
Abstract
Background and purpose
Headache constitutes the most common symptom of cerebral venous sinus thrombosis (CVST), but its pathophysiology is unclear. We sought to investigate the potential mechanism for headache genesis in patients with CVST based on its imaging correlates.
Methods
A subgroup of CVST patients having headache as the predominant symptom without significant parenchymal lesion were retrospectively analysed for imaging features of vascular congestion (VC), in addition to cortical venous (CVT) and dural sinus thrombosis (DST) on magnetic resonance imaging. Headache and imaging patterns were classified into lateralized and nonlateralized phenotypes and their correlation was sought.
Results
Among 41 patients included, 28 had lateralized headache (LH group; 15 males; mean age 32.25 ± 9.19 years) while 13 had nonlateralized headache (non-LH group; six males; mean age 27.15 ± 8.65 years). Headache characteristics in both the groups were quite similar. Imaging showed VC in 39 of 41 and CVT among 35 of 41 patients, which were lateralized in 23 of 39 and 18 of 35 patients, respectively. Nearly all lateralized imaging patterns (21 of 23 for VC and 17 of 18 for CVT) occurred in the LH group and ipsilateral to (concordant) headache, while the non-LH group showed lateralized VC and CVT in only two and one patient respectively. Sinus thrombosis was lateralized in both groups irrespective of headache laterality. Whole cohort headache-imaging laterality (including patients with nonlateralized headache and nonlateralized imaging) concordance was 31 of 39, 24 of 35 and 18 of 41 for vascular congestion, cortical vein thrombosis and dural sinus thrombosis respectively.
Conclusion
Co-localization of VC and CVT with overlying headache might provide a possible explanation of headache and its laterality in patients with CVST.
Keywords
Introduction
Cerebral venous sinus thrombosis (CVST) is an uncommon but important cause of stroke, especially in young adults, accounting for about 0.5% to 1% of all strokes (1,2). Headache is the most common manifestation, and is present in over 80 to 90% of patients in most studies; sometimes it is the only clinical manifestation of CVST (1–8). The headache is often lateralized but lacks other distinctive patterns, thereby resembling other common headaches (1,5,7). In addition, lack of understanding of its pathogenesis makes it unlikely to be included among common differential diagnosis, thereby delaying the diagnosis.
Pathophysiology and underlying imaging correlates of headache in CVST are unclear; few earlier studies have suggested the role of sinus involvement in headache genesis, while others were unable to establish it (5,7).
We sought to investigate the role of vascular congestion (VC) and cortical vein thrombosis (CVT), in addition to dural sinus thrombosis (DST), as imaging correlates of headache and its laterality in patients with CVST.
Materials and methods
Study design, patient selection and data collection
We retrospectively searched our stroke unit database between January 2012 and September 2015 for CVST patients presenting with headache as the only or dominant symptom and fulfilling other inclusion/exclusion criteria.
The following inclusion criteria were used: Patients were aged 18 years or older; CVST diagnosis was based on clinical features and established by computed tomography (CT) with CT venography; magnetic resonance imaging (MRI) combined with MR venography (MRV); no mental status change or aphasia was present to interfere with the assessment of headache details (obtained from patient, to avoid reporting bias); and at least one MRI of the brain with susceptibility weighted imaging (SWI) had been made during the same admission. We excluded patients when imaging showed frank or significant (volume >10 ml with mass effect or sulcal effacement) intracerebral hemorrhage, sulcal subarachnoid hemorrhage (SAH) or patients with evidence of meningitis (clinical and/or cerebrospinal fluid analysis), which could explain the patient’s headache. Ethical clearance was obtained from the institutional ethics review board and a waiver of consent was taken.
Patient demography and headache characteristics were collected from medical records with an emphasis on headache laterality. Patients were classified based on their headache phenotypes into two groups – lateralized headache (LH) and non-lateralized headache (non-LH) groups. We decided to differentiate these two headache phenotypes as they mimic common primary headaches, which are often recognized by their laterality characteristics. Moreover, CVST-associated headaches have no other distinct semiology to allow sub-characterization. Lastly, we were interested in investigating “hemispheric” imaging correlates of headache, interpretation and correlation of which is more relevant if the laterality of the headache is taken into consideration.
The lateralized headache (LH) group was defined based on the occurrence of unilateral headache, or bilateral headache when severity was clearly worse on one side. The other group was classified as non-lateralized headache (non-LH). Any unrelated headache in the past was classified into subtypes according to the International Headache Society (IHS) classification (9). Other clinical manifestations were also noted. All patients underwent a systematic work-up for etiology/risk factors for CVST and treatment was initiated as per suggested guidelines (10). Use of analgesics, as well as hyperosmolar therapy (mannitol, glycerol) for the management of headache and raised ICP symptoms, was at the discretion of the treating clinician.
During follow-up, the presence/resolution of headache was reviewed and its severity was recorded (mild, moderate, severe). Additional clinical features, interval symptom(s) and functional disability (modified Rankin scale) were also noted.
Image analysis
All patients underwent MRI imaging on a 1.5 Tesla scanner (Aera; Siemens, Erlangen, Germany). We reviewed the following sequences: T1W, T2W and Fluid attenuation inversion recovery (FLAIR) images, diffusion-weighted imaging (DWI), SWI and MR venogram (both non-contrast and contrast enhanced MRV). All images were read by two neuroradiologists (JS and SV), who were blinded to the headache features. Imaging findings were then classified as lateralized or non-lateralized based on the following criteria.
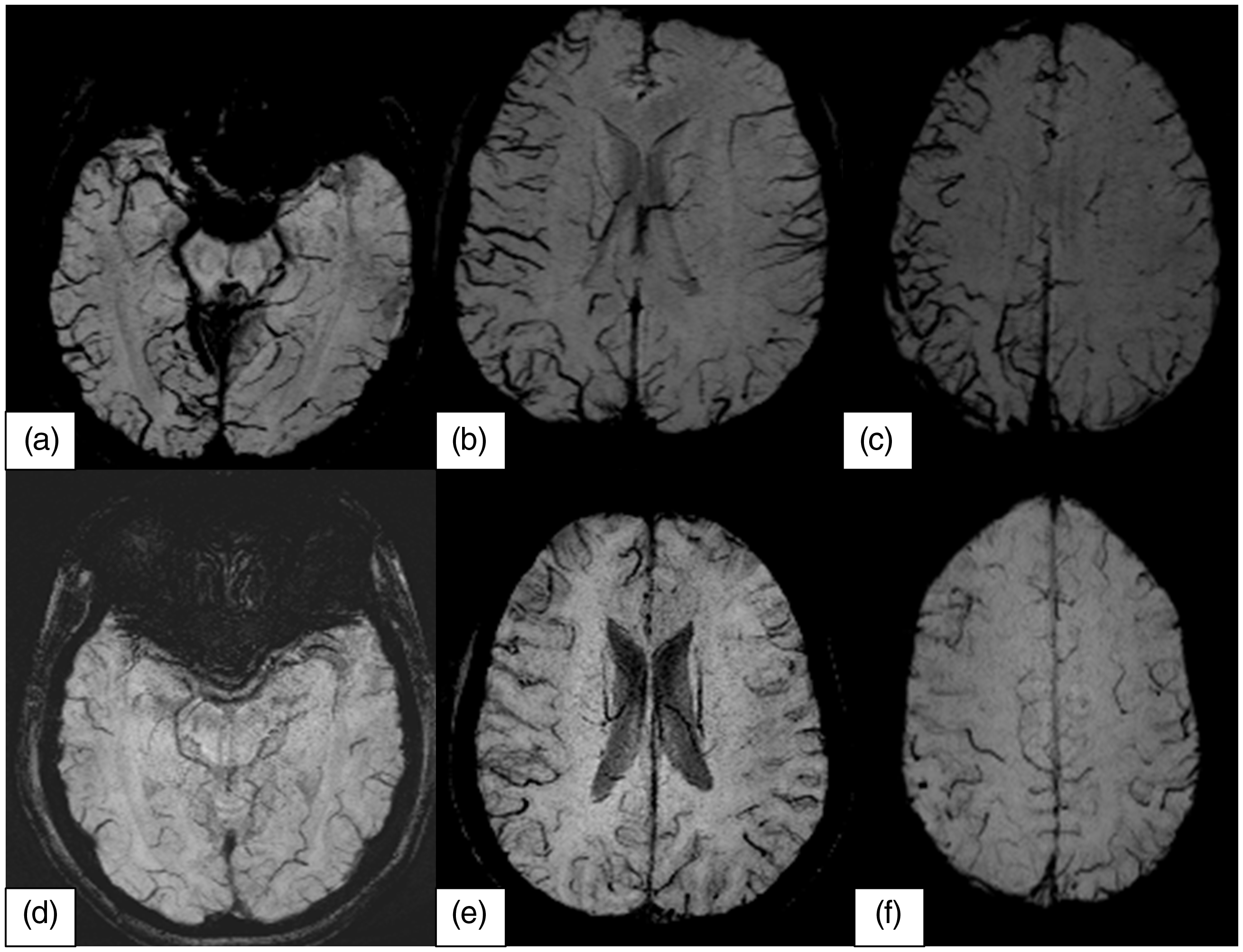
SWI images were first reviewed for the prominence of hemispheric cerebral veins, which could either denote vascular congestion or venous thrombosis. Those prominent cortical veins on SWI that were not visualized on non-contrast MRV and/or had filling defects on post contrast images were classified as being thrombosed (Figure 1), while the absence of either feature on MRV suggested vascular congestion. Vessel prominence was assessed on the axial SWI images at three different levels: Temporal (temporal horn level), ganglionic (body of lateral ventricles) and supraganglionic (above lateral ventricular level) (Figure 2). All acquired images were aligned with the anterior commissure-posterior commissure line (AC-PC line) using a multi-planar imaging workstation for standardization. Laterality was ascribed based on unilateral prominence or obvious hemispheric asymmetry in the prominence of veins in the SWI image involving at least two levels, agreed upon by both the neuroradiologists. Single prominent vessels/thrombosed veins were not regarded as a lateralized finding on SWI. Thrombosis of the cortical veins of each hemisphere was similarly assessed and the findings dichotomized based on laterality. Among the dural venous sinuses, only the transverse sinus (TS), sigmoid sinus (SigS) and jugular bulb (JugB) were used for rating the lateralization of sinus involvement, the superior sagittal sinus (SSS) and straight sinus (SS), being midline, were excluded from analysis. Results were then dichotomized as lateralized and non-lateralized findings.
Representative images in a patient with CVT that show subacute thrombosis involving left parietal vein, as indicated by the bright signal on the FLAIR images (a) and T1W images (b) with corresponding filling defect on post contrast images (d). SWI (c) shows prominent left hemispheric veins adjacent to a thrombosed vein in a patient with lateralized headache. Representative images of vascular congestion on SWI in a patient with right lateralized (LH) (a–c) and nonlateralized headache (NLH) (d–f) at different supratentorial levels.
Statistical analysis
Categorical variables are shown as the number (percent) of patients and continuous variables as mean ±SD (range). Statistical analyses of the data were performed using the χ2 test or Fisher’s exact test for nominal (categorical) data and Student’s t test or ANOVA for continuous data. For analysis, a p-value of ≤0.05 was considered significant. Data was analysed with SPSS version 16.0 for Windows (SPSS, Chicago, IL, USA).
Results
Patient and headache characteristics
Demographic and basic clinical features of CVST patients.

M = Male, F = Female; *abducent plus = abducent + other cranial nerve; †OC = oral contraceptive.
Details of headache characteristics in CVST patients.

Includes one patient who had bilateral occipital headache predominant on right side.
Follow-up revealed a resolution of headache in 16 (57.1%) and eight (61.5%) patients among the LH and non-LH groups respectively. The rest of the patients showing persisting headache reported a reduction in its severity (Table 2). No new interval symptoms were noted. Disability due to headache was mild (not interfering with daily functioning).
Imaging findings and headache-imaging correlation
Parenchymal and vascular imaging findings on MRI.

SWI = susceptibility weighted imaging.
Correlation of headache phenotype (lateralized and nonlateralized headache) with various imaging findings.

Distribution of site of headache and vascular imaging findings in all 41 patients.

Only one patient with lateralized headache lacked vascular congestion, while two patients in the non-LH group had lateralized vascular congestion. No patient demonstrated absolute discordance (contralateral side involvement) between headache and vascular congestion, though CVT did show discordance on a few occasions with regard to headache laterality (Table 5).
Discussion
The present study is the first to report the clinical relevance of vascular congestion in patients with CVST. Significant association between vascular congestion/thrombosed cortical veins with headache and its laterality suggests that they are a possible anatomical correlate of headache in CVST . This is further supported by the fact that the degree of asymmetry of vascular congestion correlates well with the laterality of headache. Patients having bilateral but asymmetrical (thus lateralized) headache had more severe vascular congestion in the ipsilateral hemisphere. A similar trend, though weaker, was also noted between cortical vein thrombosis and headache laterality.
Headache in CVST could be lateralized or bilateral, and no characteristic pattern distinguished it from other primary or secondary headaches. We and others did not observe any distinctive pattern of headache to provide a consensus on specific headache features that could be diagnostic of CVST (5–8), but we suggest that a change in pattern from a stable profile and “usual headaches” to a rapid and progressive recruiting pattern of headache in terms of frequency/severity, as seen in some of our patients with prior headaches, over a few days should alarm for possible secondary etiology, especially when associated with neurological symptoms. In such patients, imaging would be useful to exclude secondary etiologies, more so if there is no history of such prior exacerbation in their headaches.
Headache has been noted to be the most common and perhaps most important symptom in patients with CVST (1–8,11). Many factors have been postulated to explain headache, including raised intracranial pressure (ICP), sinus wall stretch, sulcal subarachnoid blood, intracerebral lesion and meningitis (5,8). The mechanism of headache in the absence of intracranial hypertension, SAH, meningitis, or intracranial lesion remains unclear and debated. This is especially important as septic etiology of CVST is becoming rare, and because, with the frequent use of imaging, many patients are increasingly being diagnosed at an earlier phase of the disease with benign clinical presentations, thus missing clinical suspicion.
Our patients either had no or minimal parenchymal involvement. Secondly, we also excluded patients with sulcal SAH or clinical/CSF features of meningitis to explain their headache. Although other factors such as intracranial hypertension could be an alternative explanation in some of our patients, headache in the presence of raised ICP is usually constant and diffuse (12) and thus lateralized headache warrants further explanation. Our study suggests that either vascular congestion and/or thrombosis of cortical veins might be important underlying factors causing headache and/or headache laterality in CVST. Stretching of the perivascular nerves of congested/dilated collaterals might explain the overlying headache and its throbbing/pulsatile quality, thus providing a headache-imaging concordance explanation as well.
Previous studies had shown vascular congestion/collaterals both on CT and catheter angiography, however its clinical relevance was not emphasized beyond diagnostic utility (13). We employed SWI to assess venous congestion and its clinical relevance. SWI is very sensitive in the detection of intravascular venous deoxygenated blood as well as extravascular blood products (14). It shows prominent veins in patients with stroke and migraine (with aura), where uncoupling between oxygen supply and demand may cause a relative increase of deoxyhemoglobin levels in tissue capillaries and the draining veins (15,16). Our observation shows asymmetric venous prominence is often seen on the sides showing cortical vein thrombosis, possibly secondary to increased opening/dilatation of venous collateral channels allowing drainage of venous blood from the ipsilateral hemisphere. Slowed blood flow in CVST allows higher oxygen extraction and higher deoxyhemoglobin levels in veins, thus making them prominent on SWI.
There are important limitations that need to be considered. Our cohort had mainly consisted of patients with combined cortical and dural sinus thrombosis, which might limit extrapolation of our data to the pure deep CVT group. The study’s smaller sample size and retrospective nature, which is understandable due to the relative rarity of CVST, requires prospective validation of the present findings in a larger cohort. Some of our patients were imaged after starting osmotherapy, which might affect vascular congestion assessment, but osmotherapy was used for all the patients of the two groups, which makes it unlikely to skew the imaging results. The low prevalence of pre-existing headache in our cohort might be due to the retrospective study design or bias arising due to the selection criteria, which might have skewed the patients included. Despite the limitations, the highly significant correlation between headache and vascular congestion/cortical thrombosis, as well as co-localization, suggest a cause-effect relationship and merit further studies to provide more insight to understand headache pathophysiology in CVST. Understanding what contributes to headache pathophysiology in this group might help in developing mechanism-targeted treatment approaches in future.
In conclusion, hemispheric vascular congestion and thrombosed cortical veins are possible underlying imaging correlates for headache and its laterality in patients with acute CVST. The asymmetry of the vascular congestion noted on SWI determines the laterality of the headache. Larger studies with SWI follow-up may provide a temporal course of vascular congestion and its correlation with headache that may further strengthen the cause-effect relationship. A prospective design with emphasis on the nature of prior headache might help to further clarify the impact of prior headaches on the presenting headache, both in laterality and semiology. Secondly, it will also provide additional clues as to when to get alarmed about potential venous stroke in patients with primary headaches. Recording of intracranial pressure during the acute and recovery phase will help in studying the interaction between ICP and vascular congestion. Moreover, studying the impact of symptomatic management on headache during the acute phase, and observing the effect on imaging, might serve as another potential approach to study the cause-effect relationship.
Article highlights
Despite headache being the most common symptom of CVST, the pathophysiology and its intracranial anatomical substrates are unclear. Hemispheric vascular congestion and cortical vein thrombosis show significant association with lateralized headache in the CVST subgroup who have no or small parenchymal lesions. No headache laterality concordance was observed with lateralized dural sinus thrombosis. Vascular congestion, either alone or in association with cortical vein thrombosis, probably underlies headache in patients with CVST who have limited parenchymal lesions. The effect of different treatment strategies on vascular congestion and cortical vein thrombosis might further define the role of these imaging markers.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.