
Abstract
Objective
Neck-Tongue syndrome (NTS) is characterized by brief attacks of neck or occipital pain, or both, brought out by abrupt head turning and accompanied by ipsilateral tongue symptoms. As the disorder is rare, we undertook a systematic review of the literature to identify all reported cases in order to phenotype clinically the disorder and subsequently inform clinical diagnostic criteria.
Methods
Two electronic databases were searched using the search term “neck tongue syndrome”. All English language references were reviewed in full. Cases were abstracted using a standardized abstraction form and the references of the retrieved articles were reviewed by hand to identify additional references and cases. Conference proceedings from recent headache meetings were searched. We also report six new cases from our centers.
Results
There were 39 primary cases, 56% of which were female. Mean age (SD) at onset was 16 (12) years. Twenty (53%) experienced neck pain, seven (18%) occipital pain, and 11 (29%) both. Pain was most often sharp or stabbing and severe, lasting several seconds to several minutes. Eleven experienced numbness and/or tingling in the neck/occiput following the pain. Thirty-six had an accompanying tongue sensory disturbance and three a motor/posture disturbance; five had both. Thirteen had other headaches, and four a family history of Neck-Tongue syndrome.
Conclusions
Neck-Tongue syndrome typically has pediatric or adolescent onset, suggesting that ligamentous laxity during growth and development may facilitate transient subluxation of the lateral atlantoaxial joint with sudden head turning. Familial cases suggest a genetic predisposition in some individuals. Neck-Tongue syndrome should be re-instated in the International Classification of Headache Disorders.
Keywords
Introduction
Neck-Tongue syndrome is a relatively rare headache disorder characterized by brief attacks of neck and/or occipital pain that are brought out by abrupt head turning and accompanied by ipsilateral symptoms in the tongue. While the first case was described by Cyriax (1), Lance and Anthony were the first to provide a detailed neuroanatomic explanation for the disorder in 1980 (2). Neck-Tongue syndrome was included in the second edition of the International Classification of Headache Disorders (ICHD) (3), but was removed from the beta version of ICHD-3 (4). No reason for this decision was made public. One possibility is that perhaps Neck-Tongue syndrome was thought to be inadequately characterized. Diagnostic criteria are needed to help clinicians recognise and correctly diagnose the disorder, and the inclusion of Neck-Tongue syndrome in the final ICHD-3 may be warranted. We undertook a systematic review of the literature of all published cases of Neck-Tongue syndrome, and describe additional cases from our own practices, in order to help inform our understanding of the clinical phenotype and the underlying neuroanatomy, as well as to guide revision of the ICHD. In addition, our observations of the onset have led us to consider the aetiopathogenesis, which has hitherto not been clarified.
Methods
Two electronic databases were searched using the search term “neck tongue syndrome”. Pubmed was searched on 2 December, 2014. Science Direct (on the journal articles setting) was searched on 17 December, 2014. All English language references were reviewed in full by the search author (AAG). Cases were abstracted using a standardized abstraction form in REDCap (Research Electronic Data Capture) (5), a secure web-based application designed to support data capture for research studies. The references of the retrieved articles were reviewed by hand to identify additional references and cases. The cases were independently reviewed by a second author (HJ) and discrepancies were resolved by consensus.
Conference proceedings from recent headache meetings were electronically searched for “neck tongue syndrome” and “tongue”. Specifically the following conference proceedings were searched: American Headache Society scientific meeting 2011 (6), 2012 (7), 2014 (8), and 2015 (9,10); the joint International Headache Congress/American Headache Society scientific meeting 2013 (11); the International Headache Congress 2011 (12) and 2015 (13); and the European Headache and Migraine Trust International Congress 2010 (14), 2012 (15) and 2014 (16).
In addition, we report six additional cases of Neck-Tongue syndrome from the authors’ centers. The UCSF Institutional Review Board served as the privacy board for the cases.
Case criteria
Criteria for including a case of Neck-Tongue syndrome in the main analysis were set a priori. The case report had to be written in English and provide at least basic demographic information, specifically age and sex. For the analysis we required that the patient’s symptoms be episodic, given that the etiologies of those who have transient episodic symptoms with head turning are likely different from those who have persistent symptoms that simply worsen with head turning. This is also consistent with the diagnostic criteria that had existed for Neck-Tongue syndrome in ICHD-2 (3), which indicated symptoms should last just seconds to minutes. Symptoms had to be precipitated by sudden head movement and involve, at a minimum, a pain component in the neck, or occiput, or both, and a sensory or motor component, or both, in the tongue occurring simultaneously with, or immediately following, the neck/occipital pain. If the individual’s symptomatology was not described thoroughly enough to meet these criteria, the report was not included.
Definition of symptom duration
When a range was given for a symptom’s duration, for example “several seconds to several minutes”, the upper end point was chosen to best illustrate the longest attack duration of the episodic, presumably primary, form of Neck-Tongue syndrome, to help clinicians better differentiate it from the situation where patients have constant symptoms.
Analysis
Data were analyzed using STATA v13.0 (College Station, TX). All analyses were descriptive.
Results
Literature search
The Pubmed search yielded 27 returns, of which 20 were in English. All 20 references were reviewed in full by the search author (AAG). The references of these 20 (2,17–35) were reviewed by hand to identify additional references, leading to the identification of 11 additional references: ten articles (1,36–44), and one abstract (45), all of which were reviewed.
The ScienceDirect search yielded four results, of which three were redundant (25,34,35) and one was a novel abstract (46). A review of conference proceedings identified three novel abstracts in which an additional five cases were reported (47–49), as well as two abstracts referring to earlier versions of this systematic review (50,51), which were ultimately removed as self-referential duplicates, as was the abstract by one of the co-authors (48) that refers to three of the new cases being presented here but did not provide clinical details of the cases. A PRISMA flow diagram depicts this process (Figure 1).
PRISMA flow diagram for Neck Tongue syndrome systematic review.
In total, 61 cases described as “Neck Tongue syndrome” were found in the literature. Of these, 28 did not meet the inclusion criteria for the primary analysis: 19 because the patients had persistent symptoms (i.e. presumptively the neck and tongue symptoms were being produced by a secondary cause) and nine cases did not provide adequate clinical detail to be abstracted (1,37,38,46). The cases with persistent symptoms were excluded from this analysis.
The remaining 33 cases of episodic (i.e. primary) Neck-Tongue syndrome were included.
New cases
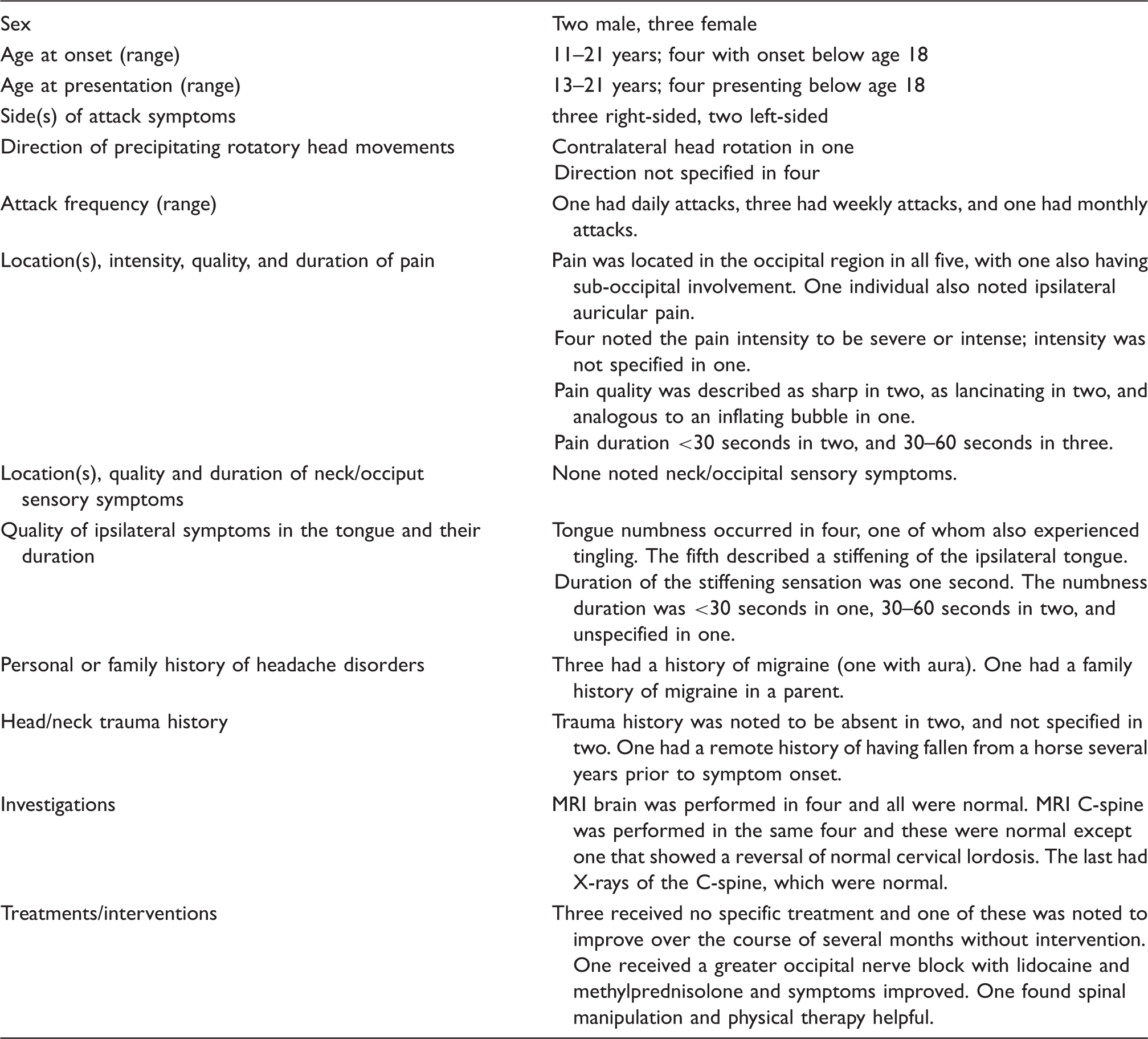
Summary of five new cases of Neck-Tongue syndrome.
Illustrative case
A 16-year-old girl has episodes of sharp and shooting neck pain triggered by neck movement, most often on the left but sometimes on the right. With these, the ipsilateral side of her neck would feel numb. She would also feel numbness and a “fuzzy” feeling in the tongue and sometimes the shoulder. The tongue would also feel a little stiff. Symptoms typically lasted about 30 seconds. She could recall episodes since pre-school (age three or four), which were initially more frequent but now occurred about once a month. General and neurologic examinations were normal. MRI of the cervical spine was normal. She also had a history of post-traumatic headache following two concussions, but these did not occur until age 14 and age 15. The mother had migraine. The maternal uncle (half-brother to the mother) reportedly had similar episodes of the neck and tongue symptoms.
See Table 1 for the additional five cases.
Analysis of all cases
There were 39 cases included in the primary analysis (33 from the literature and six reported here). Twenty-two (56%) were female and 17 (44%) male. Average age at case description was 23 years (SD 13; range 10–59). Age at onset of Neck-Tongue syndrome was reported in 31 cases (80%). Of these, age at onset of Neck-Tongue syndrome was most commonly in the pediatric or adolescent age range: mean 16 years (SD 12; range 3.5–57 years; see Figure 2). Twenty-three of these 31 (74%) had onset of Neck-Tongue syndrome under age 18, and 25 (81%) had onset at or below age 21. The remaining eight cases of the original 39 did not have age at onset clearly specified, however, the five adolescents in the Lewis et al. series were ages 12–16 years at the time of their case write-ups, so all must have been under age 18 at Neck-Tongue syndrome onset (27). As for the final three cases, one was described as having had “attacks since childhood” (17), one seemed to have onset in their 20's (33) and one in their 30's (39). All told, 29/39 (74%) of the cases had onset before age 18.
Age at onset of Neck Tongue syndrome (n = 31).
Lateralisation
The affected side was reported in 37 cases. The right side was involved in 19 (51%), left side in 15 (41%) and either side (one side at a time) in three (8%). The direction of head turn that precipitated the symptoms was reported in 24. In eight (33%) symptoms were precipitated by ipsilateral head turning, contralateral head turning brought it out in four (17%), and either side could bring it out in 12 (50%).
Pain features
With the episodes, only eight patients experienced pain solely in the occiput (21%), while 20 (51%) experienced pain just in the neck, and 11 (28%) had pain in both locations. Pain quality was reported in 25 (64%). It was most often sharp or stabbing (n = 20, 80%). Pain intensity was only explicitly described in 17 (44%), but was generally severe (n = 14, 82%) or moderate (n = 3, 18%). The duration of occipital and/or neck pain was most commonly on the order of a few seconds (n = 11, 41%), though 30–60 seconds (n = 10, 37%) and several minutes (n = 6, 22%) were also reported among the 27 where information on duration was given. In 11 cases, dysesthesia in the occiput and/or neck was also reported: five with numbness, two with paresthesias, two with both, and two described some other type of sensory disturbance. In five cases the dysesthesia lasted several minutes, in three it lasted a minute or less and in one it lasted longer than five minutes.
Sensory symptoms
Sensory symptoms in the tongue occurred in 36 of 39 cases (92%). The other three had solely motor symptoms in the tongue, while five had both sensory and motor tongue symptoms. The quality of the tongue sensory symptom was described in 35; numbness was the most common (n = 22, 63%), tingling in eight (23%), both in four (11%) and “other” in one (3%). The duration of sensory symptoms in the tongue was reported in 29, and ranged from a few seconds to a few minutes. Specifically, a few seconds in nine (31%), 30–60 seconds in 10 (35%) and a few minutes in nine (31%), with only one patient (4%) experiencing symptoms for longer than five minutes.
Motor symptoms
For the eight patients who had motor symptoms in the tongue, five (63%) described it as a pulling or twisting quality, two (25%) as abnormal posture or stiffness, and just one (13%) as weakness. Motor symptoms in the tongue lasted a few seconds in three (43%), 30–60 seconds in one (14%), a few minutes in two (29%) and more than five minutes in one (14%); in one case duration was not specified.
Frequency of attacks
Attack frequency ranged from as high as four times per day to once or twice a year. In some individuals attack frequency varied over time. In seven cases, attacks were specifically noted to come out with physical activity (2,17,19,35,44), particularly activities that involve head turning such as swimming free style, dance or figure skating (19,35). In another case, frequency was noted to go down with limiting activity (34) and in two varied with activity level (35,47).
Other accompanying symptoms
Dysarthria (27,33) (three cases), alteration in voice (one case) (47), or inability to speak (17) (one case) were noted in several cases, and in one case the individual felt a choking sensation with particularly severe attacks (19). Two patients also noted numbness of the palate/oropharynx (1,33)
One person experienced ear pressure (33), another had nasal congestion and sialorrhea (33), and another occasional bilateral lacrimation (she also had migraine) (45). One patient also had numbness in the mastoid area (2), one dysesthesia in the mandibular area (39) and one facial paresthesias (33).
Upper extremity symptoms, specifically numbness or paresthesias of the fourth and fifth fingers, were accompanying symptoms in three (2,33). Numbness in the shoulder occurred in one case (the illustrative case presented here), paresthesias in the inner scapular area in one (1), and pain in the trapezius in two (33,39). One patient had a sensory deficit in the left ulnar distribution on examination, and MRI showed degenerative changes at C6–7 (17).
One patient noted that about twice a day his head would fall back and he would feel a click (2). Another noted a popping sensation with attacks (34). Two noted that in the few minutes after an attack Due to spontaneous head movement, they could precipitate another attack with intentional head turning (17,36). Two were noted to have a mild head tilt on exam (17,34), though one had a history of congenital torticollis (17).
Potential aetiologies vs. incidental findings
There was a family history of Neck-Tongue syndrome noted in four cases, all of whom were adolescents (the illustrative case reported here, and three cases reported previously in the Lewis series) (27). As mentioned above, several cases came out more with physical activities involving head turning.
One patient’s episodes began as a child after being hit in the head by a swing at age eight (2), and another child’s episodes began after neck trauma in gymnastics (34). In two adult onset cases, episodes began following accidents – one after a motorcycle accident and one after a motor vehicle accident – though in one the episodes began a couple of years after the accident (33,39). Similarly, in one child episodes began several years after falling off a horse (48). Two women in their late 50's and one woman aged 40 had mild degenerative joint disease of the cervical spine (17,33,45). Narrowing of the peri-odontoid space was reported in two cases (28,35). MRI of the brain demonstrated tonsillar descent of 10 mm in one case (21) and a retrocerebellar arachnoid cyst in another (44). One patient’s attacks began about a month after having been seated for a 10-hour period, which the authors speculated had somehow precipitated the attacks (28).
In 13 cases (33%) the patients were noted to also have another type of headache disorder, and in three a family history of headaches (other than Neck-Tongue syndrome) was noted. In one case, Neck-Tongue syndrome attacks seemed to precipitate migraine headache (45), and in another the patient was more susceptible to Neck-Tongue syndrome attacks during migraine episodes (39).
Treatment
Treatment was not commented upon in the majority of cases. Three cases from the same series mentioned spinal manipulation therapy being helpful, including the case where symptoms began after a motor vehicle accident (39). A fourth case, where X-rays showed narrowing of the left peri-odontoid space, also reported spinal manipulation therapy to be helpful (34). One patient improved after a manipulation and physical therapy (see Table 1). Two found symptoms decreased with use of a cervical collar alone; one of these was the 57-year-old woman with degenerative joint disease and the other was the girl whose symptoms began after neck trauma in gymnastics (33,34). A third, whose symptoms began at age four, reportedly found a cervical collar combined with exercises to be helpful (47). One patient improved with amitriptyline (34), one found a nerve block helpful (Table 1), and one improved with a combination of gabapentin, NSAIDs and rest (28).
Discussion
The shared features of the 39 cases of Neck-Tongue syndrome summarized in this systematic review allow for a description of the clinical phenotype of the disorder: Neck-Tongue syndrome attacks are precipitated by sudden turning of the head and manifest as several seconds to several minutes of intense sharp pain in the neck, occiput, or both, along with ipsilateral sensory symptoms in the tongue. Sensory symptoms may also occur in the affected neck and occipital areas. Three-quarters of cases have their onset in the pediatric or adolescent age range.
Neck-Tongue syndrome appears to be a rare disorder, though some have suggested it is perhaps underdiagnosed or underreported (30,35). In a population-based study in Norway, the prevalence was 0.2% (17). A neuroanatomic explanation for Neck-Tongue syndrome was first proposed by Lance and Anthony and then supported with cadaveric dissection by Bogduk (30,31). With sudden turning of the head, a temporary abnormal subluxation at the lateral atlantoaxial joint can cause the C2 ventral ramus to become impinged against bone, as the C2 ventral ramus lies dorsal to the lateral atlantoaxial joint capsule. Sensory symptoms in the ipsilateral neck/occiput may result from compression of the C2 ventral ramus, and/or stretch of the C2 spinal nerve or its roots. Stretch on the joint capsule, which is innervated by the C2 ventral ramus, has also been hypothesized to be the source of the pain (31).
As for the tongue symptoms, afferent proprioceptive fibers from the lingual nerve (trigeminal origin) anastomose with the hypoglossal nerve within the tongue, then travel through the ansa cervicalis to continue cephalad via the ventral ramus of the C2 spinal nerve (31); therefore, compression of the C2 ventral ramus will also produce symptoms in the ipsilateral tongue (see Video 1). In rhesus monkeys, hypoglossal afferents have been shown to enter the central nervous system through the C2 and C3 ventral rami. The fact that several patients report a popping or clicking sensation or sound with episodes, or the ability to voluntarily elicit an attack for a brief period after a spontaneous one, suggest that temporary abnormal subluxation is indeed the initiating event in a Neck-Tongue syndrome attack (2,17,34,36).
Bogduk makes the point that the “numbness” in the tongue may not be due to true sensory loss but rather a result of altered proprioception in the tongue, analogous to the sensory complaints patients with Bell’s palsy may experience (30). It could be that changes in proprioceptive signaling lead to the dysarthria noted in some patients, as ability to judge tongue position while speaking could be impaired. Others have suggested that glossopharyngeal branches might also be involved in Neck-Tongue syndrome, either via direct anastomoses to the hypoglossal nerve or through anastomoses within the pharyngeal plexus, which could explain sensory involvement of the palate reported in some cases (2,33).
Bogduk also notes that the C2 ventral ramus innervates portions of the posterior face as well as skin over the mastoid process, hence the facial and retro-auricular symptoms described by some patients can be neuro-anatomically explained without necessarily invoking involvement of the trigeminal nerve (30). The neuroanatomic explanation for the upper extremity tingling that some patients experience is not clear, though Lance and Anthony suggest it may be due to traction on the dura mater during rotation putting tension on the lower cervical nerve roots (2).
An important observation about Neck-Tongue syndrome is that onset is most commonly during childhood or adolescence. Perhaps this is due to increased ligamentous laxity during growth and development leading to easier lateral atlanto-axial joint subluxation, either spontaneously or following minor neck trauma of childhood. Decreased range of motion with older age might also contribute to decreasing the likelihood of symptoms in older individuals. Increased ligamentous laxity could also be genetically mediated as there were several familial cases reported, including one of our own (38,44). Of note, increased laxity of peripheral joints has been noted on examination in some cases (38). Alternatively, subtle bony abnormalities of the atlas or axis might conceivably predispose to this condition (2,46).
Work-up and treatment of the episodic, primary form
Although the condition implies some degree of instability, that instability is in the transverse plane. Its demonstration would require axial CT scanning or biplanar fluoroscopy, under extremes of rotation. Since these investigations need to be undertaken carefully, they are not advocated as routine investigations. If Neck-Tongue syndrome develops following head or neck trauma, or beyond the adolescent or young-adult age range, imaging may be needed and in these situations it ought to be performed by experienced neuroradiologists with close communication between the imaging team and the treating clinician about the suspected type of instability. Most Neck-Tongue syndrome cases do not seem to require treatment, as attacks are not necessarily frequent and typically last just seconds to several minutes. The benefit of spinal manipulation therapy in these patients is far from proven, and the risk of arterial dissection from chiropractic manipulation would be a possible concern (52). If attack frequency is increasing, or attacks are bothersome to the patient, a period of rest or activity modification could be recommended.
Persistent neck-tongue symptoms
Persistent symptoms of tongue numbness and occipital/upper neck pain may have an underlying pathology and should be investigated. Patients with known rheumatic disease of the cervical spine, such as ankylosing spondylitis or psoriatic arthritis (38), may be at higher risk for underlying pathology and need appropriate investigations. It has been hypothesized that spasm of the inferior oblique muscle might put pressure on the C2 dorsal root ganglion and ventral ramus (40), thereby eliciting continuous symptoms that become further exacerbated by head turning, though neuroanatomically this seems a challenging explanation. Some patients with persistent symptom presentations have been reported to respond to C-spine immobilization, spinal manipulation therapy, or surgery to stabilize the cervical spine (32,38,40). However, if atlanto-axial instability plays a role in these persistent cases, spinal manipulation therapy would be contra-indicated (40).
Proposed diagnostic criteria for Neck-Tongue syndrome for ICHD-III
As occipital head pain is a common symptom of Neck-Tongue syndrome, we recommend Neck-Tongue syndrome be re-instated in ICHD-III. Diagnostic criteria are needed to help clinicians to recognise Neck-Tongue syndrome and to make a diagnosis. We reviewed the language of the ICHD-2 criteria (3) and propose revised criteria for consideration:
Description
The sudden onset of occipital and/or upper neck pain brought out by sudden rotatory head movement and accompanied by abnormal sensation and/or posture of the ipsilateral tongue. The pain is usually severe in intensity.
Diagnostic criteria:
At least two episodes that fulfill criteria B through E Sharp or stabbing unilateral pain in the upper neck, or occipital region, or both, precipitated by sudden turning of the neck, with or without simultaneous dysaesthesia. Concurrent abnormal sensation, or posture, or both, of the ipsilateral tongue Duration from several seconds to several minutes Not better accounted for by another ICHD-3 disorder
Based on the results of this systematic review, we recommend Neck-Tongue syndrome be reintroduced into the ICHD classification system, as it is a well-described syndrome with a neuroanatomic explanation. Given the early age at onset of the majority of presentations, Neck-Tongue syndrome may represent a neurodevelopmental syndrome with a ligamentous pathogenesis.
Clinical implications
Neck-Tongue syndrome is a well-characterized disorder that clinicians can learn to recognize. Patients experience brief attacks of pain in the neck/occipital region with rapid rotatory movement of the head, along with ipsilateral sensory changes in the tongue. Onset is most often in childhood or adolescence. Management is most often supportive.
Footnotes
Contributors’ statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Amy A Gelfand receives grant support from NIH/NCATS (8KL2TR000143-09), the Migraine Research Foundation, and the UCSF Center for Translational Science Institute. She has received honoraria from Journal Watch Neurology, personal compensation for legal consulting, and consulting fees from Eli Lilly and Zosano as well as travel expenses from Teva.
Hannah Johnson, Marc EP Lenearts, Jessica Litwin, Charles DeMesa and Nikolai Bogduk report no disclosures. Peter J Goadsby reports grants and personal fees from Allergan, grants and personal fees from eNeura, personal fees from Autonomic Technologies Inc, grants and personal fees from Amgen, personal fees from AlderBio, personal fees from Pfizer, personal fees from DrReddy, personal fees from Zosano, personal fees from Colucid, personal fees from Eli-Lilly, personal fees from Avanir, personal fees from Gore, personal fees from Heptares, personal fees from Nupathe, personal fees from Teva, personal fees from Cipla, personal fees from Ajinomoto, personal fees from Akita, personal fees from Wells Fargo, personal fees from Ethicon, personal fees from Promius, personal fees from MedicoLegal work in headache, personal fees from Journal Watch, personal fees from Up-to-Date, outside the submitted work; in addition, Dr. Goadsby has a patent magnetic stimulation for headache pending. There was no specific funding for this study, though Amy A Gelfand was receiving salary support from NIH/NCATS (8KL2TR000143-09) while completing this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.