity of the trigeminal nerve to GKR in cluster headache patients.
Case report
A 58-year-old woman presented with a 5-year history of two main types of right-sided facial pain. She described concurrent clinical manifestations. The first type of pain had a usual duration of 5–60 s. The pain was strictly unilateral and localized to the right orbit and forehead, and was described as a sudden, sharp, severe, stabbing headache. The jabs were both spontaneous and triggered by washing the face or brushing the teeth. There was no trigger zone.
During the same attack, the second type of pain followed immediately after the first one. The headache was ipsilateral, and described as a very severe, penetrating periocular right-sided pain, associated with right-sided lacrimation, rhinorrhea and swelling of the eyelid, which lasted between 30 and 60 min. This second type of pain could be triggered. The attack frequency was from one attack/week to one to four attacks/day.
At the beginning of the disease, the pain had the clinical presentation of right-sided TN located initially in the first division, and later in both the first and the second divisions of the trigeminal nerve. Multiple attacks (∼20 attacks/day) were described, alternately with periods of remission lasting a few months.
General and neurological examinations were unremarkable. Her past history was significant for hypothyroidism and depressive symptoms. Cerebral magnetic resonance imaging with contrast revealed that the left trigeminal nerve made contact with the inferior cerebellar artery, but with no evidence of compression or distortion of the nerve.There was no contact between vessels and the right trigeminal nerve. She was initially treated with carbamazepine (1200 mg/d) with transient relief, but she complained of sedation and nausea. With lower doses, there was a reduction in intensity and number of pain bursts, but she complained of daily attacks. Clonazepam, sumatriptan nasal spray and oxygen were also administered, but without effect. She refused intravenous sumatriptan. She was pain-free for a few weeks when administered a combination of verapamil (360 mg/d) and gabapentin (900 mg/d). Two years later, the patient developed a cluster-tic headache with attacks of excruciating pain on the right side of the forehead. There was no resolution of pain between attacks, and one attack could be followed immediately by another. Marked ipsilateral lacrimation and rhinorrhea accompanied the attacks and persisted to a lesser degree in between attacks. She was unable to eat or drink. Carbamazepine (1200 mg/d), gabapentin (1200 mg/d), verapamil and pregabalin were used, without any effect.
Radiosurgical treatment was performed with the Leksell Gamma Knife (Elekta AB, Stockholm, Sweden). Following application of the Leksell G frame, under light sedation, a stereotactic MRI was performed (Siemens 1.5 T), including a high resolution T2-weighted 3D constructive interference in steady state (CISS). A bony window stereotactic CT scan was performed. Two concomitant targets (anterior trigeminal cisternal and sphenopalatine) were used. The maximum (100%) dose was 85 and 90 Gy respectively. Planning was monoisocentric for both shots and with dedicated shielding on the trigeminal nerve due to a very narrow cistern (see Figure 1).
Dose planning for cluster-tic syndrome. Upper half: dose planning for the sphenopalatine target. Single 4 mm shot to the right sphenopalatine ganglion (maximum dose: 90 Gy). A and B: fusion between a 3D T1 post-gadolinium MRI and CT scan (bone window) with Leksell GammaPlan 8.3.1 software (Elekta AB, Stockholm, Sweden); axial and coronal views (A and B respectively). Lower half: dose planning for the trigeminal nerve. Single 4 mm shot to the anterior cisternal portion of the trigeminal nerve (maximum dose: 85 Gy). C: fusion between 3D T2 CISS and CT bone window (axial view). D: fusion between 3D T1 post-gadolinium and CT bone window (coronal view). E: sagittal view of the dose planning for both targets. CISS: constructive interference in steady state.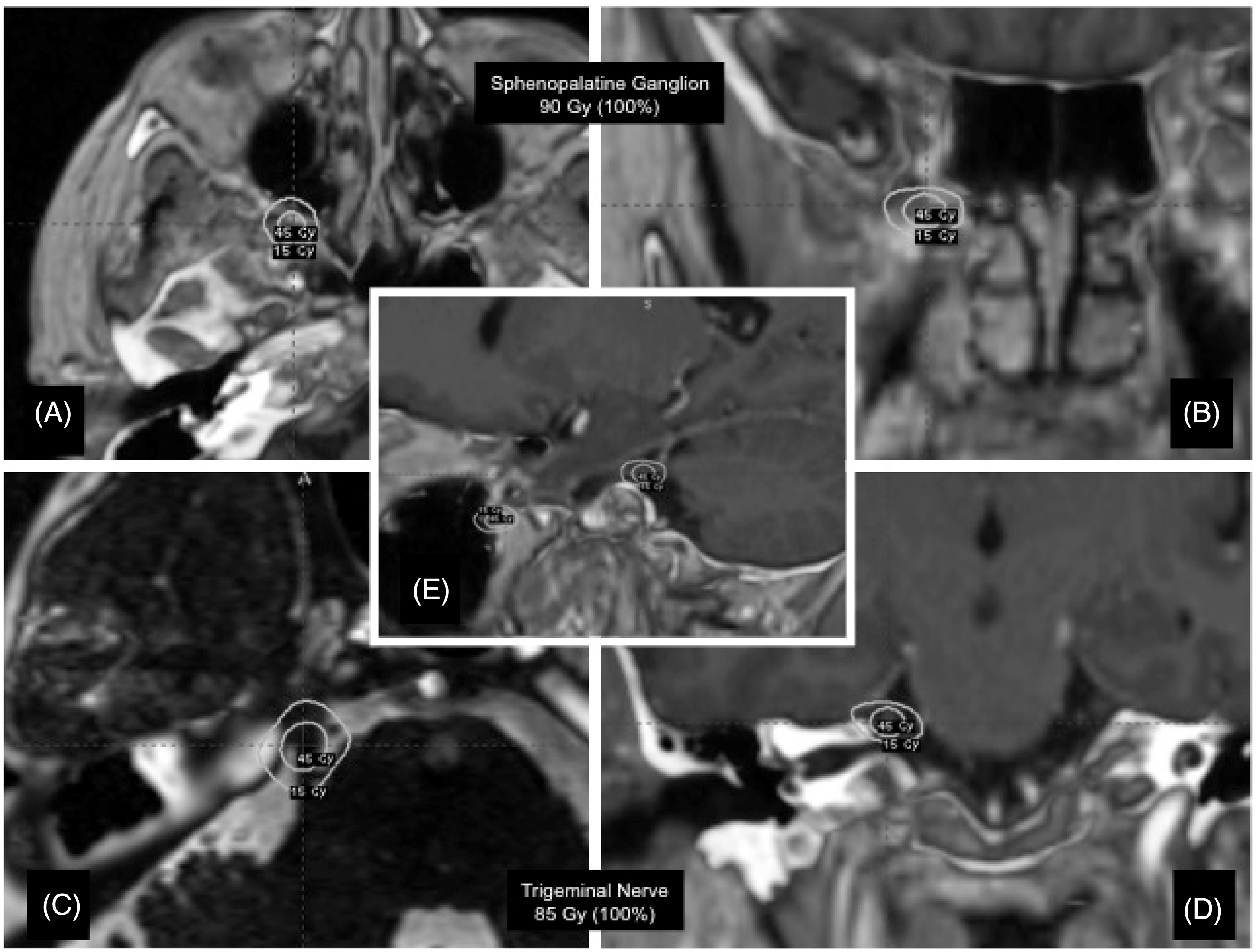
Immediately following radiosurgical treatment, the patient experienced relief of both cluster headache and TN. She stopped taking medical treatment three months after radiosurgical treatment without recurrence of the pain. Six months after GKR, she developed severe paraesthesia and sensory loss. Neurological examination showed hypoesthesia of the right V1 and V2 nerve distribution. These clinical symptoms persist to the present time. Thirty-four months after radiosurgical treatment, the patient continued to describe a complete resolution of the right-sided facial pain but also reported a real discomfort because of painful hypoesthesia. Moreover, thirty-two months after GKR treatment, she developed a typical left-sided cluster headache, with two or three nocturnal attacks daily, lasting 30–45 minutes.
The pain began around the left eye or temple, then spreading to the left upper teeth, ear, neck and shoulder and was associated with left lacrimation and rhinorrhea. There was no tic component in this new type of pain. The patient continued to refuse intravenous sumatriptan. According to the following outcome measures, the patient would be classified as a Class VI result:
Class I: pain-free without medication; Class II: pain-free with medication; Class III: pain frequency reduction >90%; Class IV: pain frequency reduction between 50 and 90%; Class V: no significant reduction in pain frequency; Class VI: pain worsening.
Discussion
The actual physiopathology of cluster-tic syndrome is unknown, but the coexistence of cluster headache and TN in a single patient prompts the suggestion that cluster headache and TN share a common pathophysiology. The existence of hypothalamic activation in cluster headache attacks (6) and the fact that hypothalamic stimulation is effective both in cluster headache and in refractory TN due to multiple sclerosis (7), suggest that hypothalamic dysfunction might play a major role in trigeminal pain. Leone (8) proposed that in these rare forms of primary headache, a disturbance of hypothalamic neurotransmitter regulation may lead to the pathological activation of the trigemino–hypothalamic pathway, and hence of the trigeminal nucleus caudalis. The source of the autonomic symptoms was hypothesized to be either the trigeminal discharge itself, dysregulation of the autonomic centres, or compression of pericarotid sympathetic fibres due to vasodilatation or perivascular oedema, or to be the result of parasympathetic overactivity during attacks.
Previously, surgical therapy for cluster headache was directed at interrupting the trigeminal nerve by chemical ablation, balloon compression, or by partial or complete surgical section of the trigeminal root. Other procedures have been developed for patients with intractable chronic cluster headache using hypothalamic deep brain stimulation or occipital nerve stimulation. GKR is a classical, minimally invasive alternative management option for TN (9,10). The radiosurgical trigeminal nerve target has also been used for the treatment of intractable chronic cluster headache with a moderate clinical outcome and a high rate of trigeminal sensory loss (11,12). The sphenopalatine ganglion (SPG) has autonomic components and has been implicated in the pathophysiology of cluster headache.
As the SPG is a parasympathetic relay for the autonomic fibres of the facial nerve towards the lacrimal and nasal mucosal glands, it appears to be a target of special interest for destructive or stimulating procedures. Indeed, the SPG is another target used both for acute (13) and preventive treatment of cluster headache (14). GKR treatment of the SPG is a new approach for intractable cluster headache. Five patients have been treated with a SPG GKR target (15–18; patient 9 in 19) and eight other patients with a dual target (TN and SPG GKR) (19). Regarding other types of trigeminal autonomic cephalalgias, one patient was treated successfully for short-lasting, unilateral, neuralgiform headache with conjunctival injection and tearing (SUNCT) syndrome using a dual target approach (20).
Comparison between the rates of hypoesthesia in patients treated with GKR for trigeminal neuralgia, cluster headache, SUNCT and cluster-tic

GKR: gamma knife radiosurgery; SUNCT: short-lasting unilateral neuralgiform headache with conjunctival injection and tearing; TN: trigeminal neuralgia; SPG: sphenopalatine ganglion; LGK: Leksell gamma knife; BNI: Barrow Neurological Institute (pain intensity score); CCH: chronic cluster headache; CH: cluster headache.
This finding is in contrast to the literature on radiosurgery for TN, which has demonstrated a low rate of hypoesthesia following trigeminal nerve radiosurgery (9,10). This shows that trigeminal nerve sensitivity to radiosurgery can be extremely different depending on the underlying pathological condition, and that there is an abnormal sensitivity of the nerve in cluster headache patients. The higher rate of trigeminal dysfunction in patients with cluster headache compared to patients with TN is not clearly understood. Kano et al. (19) suggest that patients with cluster headache are more sensitive to axonal degeneration and sensory dysfunction after radiosurgery. Is the nerve in TN then more resistant to radiosurgery?
An alternative hypothesis may be an abnormal sensitivity of the nerve in chronic cluster headache (11). These differences are confirmed by electrophysiological studies. Patients with TN have abnormal laser-evoked potentials. Because these potentials are mediated by nociceptive small, myelinated afferents, dysfunction of these fibres may play an important role in generating paroxysmal pain. Abnormalities of the afferent trigeminal pathway are present in patients with cluster headache, most prominently during the cluster period, and on the symptomatic side (21). The dysfunction may be located on the small myelinated fibres in TN and at the supranuclear level in cluster headache (11).
Conclusion
The trigeminal nerve of cluster headache patients shows a particular vulnerability to radiosurgery. Radiosurgery of the trigeminal nerve is an inappropriate treatment option for cluster headache and we do not recommend trigeminal nerve radiosurgery for the treatment of cluster headache and of cluster-tic syndrome (11,22).
However, the sphenopalatine target seems to be an interesting new option for the treatment of cluster headache patients. The dual targets might explain why the procedure was a success in this case of cluster-tic syndrome. Longer follow-up periods and additional studies are required to determine the long-term efficacy and long-term side effects of sphenopalatine radiosurgery both in cluster headache and in cluster-tic syndrome.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.