
Abstract
Background
Presently, there is no evidence to guide the acute treatment of migraine aura. We aimed to describe the effect of greater occipital nerve (GON) anaesthetic block as a symptomatic treatment for long-lasting (prolonged or persistent) migraine aura.
Methods
Patients who presented with migraine aura lasting > 2 hours were consecutively recruited during one year at the Headache Unit and the Emergency Department of a tertiary hospital. All patients underwent a bilateral GON block with bupivacaine 0.5%. Patients were followed up for 24 hours.
Results
A total of 22 auras were treated in 18 patients. Auras consisted of visual (n = 13), visual and sensory (n = 4) or sensory symptoms alone (n = 5). Eleven episodes met diagnostic criteria for persistent aura (>1 week) without infarction. The response was complete without early recurrence in 11 cases (50%), complete with recurrence in < 24 hours in two cases (9.1%), and partial with ≥ 50% improvement in six cases (27.3%). Complete responses without recurrence were more common in cases with prolonged auras lasting < 1 week than in those with persistent auras (72.7% vs. 27.3%; p = 0.033).
Conclusions
GON block could be an effective symptomatic treatment for prolonged or persistent migraine aura. Randomised controlled trials are still required to confirm these results.
Keywords
Introduction
Migraine aura is present in 20%–30% of patients with migraine (1). According to the International Classification of Headache Disorders, 3rd edition, beta version (ICHD-3 beta), migraine aura typically resolves within the hour, although hemiplegic migraine auras may last longer (2). However, prolonged migraine aura (over an hour) has been reported by 12% to 37% of non-hemiplegic migraine patients (3); migraine aura persisting over a week is classified as persistent aura without infarction in the ICHD-3 beta (2).
Quality evidence supporting the effectiveness of any treatment in the acute management of long-lasting auras is lacking. Documented responses to different drugs have been published, but only as single case reports (4). Over the last few years, only a double-blind clinical trial using intranasal ketamine vs. midazolam for the symptomatic treatment of prolonged migraine aura has been conducted; ketamine significantly reduced the intensity of migraine aura, but had no impact on its duration (5).
Several observational studies and a recent randomised clinical trial against placebo have shown that greater occipital nerve (GON) block may be an effective preventive treatment for migraine, reducing frequency, duration or intensity of attacks within weeks or months (6,7). GON block also appears to have an effect during the acute phase, causing a decrease in pain, allodynia and photophobia (8–12). To date, only three cases of hemiplegic migraine and a case of brainstem migraine have been reported in which a rapid suppression of aura was obtained after GON block (13–15). With this open, non-controlled pilot study we aimed to describe the response to GON blocks in a prospective series of patients with prolonged or persistent migraine aura.
Patients and methods
Study participants
Patients were consecutively recruited between May 2013 and April 2014 from the Neurology Department’s Headache Unit and the Emergency Department at Hospital Clínico San Carlos in Madrid. The study was sanctioned by the Hospital’s Ethical Committee. Patients were included if they met all inclusion criteria, and only after giving their informed consent. All potential candidates agreed to participate in the study. None of the patients was aware of the study prior to consultation.
Patients were deemed fit for inclusion if they met all of the following criteria (1) age over 18, (2) previous diagnosis of migraine with aura by ICHD-3 beta criteria, (3) presenting with prolonged migraine aura over two hours or persistent aura without infarction according to ICHD-3 beta; (4) ability to give a reliable account of symptoms and disease course; and (5) ability to understand the procedures of the study and sign an informed consent form.
If any of the following situations was present, patients were excluded from the study: (1) allergy to local anaesthetic medication of the amide class; (2) pregnancy or breastfeeding; (3) alcohol or illicit substance abuse; (4) coexisting primary or secondary headache diagnosis; (5) previous medical history of severe psychiatric disorders (i.e. psychotic symptoms); (6) previous surgery or trauma in the head or neck areas; (7) severe medical disease active at the moment; or (8) administration of symptomatic treatment for migraine two hours before presentation (analgesics, nonsteroidal anti-inflammatory drugs, triptans or ergotics).
Clinical assessment
The following baseline parameters were recorded for each of the included patients: sex, age, headache frequency, aura frequency, and current preventive and symptomatic medication. Regarding the presenting episode, the type (visual, sensitive, others) and duration of migraine aura until intervention was recorded, as well as coexistence of headache and its intensity using a visual analogue scale (VAS; where 0 is absence of pain and 10 is the worst imaginable pain). GON hypersensitivity was also noted. Magnetic resonance imaging (MRI) and MR angiography were obtained for all patients to exclude the presence of venous, arterial or structural brain disease.
Intervention
Anaesthetic block of both GON was accomplished through the injection of 2 ml of 0.5% bupivacaine using a 30G needle; the insertion site was at one-third of the distance on an imaginary line from the occipital protuberance to the mastoid process. All the procedures were carried out by neurologists with ample experience in nerve blocks.
Concomitant medication and follow-up
Patients received no symptomatic medication within two hours of GON block. If no response to GON block was obtained after 60 minutes (min), the intervention was considered ineffective – these patients were started on rescue medication at this point. Responders within 60 min were advised to avoid symptomatic treatment for migraine during the following hours unless acute exacerbation or worsening occurred. Initiation of preventive therapy was delayed 24 hours; patients already taking preventive medications did not modify their usual dosing scheme.
During the first 60 min after GON block, pain and aura symptoms were monitored at five-minute intervals. Patients were discharged when the clinical situation permitted, and were provided with a form to register symptom evolution. All patients were followed up telephonically 24 hours after the intervention.
Outcome and safety measures
Outcome was assessed taking into account (1) aura resolution (complete, partial – ≥50% subjective improvement – or none); (2) time to maximum effect against aura; (3) aura recurrence within the first 24 hours; (4) pain resolution (complete, partial – ≥50% improvement in VAS – or none); and (5) time to maximum effect against pain. Response was regarded as optimal when complete resolution without recurrence was obtained. Patients were carefully interrogated for possible side effects after the intervention.
Statistical analysis
Results
Demographic and clinical features of patients with prolonged aura (<1 week) and response to GON blocks.

F: female; M: male; VAS: visual analogue scale (0: no pain; 10: the worst pain imaginable); GON: greater occipital nerve; min: minutes.
Patient no. 2 had two attacks: a prolonged aura lasting < 1 week and a persistent aura (see also table 2); patients no. 4 and 6 had two prolonged auras.
Episodic: < 15 days per month; chronic: ≥ 15 days per month for at least three months.
Demographic and clinical features of patients with persistent aura (≥1 week) without infarction and response to GON blocks.
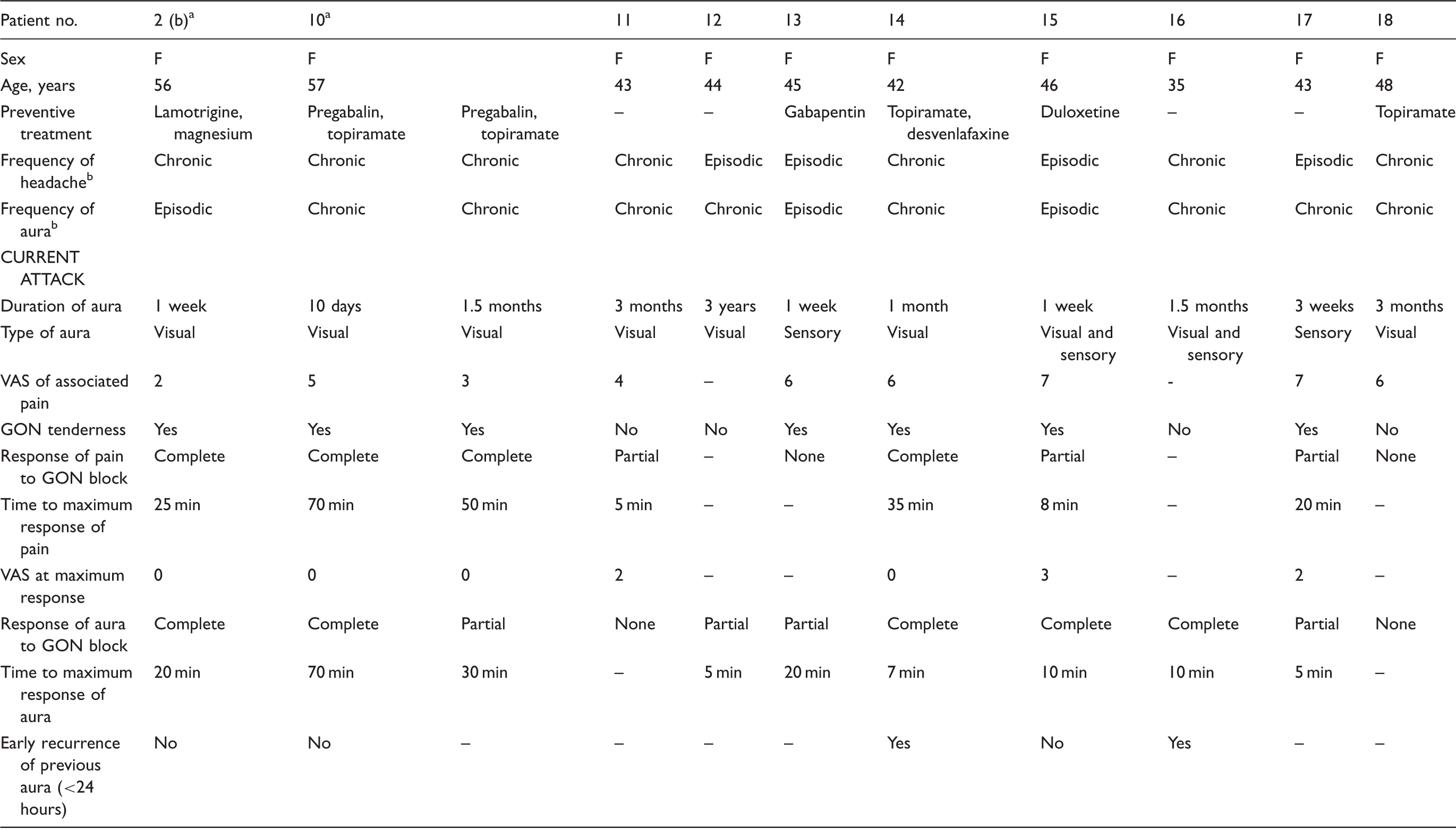
F: female; M: male; VAS: visual analogue scale (0: no pain; 10: the worst pain imaginable); GON: greater occipital nerve; min: minutes.
Patient no. 2 had two attacks: a prolonged aura lasting < 1 week (see also Table 1) and a persistent aura; patient no. 10 had two persistent auras.
Episodic: < 15 days per month; chronic: ≥ 15 days per month for at least three months.
Overall, 19 auras (86.4%) responded to GON blocks. The response was complete without early recurrence in 11 cases (50%), complete with recurrence in < 24 hours in two cases (9.1%), and partial with ≥ 50% improvement in six cases (27.3%). Maximum response of auras, either complete or partial, was reached in 5 to 90 min (median, 10 min; interquartile range, IQR, 6–30 min); the range was comparable in the subgroup with complete response, with the aura symptoms disappearing in 5 to 90 min (median, 10 min; IQR, 6.5–43.5 min). Visual symptoms had earlier resolution than sensory symptoms in the patients presenting with a mixed visual and sensory aura.
Complete responses without recurrence – i.e. optimal responses – were more common in cases with prolonged auras lasting < 1 week than in those with persistent auras (72.7% vs. 27.3%; p = 0.033; RR 2.67, 95% CI 1.01–7.47). Optimal responses were also more common in the cases with prior frequency of auras < 15 days per month than in those with higher frequency (80% vs. 25%; p = 0.01; RR 3.20, 95% CI 1.15–8.94). Otherwise, no association was found between the response of aura symptoms to GON block and the presence or headache intensity in the acute phase, frequency of headaches in the previous three months (either episodic or chronic), presence of GON tenderness or use of preventive medication. Response to GON block in those patients treated twice did not predict response in the following intervention.
Within the group with auras occurring on < 15 days per month, six out of seven prolonged auras and two out of three persistent auras had an optimal response; among those with higher frequency, only two out of four prolonged auras and one out of eight persistent auras had optimal responses (p = 0.698).
Pain responded to GON block in 16 out of 20 cases (80%). Eleven cases showed a complete response (55%) and five cases had partial response (25%). Complete response was not significantly associated with complete aura resolution. Maximum response of pain was reached in 4 to 95 min (median, 22.5 min [IQR, 8.5–38.8]; 35 min [IQR 10–50] for those with complete response). Time to pain response and time to aura response were not significantly correlated (Spearman’s ρ = 0.23; p = 0.435).
Discussion
In our study, about 85% of auras improved after GON block, usually within 30 min, and up to 60% had complete resolution of aura symptoms after the intervention. Response was complete and sustained in 50% of the episodes, with no recurrence of symptoms during the first 24 hours. When the episodes occurred with headache, 80% reported significant improvement of pain and 55% reported complete resolution.
The mechanisms through which GON block improves migraine symptoms remain to be determined. Changes in the activity of the trigeminal-cervical complex (16) may be the underlying mechanism for pain relief. Why aura is also modulated is not entirely clear. A large body of evidence points towards cortical spreading depression (CSD) as the fundamental electrophysiological phenomenon behind migraine aura (17–19). It might be that the modulation of the trigeminal-cervical complex is capable of interrupting CSD and therefore aura (13,15). However, it may well be that GON block has no direct influence on CSD, and that the effect seen on aura has more to do with the suppression of other factors involved in migraine.
In our study, a poorer response rate was seen in those patients with frequent and persistent auras. A systematic analysis of 29 patients with persistent visual aura also revealed that a longer duration of illness was associated with intractability (20). Thus, it is possible that GON block has an effect on some initiating factors of migraine and CSD, but not on those mechanisms responsible for maintaining the aura. Neuroplasticity phenomena may be the cause of this intractability, involving a GABAergic inhibitory circuit dysfunction and an increase in cortical excitability (21,22).
Our study has some limitations. First of all, a small sample size might have precluded us from detecting certain correlations between parameters. The fact that there was no sham procedure to rule out a placebo effect must also be noted. Moreover, despite the fact that all our patients’ auras lasted at least two hours, it is possible that some of the auras may have subsided independently of the intervention. Given all these limitations, our results should be considered as preliminary.
We believe GON block can be an effective procedure in the symptomatic treatment of prolonged or persistent migraine aura. We found that those patients with less-frequent and shorter-lasting auras are more likely to respond. GON block should be considered in patients with long-lasting auras as there are currently no other proven effective therapies. Randomised and controlled clinical trials are still necessary to establish the efficacy of this procedure.
Clinical implications
Anaesthetic greater occipital nerve (GON) block appears to be effective in relieving the symptoms of prolonged or persistent migraine aura. Response is more likely in patients with less-frequent and shorter-lasting auras.
Footnotes
Acknowledgement
This study was presented in part at the 17th Congress of the International Headache Society (Valencia, Spain, 14–17 May 2015).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.