
Abstract
Introduction
We report a case of cervicogenic headache caused by an intradural extramedullary tumor of the middle cervical spine, which has not previously been reported.
Case presentation
The patient was a 73-year-old male who visited a physician for a chief complaint of pain from the left lower jaw to the auricle and occipital region. The headache was induced with retroflexion of the neck. On cervical magnetic resonance imaging, an intradural extramedullary tumor was noted on the left side at the C4/5 level. The intradural tumor, which arose from the C5 nerve root, was excised and the pain was resolved. The pathological diagnosis was schwannoma.
Conclusion
Previously reported cases of spinal cord tumor-induced cervicogenic headache were due to upper cervical spinal tumors. This is the first report that a middle-lower cervical intradural extramedullary tumor caused cervicogenic headache.
Introduction
Headache caused by cervical spinal diseases is known as cervicogenic headache, but few cases accompanying spinal cord tumors have been reported. Previously reported cases were caused by upper cervical spinal cord tumors. We encountered a patient with cervicogenic headache induced by a cervical intradural extramedullary tumor which arose from the 5th cervical nerve root. This is the first reported case of cervicogenic headache induced by a middle-lower cervical intradural extramedullary tumor.
Case presentation
The patient was a 73-year-old Asian male who had retired. His chief complaint was pain from the left lower jaw to the auricle and occipital region; he had a past medical history of hypertension and hyperlipidemia, but had no experience of admission or surgery. The patient became aware of pain from the left lower jaw to the auricle and occipital region 3 months before visiting our hospital. He visited an otolaryngologist and was referred to the neurology department of our hospital. No abnormality was noted on neurological examination, and only age-related changes were observed on a head magnetic resonance imaging (MRI) scan, showing no abnormality causing headache. Since he complained that extension of the neck induced headache, cervical MRI was performed, and an intradural extramedullary tumor was present on the left side at the C4/5 level. Thus, the patient was referred to our neurosurgery department.
On the first neurological examination at our department, no abnormality was noted in motor function, but about 8/10 grade hypoesthesia was noted in the left lower jaw and cervical region over the left shoulder. No abnormality was noted in the tendon reflexes, nor was there any pathological reflex.
Pain developed from the left lower jaw to the left auricle and occipital region, which are innervated by C2 and C3 nerve roots. Regarding the property of the pain, it was like an electrical sensation lasting for several seconds, appearing only on extension of the neck, but neither flexion nor rotation caused pain.
On contrast-enhanced MRI of the cervical spine, an intradural extramedullary tumor was present at the C4/5 level, and the spinal cord was compressed rightward (Figures 1a and 1b).
Contrast-enhanced MRI of the cervical spine. (a) Sagittal view: a tumor was present at the C4/5 level; (b) axial view: the tumor compressed the spinal cord rightward.
Under general anesthesia, C4/5 left hemilaminectomy was performed, and the tumor was excised. The tumor arose from a part of the C5 dorsal nerve rootlet and it was excised en bloc. In the postoperative pathological examination, spindle cells were arranged in bundle and spiral patterns showing palisading, and the tumor was diagnosed as schwannoma.
After surgery, no new neurological abnormality or other complications developed, including in the C5 nerve root-innervated region. Pain from the lower jaw to the auricle and occipital region induced by extension of the neck disappeared within several days after surgery, and the tumor had completely disappeared on the postoperative MRI scan. The patient was discharged 8 days after surgery. Hypoesthesia from the lower jaw to the left shoulder had been resolved on outpatient examination after 3 months. At 3 years after surgery, there was no neurological abnormality, pain has been absent, and no tumor has recurred on contrast MRI.
Discussion
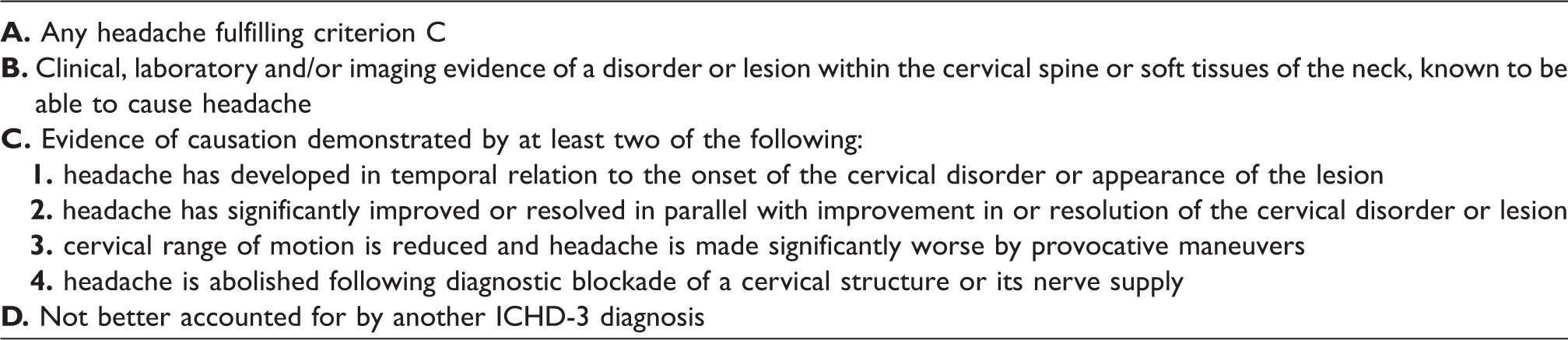
Diagnostic criteria of cervicogenic headache from the International Classification of Headache Disorders, 3rd edition (ICHD-3) (beta version), 2013.
In the present patient, an intradural extramedullary schwannoma arose from the 5th cervical posterior nerve root, and pain was resolved by tumor excision alone, suggesting that stimulation of the nerve root caused the pain. Rosenberg et al. (4) reported a case of headache caused by metastatic tumor infiltration in the C2 nerve root. Regarding cervical intradural extramedullary tumor, Garza (5) reported headache of the ipsilateral occipital nerve-innervated region caused by schwannoma that developed in the craniocervical junction, and Conrad and Merger (6) reported trigeminal neuralgia caused by schwannoma that developed in the upper cervical spinal region and pressed the spinal nucleus of the trigeminal nerve, but, to our knowledge, no case of cervicogenic headache caused by an intradural extramedullary tumor that arose from the middle-lower cervical nerve has previously been reported.
The presence of the spinal nucleus of the trigeminal nerve has been suggested as the mechanism of cervicogenic headache. The spinal nucleus of the trigeminal nerve descends in the spinal cord, reaches the upper cervical spinal cord, and forms a synapse with the upper cervical nerve. It is considered that inflammation that occurred in the 1st to 3rd cervical nerve roots disseminates to the spinal nucleus of the trigeminal nerve and causes facial pain and headache (7,8). However, cervicogenic headache caused by not only upper cervical spinal disease, but also cervical spondylosis and disc herniation at a level lower than the spinal nucleus of the trigeminal nerve, has been reported, and the anatomical details have not been elucidated (9,10). Most pain stimuli entering through the nerve root pass through the dorsal horn of the spinal cord and central gray matter and ascend the anterior spinothalamic tract on the opposite side, but a part of the stimuli enter the ipsilateral ascending spinocervicothalamic tract. Sjaastad et al. assumed that this spinocervicothalamic tract and the spinal nucleus of the trigeminal nerve communicate through anastomosis (2). The spinal roots of the accessory nerve, together with fibers from the anterior branches of the 2nd to 4th cervical nerves, innervate the sternocleidomastoid and trapezius muscle. These are not purely motor nerves, and contain sensory nerves transmitting a proprioceptive sensation and noxious information. This pathway is also considered to explain the anatomical relationship with cervicogenic headache (11).
It is conceivable that overlap of the dermatome and myotome is another mechanism of cervicogenic headache. Dykes and Terzis (12) investigated both the dermatomal and myotomal distribution of the nerve roots using 10 African green monkeys. They concluded that the cutaneous region served by one spinal nerve is actually much wider and much more variable in location than is generally recognized, and the territory of each myotome tended to be larger than the dermatome of the same spinal nerve. Schirmer et al. (13) reported that a significant number of roots innervated a broader range of muscles in the results of intraoperative nerve root stimulation. Stimulation to the C5 root contributed significantly to all muscles in the upper extremity, including trapezius muscle.
We encountered a patient with cervicogenic headache caused by an intradural extramedullary tumor which arose from the 5th cervical nerve root. Previously reported cases of cervicogenic headache were induced by middle-lower cervical spinal lesions and the lesions were mainly extradural, such as cervical spondylosis and disc herniation. This is the initial case report of very rare cervicogenic headache induced by a middle-lower cervical intradural extramedullary tumor.
Although the chief complaint is facial pain or headache, when pain is induced by movement of the cervical region, it may be important to closely investigate cervical spinal lesions in consideration of cervicogenic headache.
Conclusion
A case of cervicogenic headache caused by C5 root derived shwannoma is reported in this article. This is the first reported case of cervicogenic headache induced by a middle-lower cervical intradural extramedullary tumor.
Clinical implications
Previously reported cases of spinal cord tumor-induced cervicogenic headache were due to upper cervical spinal tumors. This is the first report that a middle-lower cervical intradural extramedullary tumor caused cervicogenic headache.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.