
Abstract
Background
Sensitization and impaired habituation of cortical neurons have been reported in migraineurs. Repetitive transcranial magnetic stimulation (rTMS) may change these phenomena and be the basis of therapeutic response. We report the effect of 10 Hz rTMS on sensitization and habituation of median somatosensory evoked potential (SEP) in migraineurs, and correlate these changes with clinical response.
Methods
Migraineurs having four or more episodes of headache per month were included and their clinical details were noted. Three sessions of 10 Hz rTMS, 600 pulses in 412.4 seconds were delivered on the left frontal cortex corresponding to the hot spot of right abductor digiti minimi, on alternate days. Median SEP was done before and 30 minutes after the third rTMS session. Sensitization (block I N20 amplitude) and impaired habituation (if N20 amplitude of block 2 or 3 were not suppressed compared to block I) were noted. The reduction in frequency and severity of headache in the next month were noted and correlated with SEP changes.
Results
Ninety-four migraineurs were included; 56 received true rTMS and 38 sham stimulation. Following stimulation, reduction in N20 amplitude of block 1 correlated with a reduction in frequency and severity of headache at one month. The impaired habituation significantly improved in the true rTMS group compared to sham stimulation, and correlated with a reduction in the severity of headache but not with frequency.
Conclusion
In migraineurs, 10 Hz rTMS improves habituation and may be the biological basis of headache relief.
Introduction
Headache is a common health problem, and affects more people than asthma and diabetes (1,2). Migraine is the commonest cause of headache, and about 12% of the general population suffers from migraine (3). The underlying pathophysiology of migraine is complex, and probably interplays between genetic, biochemical and environmental factors. Evoked potentials have been used to evaluate cortical neuronal excitability and inhibition. Abnormal cortical excitability, impaired habituation and potentiation have been reported on contingent negative variation (CNV), visual, auditory and somatosensory evoked potentials (5–9). In migraineurs, two main evoked potential findings have been reported, cortical disexcitability and deficient habituation. In some studies, reduced P100 amplitude of pattern-reversal visual evoked potential (PR-VEP) has been reported in between headache attacks, and higher amplitude during or in close proximity of a headache to others (9–12). We have reported impaired habituation in 71% of patients with migraine using median somatosensory evoked potential (SEP), and this phenomenon was observed in all the subtypes of migraine, i.e. episodic migraine, chronic migraine and medication overuse headache. Patients with allodynia had evidence of sensitization on median SEP (13). Manipulating these two basic neurophysiological characteristics of abnormal excitability and impaired habituation in migraineurs may help in aborting or reducing the headache attack. A single pulse of transcranial magnetic stimulation (TMS) has been reported to relieve pain at 2 hours in 81% patients in an open labeled study, and 39% to 69% in randomized control trials (14,15). High rate repetitive TMS (rTMS) at 10 Hz, 600 pulses delivered to the hotspot of the right abductor digit minimi for three days was effective in reducing the severity of pain in 78.7% and frequency in 76.6% of patients (16). The basis of clinical response following rTMS has been evaluated in only a few studies (17,18). In one study, the level of β endorphin was increased following 10 Hz rTMS and was associated with clinical improvement (19). In another study, long lasting habituation of VEP in migraineurs has been reported after high rate rTMS over the occipital area (20). In the available medical literature, there is only one study evaluating the effect of high rate rTMS on sensitization and impaired habituation using median SEP (21). This study, however, did not correlate these phenomena with reduction in headache frequency and severity. In this study, we therefore report the effect of high rate rTMS on sensitization and impaired habituation of median SEP in migraineurs, and compare these changes with migraineurs receiving sham stimulation. We also correlate the SEP changes following rTMS with reduction in headache frequency and severity at one month.
Subjects and methods
Patients with migraine who were having more than four headache attacks per month were included from the neurology out patient service of a tertiary care teaching institute. The diagnosis of migraine and medication overuse headache was based on the International Classification of Headache Disorder (22). The study was approved by Institute Ethics Committee (PGI/BE/256/2011). This is a sub analysis of our earlier study, in which we reported high rate rTMS as a migraine prophylaxis (16).
Exclusion criteria
Migraineurs with seizure, mental retardation, neurological deficit, structural brain abnormality on CT/MRI, pregnancy, major psychiatric or metabolic disorders and those on antipsychotic, antiepileptic or migraine prophylactic drugs were excluded. The patients who did not consent for the study were also excluded.
Evaluation of SEP
The demographic (age, gender, residence and education) details of the patients were noted. The duration of illness was noted. The frequency of headache per month, severity, associated symptoms and functional disability were recorded. The severity of headache was measured on a 0–3 scale (0 = none, 1 = mild, 2 = moderate, 3 = severe), and functional disability on a 0–4 scale. The patients were asked about allodynia using a questionnaire (23). The patients were advised to maintain a headache diary including frequency, severity and functional disability. The need for an abortive drug and its response were also noted. The migraine prophylactic drugs were stopped 15 days prior to the study. On the day of study, the patients were advised to avoid taking abortive medication [non-steroid anti-inflammatory drugs (NSAIDs), triptans or opioids] if possible till the SEP study was completed to avoid the effect of drugs on SEP. Presence of headache on the first and last day of SEP was noted.
Median SEP
Right median SEP was done before the first and 30 minutes after the third session of rTMS. The patients were asked to relax on a couch in a supine position. The median nerve was stimulated at the wrist at 1 Hz by 0.5 ms square wave pulse with a current strength in which there is a perceptible painless twist of the thumb. The band pass was 2–3000 Hz, and analysis time was 100 ms. The recording electrode was placed 2 cm posterior to C3 referred to Fz in a 10–20 system of EEG (electroencephalography) electrode placement. Three consecutive blocks of 100 epochs were averaged, and peak to trough of N20 amplitudes were measured. The amplitude of N20 in block I was considered for sensitization. Impaired habituation was defined if the amplitudes of N20 in block 2 or 3 were not reduced compared to block 1. Augmentation was considered if the N20 amplitude of block 2 or 3 was increased compared to block I (13).
High rate rTMS
Repetitive transcranial magnetic stimulation was performed using a magnetic stimulator, Magstim Rapid Whiteland, Wales, UK. A figure of eight air cooled coil of 7 cm diameter was used, and sham stimulation was performed using an identical-looking sham coil. We followed the stimulation protocol of Brighina et al with some modification (24,25). The stimulator was placed over the left frontal region, which corresponds to the hot spot of abductor digiti minimi. This corresponds to the scalp, which is 7 cm lateral and 2 cm anterior of the line joining Cz to tragus. The motor threshold was measured, and 70% of this was used for rTMS. Each session of 10 Hz rTMS comprised 600 pulses in 10 trains in 412.4 seconds. Three sessions of rTMS were delivered on alternate days. Sham stimulation was delivered in a similar manner using an identical looking sham coil. It produced a similar sound, but did not produce muscle contraction. The motor threshold, however, was not measured for sham stimulation to avoid the effect of true stimulation (16).
Follow up
The frequency and severity of headache in the subsequent four weeks were noted and outcome was defined at one month. The patients were considered improved if there was >50% reduction in frequency and severity. The overall improvement in frequency and severity was evaluated using a 0–100 Visual Analogue Scale (VAS) scale.
Statistical analysis
The baseline clinical and SEP characteristics were compared using the Fisher exact test for categorical and the independent t test or Man-Whiney U test for continuous variables. The change in sensitization was compared within the group by paired t test, and between the groups by independent t test. The change in N20 amplitudes in Block 2 and 3 compared to block 1 was compared by one-way analysis of variance (ANOVA) using Tukey post hoc correction. The number of patients with impaired habituation before and after sham and true rTMS was compared using the Chi square test. The change in SEP parameters between responders and non-responders were compared using various parametric and non-parametric tests. The variable was considered significant if the two-tailed p value was <0.05. The statistical analysis was done using SPSS 16 version and graphs were prepared by GraphPad Prism 5.
Results
Comparison of the clinical characteristics of migraine patients who received true and sham repetitive magnetic stimulation (rTMS).

SEP = somatosensory evoked potential.
Median SEP
Fifty-six patients received true rTMS and 38 received sham rTMS. The baseline N20 amplitudes of blocks 1, 2 and 3 in the true rTMS and sham stimulation groups were not different (Table 1). About 73% patients in both the groups had impaired habituation.
Effect of rTMS
In the true rTMS group, the sensitization (N20 amplitude of block I), although reduced compared to the pre rTMS value, did not achieve statistical significance (8.03 ± 3.98 µv vs. 7.74 ± 4.45 µv; p = 0.38). The impaired habituation improved after the true rTMS, whereas it was more marked following sham stimulation (Figure 1). On comparing SEP parameters between the true and sham rTMS after the third session, there was no difference in reduction in sensitization (7.74 ± 4.45 vs. 7.69 ± 3.45 µv; p = 0.95). However, the difference of N20 amplitude in blocks 1–2 (p = 0.02) and 1–3 (p = 0.05) revealed greater suppression in the true rTMS group compared to the sham stimulation group (Figure 1).
Error line diagram shows effect of true and sham repetitive transcranial magnetic stimulation (rTMS) on habituation of N20 potential of median somatosensory evoked potential. The impaired habituation improved following true 10 Hz rTMS (a), but did not improve following sham stimulation (b). The baseline impaired habituation of N20 potential, although not different between rTMS and sham stimulation groups (c), improved significantly following true rTMS compared to sham stimulation (d).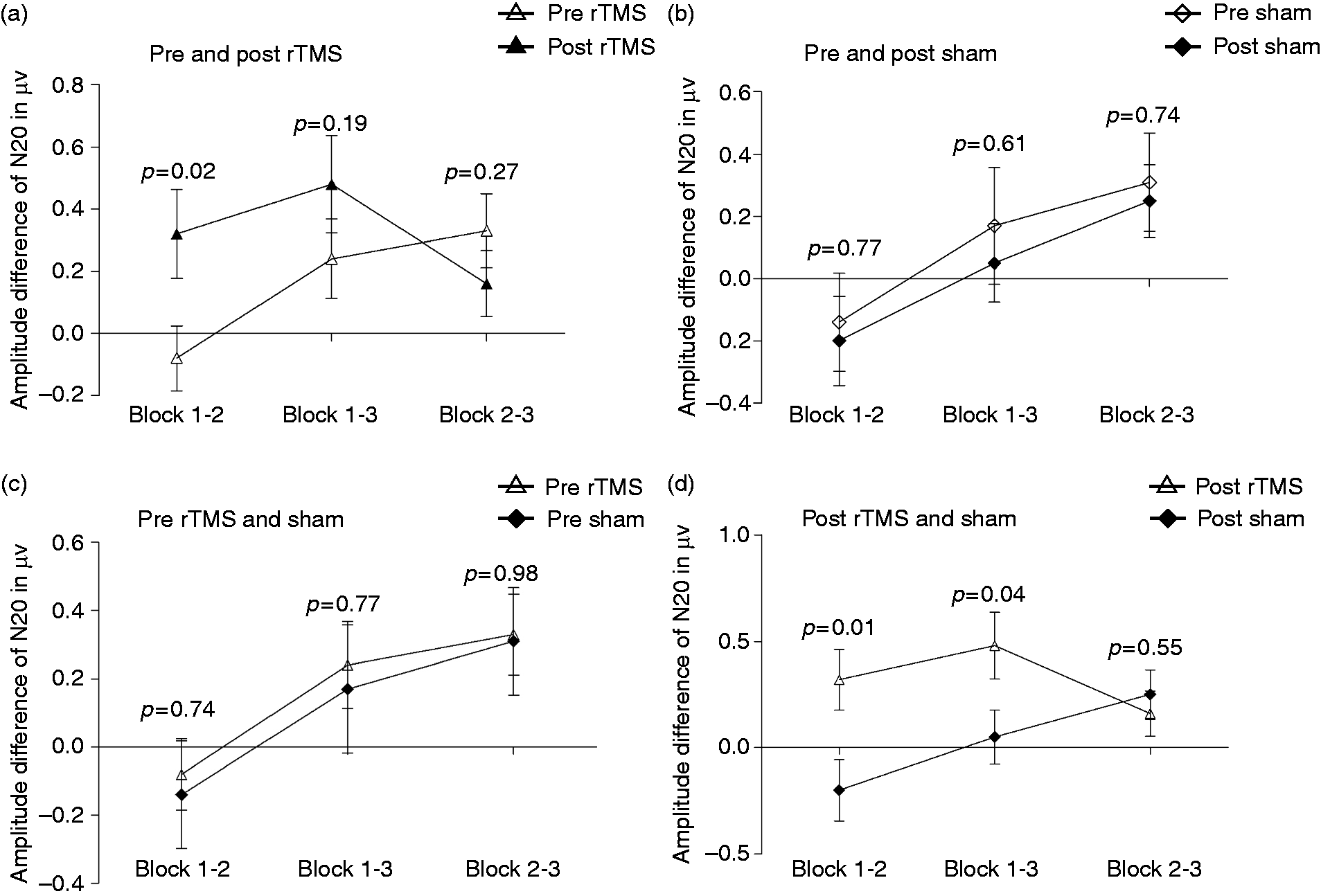
In the true rTMS group, the impaired habituation decreased from 41 (73.2%) patients to 31 (55.4%; p = 0.07) and in the sham stimulation group from 28 (73.7%) to 26 (68.4%; p = 0.84). The details are shown in Figure 2.
Number of migraine patients with habituation and impaired habituation before and after true repetitive transcranial magnetic stimulation (rTMS) and sham stimulation.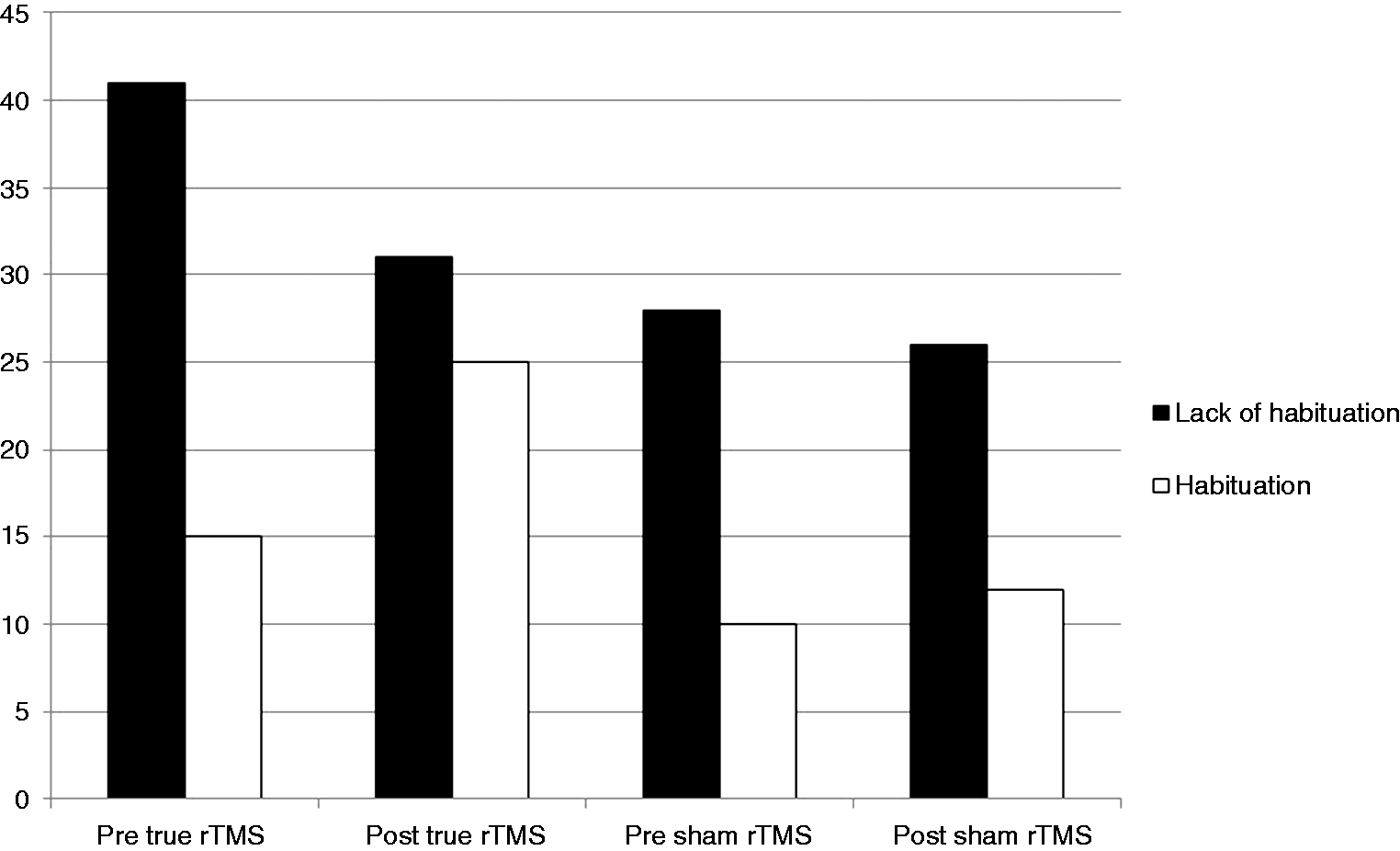
Correlation with clinical response
The baseline block 1 amplitude correlated with frequency and severity of headache. During the first SEP study, 70 (74.5%) patients had headache, and the block 1 N20 amplitude was insignificantly higher in them compared to those without headache (8.51 ± 4.43 vs. 7.13 ± 2.81 µv; p = 0.24). During the second SEP study, 37 (39.4%) patients had headache and their block 1 N20 amplitude was also insignificantly higher than those without headache (8.59 ± 3.73 vs. 7.87 ± 4.35 µv; p = 0.13). At one month, 44/56 (78.6%) in true rTMS and 13/38 (34.2%; p < 0.0001) patients in the sham stimulation group had improved by more than 50% in VAS score. The average severity of headache also declined significantly in the rTMS group compared to the sham group. The reduction in headache frequency at one month correlated with a reduction in sensitization in the true rTMS group (r = 0.32; p = 0.02), but not in the sham group (r = 0.12; p = 0.48). The reduction in headache severity also correlated with a reduction in sensitization (r = 0.25; p = 0.02) and the extent of habituation in block 2 (r = 0.21; p = 0.04). However, this effect was similar in both true and sham stimulation groups. The correlation of relevant variables is shown in Figure 3.
(a) Regression curves show correlation of the reduction in sensitization (N20 amplitude of block I before and on fifth day after stimulation) on median somatosensory evoked potential with frequency and severity of headache attack at one month. (b) Regression curves show correlation of severity of headache [Visual Analogue Score (VAS) and severity score on a 0–3 scale)] with improvement in habituation in repeat median somatosensory evoked potential on fifth day after stimulation.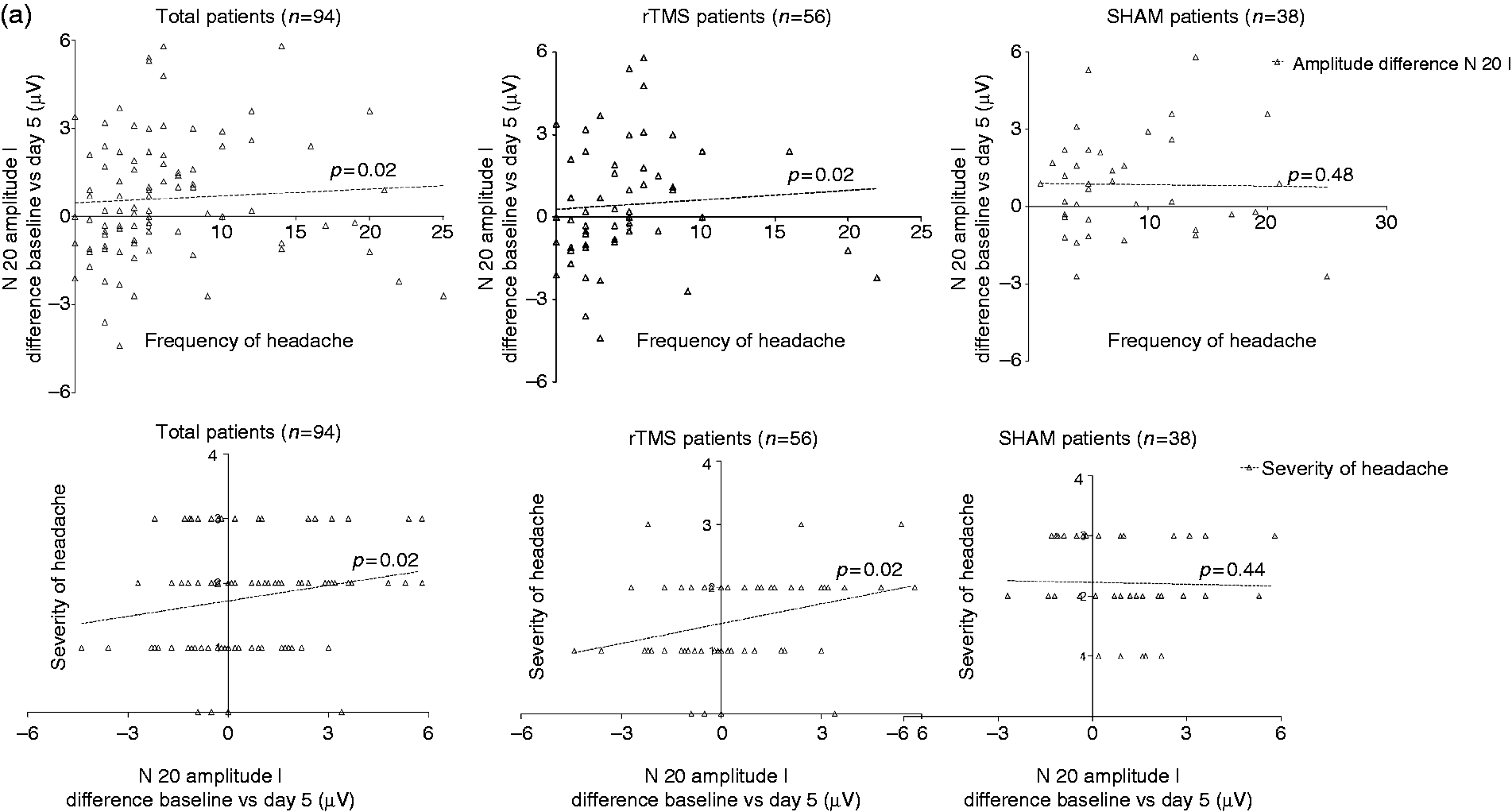
Discussion
In this study, 10 Hz rTMS resulted in significant suppression of N20 amplitude of block 2 and 3 compared to sham stimulation, suggesting improvement in habituation. Sensitization, although reduced following rTMS, did not achieve significance compared to sham stimulation. The improvement in habituation correlated with reduction in headache severity, and reduction in sensitization correlated with frequency and severity of headache at one month. This study evaluated the effect of high rate rTMS on sensitization and impaired habituation using median SEP in migraineurs, and correlated these phenomena with improvement in headache frequency and severity for the first time. In a recent study, the effect of rTMS on median SEP has been evaluated in 13 migraineurs and 13 healthy controls. In migraineurs, one Hz rTMS reduced the block 1 N20 amplitude and habituation, whereas 10 Hz rTMS increased the block 1 N20 amplitude and induced habituation. Evaluation of high frequency oscillations (HFO) revealed an increase in late HFO following 10 Hz rTMS in both patients and controls, but early HFO was increased only in the patients compared to pre-stimulation level (21). The early HFO is attributed to thalamocortical cholinergic projection, and late HFO to cortical GABAergic interneurons. SEP study in migraineurs revealed smaller baseline amplitude, and a smaller area under curve (AUC) of early HFO burst during the interictal period compared to the controls, but there was no difference in late HFO. During headache, the amplitude and early HFO were comparable to the controls. Based on HFO on SEP, the authors have suggested dysfunction of the thalamocortical loop for the genesis of impaired habituation in migraine (26). In a study on 55 migraineurs, there was significant potentiation of N20 potentials in the subsequent blocks of median SEP, whereas there was suppression of N13 and N20 potentials in the healthy individuals (27). Another study on episodic migraine has reported sensitization and habituation during the ictal period, and no sensitization and impaired habituation during the interictal period. However, the patients with medication overuse headache had both sensitization and impaired habituation (28). In our earlier report, migraineurs had sensitization and impaired habituation of N20 potential of median SEP compared to the controls, which were more marked during headache. Impaired habituation was observed in all the subtypes of migraine; 76.1% in episodic migraine, 73.9% in chronic migraine and 61.3% in medication overuse headache. Sensitization was highest in chronic migraine followed by episodic migraine and medication overuse headache, and correlated with allodynia (13). Sensitization and impaired habituation may be dependent on the innate and adaptive behavior of neurons. Moreover, habituation may be a dynamic process depending on the state of the neurons. The extent of habituation may vary in the same individual at different times. We have therefore repeated the SEP study in both of the groups.
There are only a few studies evaluating the effect of rTMS on VEP in migraineurs. In one study, VEP during the interictal period did not reveal impaired habituation (29). Later, the same group reported reduction of habituation, but not the sensitization of VEP following 10 Hz rTMS, 900 pulses (30). In healthy volunteers, 1 Hz rTMS over the occipital cortex resulted in an increase in block I VEP amplitude, and impaired habituation in subsequent blocks. 10 Hz rTMS had no effect on healthy volunteers. In migraineurs, 1 Hz rTMS had no effect on habituation, but 10 Hz rTMS increased block 1 amplitude and normalized habituation. This effect lasted for 9–30 minutes (31). This study, however, did not correlate the VEP changes with clinical migraine response. Daily rTMS for five days in migraine patients resulted in VEP changes from hours to seven days in another study (20). We have performed SEP within 30 minutes of a third session of rTMS to evaluate the maximum effect following stimulation. The degree of suppression in block 2 following rTMS was significantly higher compared to the pre rTMS level, and correlated with improvement in headache severity at one month. The change in sensitization of SEP following rTMS also correlated with reduction in frequency and severity of headache at one month. The lack of significant changes in SEP parameters following sham stimulation, and significant correlation of SEP changes with clinical improvement in true rTMS, suggest the role of rTMS in modulating neuronal behavior. The neurobiology of cortical neurons has been evaluated with the help of TMS. Low rate (<5 Hz) rTMS inhibits the underlying cortex, and high rate rTMS (>5 Hz) most often activates it (9,32). The regional blood flow (rCBF) is also reduced following low rate rTMS, and increased following high rate rTMS (33). The motor cortex has a strong modulatory effect on the sensory cortex and vice versa. Stimulation of the M1 cortex in mammals suppresses the neuronal response to touch by 40% in the ventro-posterolateral nucleus of thalamus (34), and by 10% in brainstem nuclei (35,36). In humans, rTMS over the motor cortex results in neurotransmitter release in the subcortical structure, and activation of the cortico-subcortico-cortical loop induces EEG oscillations (37,38). Inhibition of thalamic sensory relay neurons following motor cortex stimulation has been attributed to pain relief in central pain (39). 10 Hz rTMS over the motor cortex in migraineurs has resulted in an increase in plasma β endorphin level, which correlated with improvement in headache frequency and severity. The responders had higher changes in β endorphin from pre rTMS level compared to those who did not respond (25). High rate rTMS also results in excitation of GABAergic neurons, which may be responsible for improvement in habituation of SEP. The reduction in sensitization following rTMS in our study may be due to activation of the thalamocortical and brainstem aminergic pathway, which set the neuronal excitability level.
The present study is limited by its non-randomized design, inclusion of chronic migraine with medication overuse and lack of SEP at one month follow-up. We did not have control healthy volunteers for rTMS for ethical reasons.
The present study highlights the improvement in habituation of SEP following high rate rTMS. The change in habituation and sensitization correlated with clinical response. Further study is needed to evaluate the effect of extended sessions of high rate rTMS in non-responders as well as the requirement for subsequent stimulation in responders.
Clinical implications
In migraineurs, high rate rTMS improves habituation of median SEP. The reduction in headache frequency at one month correlates with reduction in sensitization following rTMS. Following rTMS, the reduction in headache severity at one month correlates with both improvement in sensitization and habituation of median SEP. High rate rTMS may reduce headache by modulating the neuronal behaviour.
Footnotes
Acknowledgement
We thank Mr. Rakesh Kumar Nigam and Mr. Shakti Kumar for secretarial help.
Ethical approval
The study was approved by Institute Ethics Committee (PGI/BE/256/2011).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.