
Abstract
A search has been made for the neck-tongue syndrome. It started out with a systematic inquiry during the Vågå study of headache epidemiology during the years 1995-97. Two cases were detected relatively early during the study. This led to a scrutiny of such cases also in our hospital headache practice. The origin - and the basis of the study, nevertheless, was the Vågå study. In the Vågå study, where 1838 18-65-year-old parishioners were examined, there were four neck-tongue syndrome cases (N-TS), i.e. a prevalence of approximately 0.22%. N-TS may be more frequent than hitherto surmised. A variant was observed in one case; a young male: instead of numbness, a ‘spasm’ seemed to occur in the tongue. None of the four had at any time consulted their physician for their complaints. In our regular headache practice, two new cases were detected. In one of them and in one of the Vågå cases, there was a combination with ipsilateral cervicogenic headache (CEH). In N-TS, there may be both ipsilateral headache and upper extremity sensory phenomena, a constellation reminiscent of CEH. The possible pathogenetic relationship between N-TS and CEH is therefore discussed in some detail.
Introduction
Occasionally, headache may manifest itself unilaterally and steadily on the same side. Migraine manifests itself in this way in approximately 15% of the cases (1). Unilaterality without side-shift has been stipulated as one of the main characteristics in cervicogenic headache (CEH) (2). Except for in these two types of headache, a domineering unilaterality is a rare phenomenon. Among the actual mini-groups described so far, is also the neck–tongue syndrome (3).
The appellation neck–tongue syndrome (N-TS) implies involvement of the neck. Headache, at least in the occipital area, may be an integral part of N-TS. Headaches with origin in the neck have generally had an ‘irksome birth’, the exception being N-TS. The close temporal association between the neck movement and pain in N-TS, the sudden ‘explosion’, is so impressive that critical attitudes towards the neck as the source may have disappeared like dew for morning sun beams. In principle, CEH has three of the ingredients that N-TS may have: neck pain, unilateral head pain, and mechanical precipitation of attacks.
We have been searching for N-TS as a counterpart of CEH already from its inception in 1980 (3), but without success. We were at the point of giving up this search, when participants in the Vågå study of headache epidemiology started telling us about this sort of pain. In the present communication, some new cases of N-TS are added. These cases stem both from the Vågå study and from our general headache practice. In the exceptional case, N-TS proved to coexist with CEH. Such a coexistence may to some extent throw light upon the nature of CEH. The observations from the Vågå study per se can be used in a prevalence estimation of N-TS.
Materials and methods
A systematic study of N-TS cases was carried out in connection with the Vågå study of headache epidemiology during the years 1995–97. Questions regarding neck pain ± radiation of the pain were routinely asked. The first two cases were detected in this context. These observations led to a scrutiny of new cases in our general headache practise, at the University hospital level. In the course of the next years, several cases were detected during the latter type of practise and in the Vågå study. The basis, nevertheless, was the Vågå study.
There were 3907 inhabitants within the precincts of Vågå at the beginning of the study. All within the age group 18–65 years were invited to participate. Of 2075 available 18–65-year-olds, a total of 1838 (88.6%), were included. The program consisted of a semistructured, face-to-face interview plus a physical and neurological examination, mainly including neck/head (4). Both components of the programme were in the hands of the principal investigator (O.S). In dubious cases, an extensive, clinical neurological examination would be carried out. In some cases, even auxiliary tests, like neuroimaging, would be carried out.
This communication consists of five parts:
Two regular N-TS cases in the Vågå series (cases 1 & 2);
One case of N-TS from the Vågå series, but with ‘lingual spasm’ (case 3);
One case of N-TS combined with CEH and brief, facial discomfort, Vågå series (case 4);
Additional case of regular N-TS combined with CEH, outside the Vågå series (case 5);
Additional case of regular N-TS, outside the Vågå series (case 6).
The N-TS criteria have primarily been those set forth by the IHS (5); but we have been forced to keep an open mind as to symptomatology, since this study primarily took place at the grass-roots level in an unselected population. The diagnosis of CEH was made according to (2).
Case reports
N-TS, regular form (cases 1 & 2)
Case 1
A 39-year-old female had had N-TS attacks since childhood, with rare, rather intense attacks. These were provoked by swift neck movements and only that, mostly (only?) towards the right side. The sharp, stunning right-sided neck pain was shortlasting and lancinated into the right tongue-half, where it was converted to a numbness, lasting less than one minute. The interval between attacks was year-long (Table 1).
Neck–tongue syndrome (N-TS)

‘Pure’ N-TS: cases 1, 2 & 6; N-TS + lingual spasm: case 3; N-TS + CEH: case 5; N-TS + CEH + brief facial discomfort + atypical precipitation mechanisms: case 4. R, right side; L, left side. Min, minutes; s, seconds.
0–5.0+ scale (6). Mean value, headache-free parishioners: 0.42+; mean Vågå material: 0.79+
Skin width, trapezius area, headache-free parishioners: 14.3 ± 5.7 mm;
Visual estimation of skin-fold width.
Case 2
A 46-year-old male had had attacks since approximately the age of 7. Right-sided attacks started after abrupt neck rotation, mostly towards the right side. The brief neck pain spread into the right side of the tongue, where it was transformed to a numbness of short duration. The interval between pain episodes was rather long.
Some further details concerning these two cases, the only ones with an entirely typical picture in the Vågå series, are presented in Table 1. Naturally, not every neck rotation provoked an attack. There was a limited no. of life-time attacks. Remarkably, there was no increase in ‘features indicating cervical abnormality’ (Table 1) (6). Skin-fold thickness values were within control limits and without any asymmetry (Table 1) (7).
N-TS and ‘lingual spasm’ (case 3)
A 20-year-old male draftee had congenital torticollis of the tonic type. In boyhood, the head was slightly rotated towards the left and slightly tilted towards the right. On conservative management, he was more or less symptom-free in adolescence/early manhood.
At 15, during a solitary micturition syncope, he sustained an occipital trauma, hitting the edge of a table, with an ensuing, residual stiffness in the neck for some months. The site of the impact was 2–3 cm to the right of the midline; the scar was 2.5–3 cm long, the lower end being 3–4 cm above the external occipital protuberance. Sensation for touch was reduced in a small area laterally to the scar, the scar itself being indolent. He has been followed-up after 7 years.
The first couple of years after the trauma, he had 4–5 episodes with N-TS. The last 3–4 years, he had another 8–10 attacks. Immediately upon an abrupt neck rotation to the left, rightsided pain would start: simultaneously in the upper nuchal area, in the occipital area, laterally and slightly upwards of the protuberance, and in the tongue. The tongue was immediately ‘drawn’ posteriorly (and to the right?) in one solitary movement. He terms it ‘cramp’ (the same word used in Norwegian). As a footballer, he knows what leg cramps are, and that is what he, spontaneously, compared it to (Table 2). It was the spasm that rendered him speechless. The pain was then substituted by numbness in the entire pain area, this part of the episode lasting 1–2 min. The speechlessness outlasted the numbness: Most of the attacks came during football games (‘soccer’), when trying to hit the ball with the head, the head being in a rotated position. As a captain of his team, he a few times tried to give orders right after the pain/numbness was over, but he was speechless, probably for another 30–60 s. None of the attacks appeared spontaneously. Immediately after an attack, he actually had been able to provoke another attack on turning the head. Nausea, throbbing headache, phono- and photo-phobia were apparently not present during attacks.
‘Elements’ present in the single patient
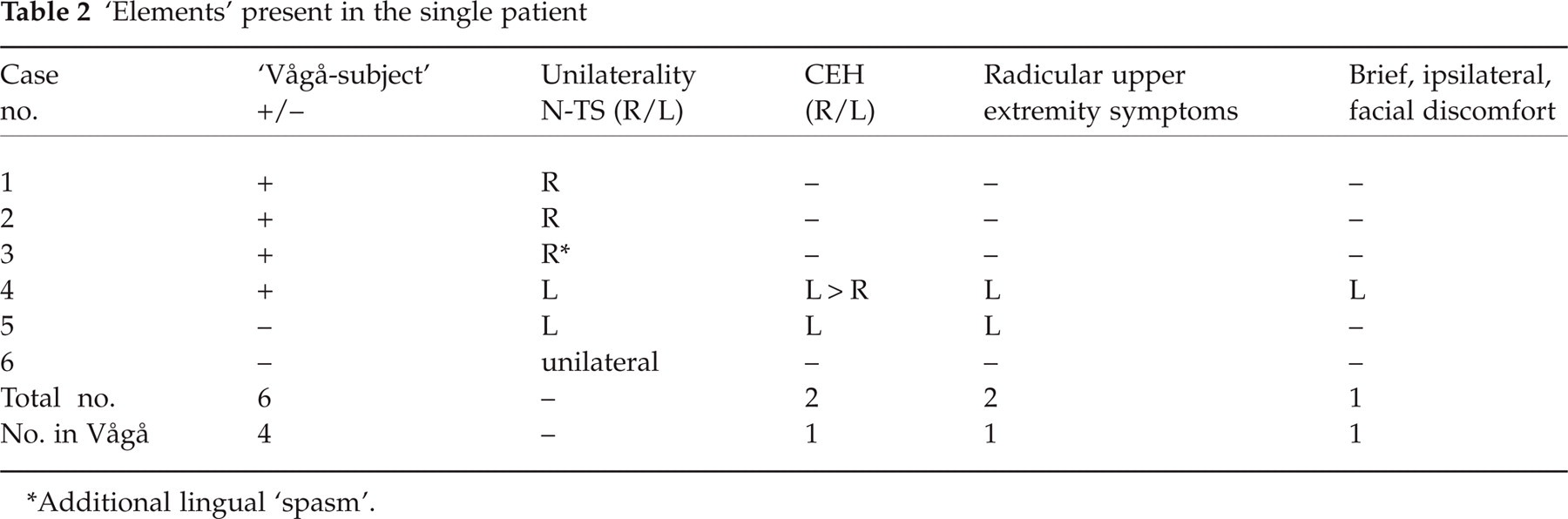
Additional lingual ‘spasm’.
On neurological examination, movement, power, and sensation of the tongue were normal, as was the function of the cranial nerves. Shoulder area skin was 9 mm thick bilaterally (i.e. normal values) and nontender (7). The head was possibly tilted 5° to the right. There was a mild, but definite tenderness in the groove behind the right mastoid process. There was approximately a 25° reduction of neck rotation to the right (controlled more times; normal range of motion to the left). There was slight tenderness in the right sternocleidomastoid (middle part) and upper part of the trapezius muscles. ‘Features indicative of cervical abnormality’: 1.5+ (6), an upper normal value.
N-TS and CEH (case 4)
The case history of this 64-year-old man is detailed because of atypical traits; he has been followed rather closely over the following eight years. He had sustained various, indirect traumas to the neck during childhood. Stiffness in the neck had developed over the last > 10 years. This parishioner had (A) N-TS; (B) cervical radicular phenomena; (C) CEH, with atypical provocation mechanisms; (D) brief, facial discomfort (Tables 1 and 2), all on the left side.
N-TS-like symptoms
From c. 50, leftsided episodes of sharp pain of 1–2 s’ duration appeared in the middle-lower part of the neck (n = 15–20), following quick neck rotation to the left. During a couple, recent episodes, there was a stinging, leftsided, 1–2 s-long sensation in the tongue; it is doubtful whether there was any numbness. The lingual episodes did not occur at a time with facial discomfort (mentioned below), arm symptoms, or CEH. The pain was ‘fairly strong’; there was no spreading towards arm or head of this pain. The neck pain could possibly at times be produced at will, but not the tongue symptoms.
Cervical radicular complaints
Short-lasting, leftsided episodes with paraesthesias into fingers 2/3 appeared, and sensation for touch and temperature on the distal phalanx of finger 3 was subjectively altered for prolonged periods, possibly most noticeable upon thermal stimuli, but not clearly demonstrable upon rough, clinical testing. This hypesthesia was mostly experienced outside a CEH period. In two, a-couple-months-long periods, there were occasional ‘twitches’ in the left triceps muscle. There was never a severe, left-sided radicular pain.
The neurological and supplementary examination findings are most relevant in connection with the cervical radicular phenomena and will be dealt with here. Complete neurological examinations (n = 3) showed no noticeable weakness/sensation loss or myotatic reflex changes. Range of motion in the neck was gravely diminished; rotation: towards the right: 25° deficit; towards the left: approximately 30° deficit; extension: 60° deficit. Considerable tenderness was present in the groove behind the mastoid process, with a clear left-sided preponderance: 1.5+ pain at 6–8 kg pressure: persisting frontal area pain (6). Skin-roll test showed normal values (7); features indicating cervical abnormality: 3.0+, i.e. a clearly pathological value (range 0–5.0+ (6)) (Table 1). MRI of the brain: negative findings. Cervical spine MRI showed massive degenerative disk changes, most marked at the C5-6 and C6-7 levels, without infringement upon the cord. X-ray examination of the cervical spine corroborated these findings. MRI was taken to exclude a serious disorder. In that respect, the long-lasting case history also was reassuring.
CEH
This was experienced from the age of 60 in two periods, each of 2–4 months duration, and approximately one year apart. Long-lasting (weeks) exposure with neck flexion seemingly could provoke a long-lasting symptomatic period. The CEH pain appeared only after weeks of exposure. The constant, fluctuating, but mostly low-grade, upper nuchal pain could spread to the fronto-temporal area as mild/moderate pain (3–4+ on a 0–6+ scale (8)). The pain was in essence bilateral, but periodically predominantly leftsided. There could be unwellness and dizziness, but no nausea. In the worst periods, a brief, but rather intense pain increment would follow immediately upon stooping, but also upon assuming the erect position too quickly after stooping. Removing an object from the floor, with the upper part of the body and the neck kept in an erect position, could pass without additional symptoms. Coughing could increase the head pain in such periods, but not to the extent that stooping did. There was recently a near-fainting episode upon prolonged extension of the neck, outside the CEH periods.
Brief, facial discomfort
For the last 7–8 years, there has been an episodic, leftsided, facial discomfort, the frequency highly varying, from several per hour to one per several months (Table 2). The ‘epicentre’ was steadily located preaurally; the affected area was approximately 3 cm in diameter. There was no spreading and no tinnitus, and it was entirely unrelated to chewing. An episode lasted about ½-1 minute, with abrupt beginning and end. The discomfort was ‘indescribable’; similar to, but apparently different from ‘itching’ and ‘pins and needles’ (without the sharp quality); the discomfort was described as slightly fluctuating, but not pulsating. There was no particular tenderness over the TMJ. Sensation was normal in this area.
Temporally, the ‘facial discomfort’ seemed to be totally dissociated from CEH, as well as from the radicular phenomena, but the ipsilaterality of these phenomena is intriguing. A certain precipitation mechanism seemed to be predominant, as regards the protracted CEH exacerbations: bending forward for prolonged periods – days/weeks. This precipitation mechanism leading to protracted exacerbations has, as far as we are concerned, not been properly described before in CEH.
A resurgent interest in N-TS in the wake of the Vågå study led to the detection of two more cases (Table 1).
N-TS and CEH; not belonging to the Vågå study (case 5)
A 40-year-old housewife had had a considerable number of a-few-seconds-long N-TS attacks from around 10, with left-sided neck pain and tongue numbness, precipitated by neck rotation. Neck movement always (?) antedated the pain paroxysms. She had sustained a direct neck trauma at approximately 14, i.e. after the onset of N-TS. This patient had since the age of 37 had leftsided CEH, with chronic-fluctuating pain in the neck/back of the head and with exacerbations from a few times per week up to daily. The pain spreads to the ocular/temporal area (Table 2), but also to the left shoulder and distal arm. Paresthesias and numbness were noted in the four ulnar fingers. These complaints could hinder sleep. There was slightly reduced movement in the left shoulder joint, but an X-ray study of the shoulder was negative. A GON-blockade on the left side took away much, but not all of the pain. CEH was the reason for consultation, not the N-TS.
Clinical neurological examinations (n = 3) showed a questionable sensory deficit in the ulnar side of the left upper extremity and in the two ulnar fingers and a possible reduction of the left triceps reflex. The groove behind the left mastoid process was clearly tender, the pain on palpation spreading onto the vertex and retroorbitally. Rotation to the left was reduced by approximately 25° and extension even more. Cervical spine MRI showed degenerative changes at the C6-7 level, with clear encroachment upon the left 7 root canal and with suspicion of affection of the root. ‘Features indicating cervical abnormality’ were increased (Table 1). The N-TS seemed to have started prior to the neck trauma at 14. It might be more than a chance association that both the N-TS, the probable radiculopathy, and the CEH were on the same side.
N-TS, not belonging to Vågå series (case 6)
This patient, whose file we could not retrieve, was a male agricultural worker, approximately 30 years old at the onset. He had a 2–3-year-long history of typical unilateral, moderate/severe neck pain upon neck movements and a subsequent, ipsilateral, short-lasting tongue pain. The total number of attacks was ‘considerable’, N-TS being the reason for consultation. Neurological examination (n = 1) was negative.
Discussion
Prevalence
N-TS has been supposed to be a rare syndrome (9). A report from 2003 (10) gives the total number as 32 + 8 new cases: = 40. The fact that also other, rather large series have been reported: n = 6 (11); and n = 7 (?) (3, 12); and the present report: n = 6, indicates that N-TS occurs more frequently than hitherto surmised.
While previous reports seem to be based on patient consultations, the present communication is mainly based on epidemiological data: 4 parishioners in Vågå seemed to suffer from N-TS, corresponding to a prevalence of 0.22% (Table 2). In an epidemiological study of this nature, a more mild version (‘N-TS light’) of the syndrome could conceivably surface. None of the four had consulted their physician due to these complaints. The frequency of attacks seemed to be relatively low, i.e. approximately one attack per year. It is hard to extract a comparable figure from relevant literature.
On the clinical manifestations of N-TS
‘Nuchal jabs’ (13) and N-TS have similar characteristics. The original picture of N-TS was: a sharp, unilateral neck pain upon neck rotation and ensuing ipsilateral numbness in the tongue (3, 14). There are apparently variants of this picture. Thus, Hankey (15) states: ‘upper nuchal pain radiating to the ipsilateral side of the tongue …; … followed by residual numbness … ipsilateral side of the tongue …’. There may, according to these descriptions, be a numbness of the tongue, with or without a foregoing tongue pain (3, 9, 15). And ‘residual numbness over the posterolateral aspect of the upper neck – for 3–5 minutes’ (15). Neck pain apparently might (3, 15, 16) or might not (3, 9) be followed by neck numbness.
Neck and tongue symptoms frequently – but apparently not always (17) – follow ipsilateral rotation in the neck. Although neck and tongue symptoms remain ipsilateral, the rotation may be to either side (3, 9, 18). However, the picture may become even more complex: the whole constellation of symptoms could change to the opposite side, inclusive of the precipitation mechanism (15).
Another variation is even more conspicuous: In for example Lance & Anthony (3) case II, only ‘on the last occasion’ (out of 6–7 attacks, over three years) had there been numbness of the tongue. In other words, for prolonged periods, it was not known that this patient would develop the additional and the most characteristic manifestation of N-TS: the tongue symptoms. There is, nevertheless, every reason to believe that the same disorder had been present since the beginning, but in an incomplete form and not fully expressed. Conceivably, the ‘complete picture’ will not – in a given case – have surfaced at the time of consultation; in some such cases, it may never (?) surface (11). The diagnosis may be established with certainty only in those who later develop ‘the full syndrome’. Also in our case 4, it was only after a long period with attacks of stinging neck pain that tongue pains appeared. The chances that in such a case, tongue symptoms eventually will develop, must be assumed to be many times larger than the chances that a given, nonaffected individual eventually will develop N-TS.
If only the unilateral neck pain is present, and not the lingual symptoms, the differential diagnosis vs. nuchal jabs (13) may be difficult. There may be several differential diagnostic hints: When severe, the pain of N-TS might radiate (3, 19), and there may be tingling in the arm (17) and even occipital headache(see below). The latter symptoms, if present, clearly distinguish N-TS from nuchal jabs, which altogether seems to be a symptom-poor pain disorder (Table 3).
Some clinical characteristics of N-TS and nuchal jabs (13)

To ipsilateral occiput/head and/or upper extremity.
Headache as an integral part of N-TS
Headache may be part of the solitary N-TS attack: ‘When severe, the pain radiated to the back of her head …’ (19). ‘… ‘pressure’ sensation in the occiput …’ (case I) and ‘… ipsilateral …’–‘sharp occipital pain’–‘shooting’ to the periorbital area.’ (case II) (17). In Lance and Anthony's case II (3), the following happened: ‘… a sharp pain in the right [= symptomatic side] occipital region, shooting upwards ‘like a line up the back of the head’ …’. And in case III: ‘… tearing pain’ … ‘which radiated over the left occipital region, followed immediately by a tingling burning feeling over this area’. Case I: ‘… pain appeared to be deep to the angle of the jaw on the left [= symptomatic side], radiating to the occiput …’ (20). Occipital pain – in the absence of any neck pain – has also been observed: thus, in Lance & Anthony's case II (3).
The pain/sensation into the head generally appeared concomitantly with the neck/tongue phenomena, similarly to what was observed in our case 3, and generally (invariably?) on the symptomatic side. Headache in the mentioned cases was an integral part of the single N-TS attack; in our two other cases of N-TS and ipsilateral headache (cases 4 & 5), the two disorders appeared asynchronously, the headache, furthermore, being long-lasting and assuming CEH characteristics. Admittedly, the head pain in N-TS was mainly occipital (with the exception of (17)), while the CEH part in the combined N-TS/CEH picture also was ‘anterior’.
Ipsilateral upper extremity phenomena in N-TS
Even ipsilateral arm discomfort/sensory disturbances, typical traits in CEH, may be part of N-TS. According to Lance and Anthony (3): ‘Simultaneously – numbness of the right side of the tongue … and of the right little and ring fingers, which lasted for a few seconds only’ (case I). And in another case: ‘when severe, the pain radiated … into the right [= symptomatic side] arm’ (19). ‘These complaints (i.e. ‘sharp’‘aching’ pain, radiating along the border of the trapezius to the acromioclavicular joint) had been occurring concomitantly with … and ‘pins and needles’ paresthesias of the 4th and 5th digits of her right [= symptomatic side] hand’ (case I (17)). And: ‘… paresthesias in the ulnar distribution of the upper extremities. These would usually be solely on the right side, occasionally on the left, but never both sides concomitantly’ (case II) (17). At this stage, it remains uncertain what significance to attach to the mainly ulnar distribution of the finger symptoms in N-TS. In CEH, sensory phenomena may be diffuse/vague – or radicular. The atypical tongue phenomena in our case 3 were like a spasm with movement in one direction only, similar to what has been described by Lance (12).
N-TS and CEH – similarities and differences
There seems to be more or less consensus that N-TS originates in the neck, e.g. N-TS presents ‘… with a referred pain syndrome that is clearly cervicogenic as evidenced by the prompt precipitation of the symptoms by neck movement’ (17). The fact that some patients, immediately upon an attack, voluntarily can precipitate an episode by neck movements (but not otherwise) also attests to the fundamental role of the neck in N-TS (15, our case 3).
The ultimate implications of these observations may seem to be:
Pain conditions with a symptomatology like – but not necessarily identical to – that of N-TS also may arise in the neck.
Such symptomatology, and not only that of N-TS, may be provoked by certain mechanical precipitation mechanisms, with an impact on the neck.
In N-TS, there is nonobligatory radiation of pain towards shoulder/arm and occipital area and occasionally even the eye, as already mentioned. A characteristic feature of N-TS attacks is that, generally, the whole panorama of symptoms – when present – appears immediately upon a quick exposure and in concert. Due to this association in time, it is highly likely that, in N-TS, all the symptoms, including the headache, not only are generated from the neck, but by the same/similar mechanism. There is little reason to postulate an accessory mechanism for the head/arm pain.
In this respect, N-TS is clearly different from combination CEH/N-TS, where the various features appear asynchronously. Mechanical precipitation of attacks is probably a hallmark of CEH (2). In CEH, the adequate stimuli seem to be relatively long-lasting ones, e.g. untoward positioning of the neck during sleep, when protective mechanisms (against untoward positioning of the neck) are not operative. In N-TS, a short-lasting, and not a long-lasting, stimulus is the adequate one. Short-lasting exposures, such as coughing and straining at stool, do usually not suffice for generating attacks in CEH (exceptional case: no. 4, present communication). Due to the long-lasting provocation in CEH – any combination with an ensuing headache may represent a challenge to the observer. The temporal differences between N-TS and CEH are thus appreciable: 1. the duration of the stimulus; 2. the interval between stimulus and the result; and 3. the duration of the pain.
In N-TS cases without associated CEH (1, 2), there were normal ‘features indicative of cervical abnormality’ (mean: 0.25+Table 1), whereas in the cases combined with CEH, there were markedly increased values: no. 4 (3.0+) and no. 5 (3.5–4.0+). Also in the one with torticollis and lingual spasm, there was a relatively high value: 1.5+ (Table 1). The mean value in the general population was: 0.79+ (6). A value > 2.5+ was present in only 2.3% of the cases in Vågå (6).
There may seem to be various variants in the N-TS/CEH interrelationship (Table 4). ‘Features indicative of cervical abnormality’ (I) thus seem to be present to a much higher extent in the CEH + N-TS combination than in ‘pure’ cases of N-TS. Other marked differences count in the direction of a dichotomy between CEH and N-TS: (II) tongue symptoms are not present in CEH. (III) Headache is – by definition – invariably present in CEH.
The various combinations of N-TS with other pain syndromes/phenomena

This leads to another rather thought-provoking notion: In N-TS cases where tongue symptoms in the initial phase have been lacking, but where headache was present(e.g. case II (3)), two of the main counter-arguments, i.e. II & III(see above) against a unitarian concept for these headaches may seem to be lacking. The two headaches become rather similar from a clinical/phenomenological point of view. Point I may have to do with localization and degree of involvement in the two disorders and may not necessarily be a ‘splitting factor’. By analogy, due to this genuine similarity between N-TS and CEH in such cases, it can probably be inferred that the cervical area is likely to be stigmatized also in CEH: attacks of CEH originate in the neck, just like those of N-TS.
In spite of spectacular similarities between N-TS and CEH, the different precipitation mechanisms and temporal perspectives indicate that we are faced with fundamental discrepancies; fundamental differences of this order of magnitude indicate that we probably have to do with two different disorders, both with an origin in the neck.
In our cases with a combination of N-TS and CEH (cases 4 & 5; Table 2), an essential matter may appear to be that CEH was ipsilateral to the N-TS symptoms. That a rare symptom complex like N-TS is located on the same side as CEH, is hardly likely to be due to mere coincidence, although this possibility cannot be entirely excluded.
Headache and other symptoms in connection with N-TS attacks have not been particularly focussed on in previous reviews on N-TS.
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway, Pharmacia & Upjohn, and the Alf Harborg Foundation, Department of Neurology, St. Olavs. Hospital, Trondheim, Trondheim University Hospitals, for generous support during the various phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.