
Abstract
Objective
To report a case series of a novel migraine subtype, which we term as episodic status migrainosus (ESM), characterized by attacks of migraine exclusively lasting more than 72 hours. We hypothesized that this would represent a novel nosologic entity, possibly an unstable migraine phenotype with a high conversion rate to chronic migraine (CM).
Methods
We conducted a retrospective review of patients diagnosed with status migrainosus at the Mayo Clinic, Rochester, between January 2005 and December 2015. All the records were then manually reviewed for patients with migraine headaches exclusively lasting more than 72 hours.
Results
We identified 18 patients with ESM, with a female predominance (15(83.3%)) and a median age of onset of 16.5 (IQR 13–19) years. The median monthly attack frequency was two (IQR 1–3), with each attack lasting a median duration of seven (IQR 4–12.5) days. Stress was the most commonly reported precipitant (11 (61.1%)). Migraine with aura was common (10 (55.6%)), as was comorbid depression (10 (55.6%)). Fifteen (83.3%) patients developed CM at a median of 7.8 (IQR 2.6–21.9) years from their first attack. There was no significant association between the time to the development of chronic migraine with either attack frequency or duration.
Conclusions and relevance
We report the existence of a novel migraine subtype, episodic status migrainosus. This migraine subtype appears to have similar clinical characteristics to episodic migraine with or without aura, except for a notably high tendency to progress to chronic migraine.
Introduction
Migraine is a common and disabling disorder affecting approximately 12% of the general population, and ranking as the seventh-highest cause of disability worldwide (1,2). The overwhelming majority of individuals with migraine experience less than 15 headache days per month, with each attack lasting between four and 72 hours, consistent with International Classification of Headache Disorders 3 (ICHD-III beta version) criteria for migraine with or without aura (3). When an attack of migraine is unremitting for ≥72 hours and associated with debilitating pain and/or associated symptoms, the patient would meet additional criteria for a complication of migraine termed status migrainosus (SM)(3).
The true prevalence of SM is not known, a disorder surprisingly being only rarely written about in the medical literature (4,5). In a retrospective review of patients encountered by a specialist headache practice in southern France, SM was only encountered in nearly 3% of the patients, with approximately one third experiencing a subsequent SM relapse (4). In our clinical practice, we have noted a minority of instances in which the exclusive migraine phenotype consists of attacks of migraines lasting in excess of 72 hours (with no shorter attacks or other migraine/headache types), prompting us to retrospectively review a larger cohort for similar cases. In this study, we report the characteristics of this novel subtype of migraine which we term, based on the clinical features, as episodic status migrainosus (ESM). We hypothesized that this would represent a novel nosologic entity, possibly an unstable migraine phenotype with a high conversion rate to chronic migraine.
Methods
Study design
We conducted a search for the following terms “Status migrainosus”, “Headaches lasting more than 72 hours/3 days” using the electronic data search system at the Mayo Clinic, Rochester, MN between January 2005 and December 2015. All the records were then manually reviewed and patients with exclusive migraine headaches lasting more than 72 hours or three days were included in our final cohort, as per the inclusion/exclusion criteria discussed below.
Study definitions
Status migrainosus was defined according to the recent definition proposed by the International Classification of Headache Disorders 3 (ICHD-III beta version) as a debilitating migraine attack lasting more than 72 hours, occurring in patients with Migraine without aura and Migraine with aura, being unremitting with pain and/or debilitating associated symptoms. Migraine with aura, migraine without aura and chronic migraine were also defined as per the definitions proposed by ICHD-III beta version (3). Effective abortive medications were defined as the drugs which completely resolved the attack, while effective preventive medications were defined as those that led to at least a 50% reduction in the attack frequencies.
Inclusion/exclusion criteria
Patients were included in the study if they 1) satisfied the above criteria for SM 2) exclusively had attacks of migraines lasting more than 72 hours/3 days, and 3) had <15 headache days per month at the onset of their ESM. The latter inclusion criteria was imposed so that our cohort could be readily distinguished as having severe, protracted migraine attacks, and distinct from individuals meeting criteria for chronic migraine. Patients were excluded from our study if 1) they had headaches or other headache syndromes lasting less than 72 hours 2) they had a history of other types of headaches 3) they had pure menstrual migraine 4) the first attack of SM lasted more than 15 days 5) they developed SM after an associated head trauma, illness, or surgery 6) they had a congenital malformation or a structural abnormality in the brain, and/or 7) they had an alternate diagnosis on prolonged follow-up.
Clinical parameters, procedures and investigations
All the patients were seen by a neurologist for a complete neurological and systemic examination. We abstracted basic demographic information, in addition to extensive history pertaining to SM attacks, including age of first migraine attack, duration of migraine, average headache intensity, precipitating factors, associated signs/symptoms with migraine, associated aura, presence of any other comorbidities, and whether a family history of migraine was present. Specific data was collected for each visit, which included the change in the migraine characteristics, effective abortives and effective preventives. We also collected data on the development of chronic migraines such as age, timing, abortives and preventive medications used. Imaging was also recorded, when available.
Ethical standards
The study was approved by the Mayo Clinic institutional review board, and all patients or their representatives signed a consent form allowing their participation in the study. The research has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Statistical methods
Continuous variables were described as median values with interquartile ranges (IQR), and nominal variables as counts and percentages. Group differences for categorical data were assessed using the chi-square test and Fisher’s exact test as applicable, while the Mann-Whitney test was used to analyze continuous variables as they were not normally distributed. All statistical tests were 2-sided and p ≤ 0.05 was considered to be statistically significant. Statistical analyses were performed using the JMP 11.0.0 (SAS Institute Inc., Cary, NC, USA).
Results
We identified 532 patients in our preliminary search, who had a diagnosis of “status migrainosus”. After excluding patients using the above mentioned exclusion criteria, our cohort consisted of 20 patients, who had an exclusive phenotype of migraines lasting more than 72 hours. We then excluded two additional patients because their first headache attacks lasted more than 15 days (20 days and 3 months), putting them in the category of chronic migraine. All included individuals were evaluated in the Mayo headache clinic, where a detailed standardized intake questionnaire allowed us to exclude the presence of medication overuse headache in any case.
Clinical characteristics and presentation
Demographics and migraine characteristics.

Data is expressed as number (%) or median (interquartile range)
Individual characteristics for the patients included in our cohort.

The abortive medications when used alone were effective in only five (27.8%) patients, while 13 (72.2%) patients required multiple combinations of medications. Specific details of the individual patient’s effective and ineffective abortive and preventive medications are shown in Table 2. No patients were identified who met the criteria for medication overuse headache based on the reported details in their records.
Fifteen (83.3%) patients in our cohort developed chronic migraine at a median age of 26.8 (IQR 18.2–44.2) years. The median duration between the onset of first headache to the development of chronic migraine was 7.8 (IQR 2.6–21.9) years. A Kaplan-Meier curve showing the time to the development of CM is shown in Figure 1. The details of the individual patient medications and the time to the development of CM are shown in Table 2.
A Kaplan-Meier curve showing the time to the development of chronic migraine from the first attack of episodic status migrainosus.
There was no significance between the time to the development of CM from the first attack of migraine and headache duration (p = 0.358), headache intensity (p = 0.995), average number of headaches/month (p = 0.912) or the age of first attack (p = 0.362). Patients tended to develop CM earlier if DHE (2.5 vs 13.3 years, p = 0.083) and opioids (p = 4.7 vs 9.5 years, p = 0.648) were used as abortives. However none of the associations were statistically significant, possibly because of the small sample size.
Discussion
In this study we describe and define a novel migraine subtype we are labeling “episodic status migrainosus”. These patients present with an exclusive phenotype of migraines lasting more than 72 hours and their headache attacks are generally protracted. Based on our experience, we propose diagnostic criteria for this condition in Figure 2. We observed that most of the patients presenting with episodic status migrainosus tend to progress to CM, although this could not be related to specific features of the disorder in our small cohort.
Proposed diagnostic criteria for episodic status migrainosus.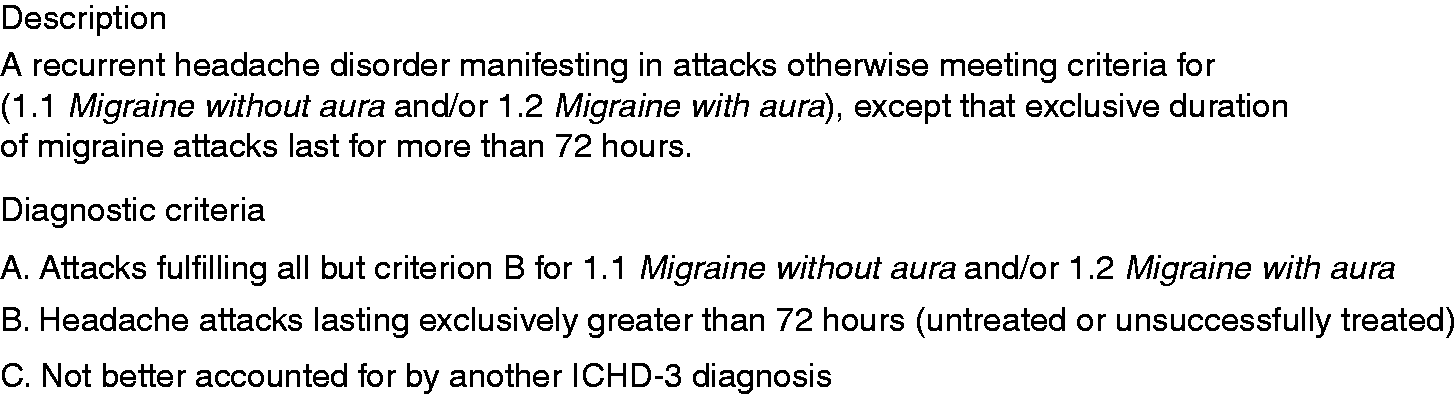
SM is reported to be a rare complication of migraine, present in nearly 3% of patients, the majority (84%) of whom have migraine without aura (4). In our cohort, ESM patients more commonly presented with migraine with aura (55.6%). Emotional stress, depression, analgesic overuse, and menstruation have been reported to be the main precipitating factors for SM (5). While we did not encounter cases of medication overuse headache, we did identify stress, sleep deprivation, and menstruation as common precipitants.
While our report is uncontrolled and retrospective, it is notable that osmophobia was reported by approximately two thirds of our patients, as this feature is thought to have poor sensitivity, but strong specificity in the diagnosis of migraine (6,7). In addition, it is notable that both nausea (85%) and vomiting (50%) were common in our cohort, as this may be an independent risk factor for CM progression (8). In addition, nausea has been associated with impaired quality of life in migraine (9). Clinically diagnosed depression was also very common in our cohort (55.6%), which appeared to be disproportionate to the 5–17% prevalence reported in the general migraine population, and is also noted to be a risk factor for CM progression (10,11).
Nearly 15/18 (83.3%) patients with ESM went on to develop CM over the next eight years. Two of the three patients did not have a follow up visit and the third patient didn’t develop CM after a follow up of nearly five years. Hence, patients with ESM appear to represent an unstable phenotype, who are at a high risk for the development of CM. Similar to that observed in the general migraine population, a trend was noted for more rapid development of CM in individuals exposed to opioids. Given that the majority of patients were seen as referrals for consultation, and in some cases had already progressed to CM at the time of their initial encounter, the diagnosis of ESM had to be made by virtue of a detailed clinical history.
Overall, the clinical features of our cohort support the presence of a novel migraine variant defined by the strict occurrence of protracted migraine attacks lasting more than 72 hours, noted to have a median headache duration of seven days in our series. The presence of otherwise characteristic migraine symptoms supports the hypothesis that this subtype is pathophysiologically similar to episodic migraine with or without aura. Individuals with pure menstrual migraine were excluded, since menstrual migraines may be more likely to result in longer duration attacks, therefore creating the potential for confusion with a preexisting diagnostic entity (12). While a high conversion rate to CM is noted in our series, we cannot conclude whether this observation is inherent to the unique migraine phenotype, and/or a function of comorbidities (i.e., depression, opioid exposure) also. The abrupt, protracted nature of the attacks is of significant pathophysiologic interest, as understanding the nature of the on-off switch may advance our understanding of allied conditions such as acute migraine, chronic migraine, and new daily persistent headache.
The main limitations of this study are inherent to the retrospective design and the small size of the cohort. The cohort was derived from patients seen at a tertiary referral center, therefore including some individuals who were not followed longitudinally. Furthermore, the retrospective nature of the study also prevented us accurately reporting the specific pattern of abortive medication use (i.e. days in a row), although we can confidently report the absence of medication overuse headache based on the reported details in the medical records. We were not able to characterize the associated auras beyond application of standard criteria, as sufficient data were not available. The limited sample size, possibly reflecting the rarity of the syndrome, precluded logistic regression analysis to identify risk factors in our cohort for the development of CM. Further prospective studies are needed to identify these patients, understand the nature of the recurrent, protracted attacks, and to explore the factors that might lead to the development of CM in these patients. Future work, looking at subsets of patients with either episodic or chronic migraine who also experience relapses of status migrainosus, would also be of interest to study as potentially unique clinical and prognostic subtypes.
Conclusions
Episodic status migrainosus is a disorder characterized by attacks otherwise meeting criteria for migraine with or without aura, except for an exclusive attack duration greater than 72 hours. The clinical features are similar to migraine, except for what appears to be a very high propensity for progression to chronic migraine. Prospective evaluation is required to definitely include ESM as an independent nosologic entity. Further studies are is necessary to better characterize the nature of the protracted migraine attacks and progression to chronic migraine observed in this condition.
Article highlights
In this study we describe and define a novel migraine subtype, which we are labeling as “episodic status migrainosus”. Individuals with ESM present with an exclusive phenotype of migraines lasting more than 72 hours, and their headaches attacks are generally intense and protracted. Individuals with ESM appear to have an unstable migraine phenotype with a high tendency to progress to chronic migraine.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.