
Abstract
Background
Treatment options for cluster headache (CH) include acute, transitional and prophylactic strategies. We assessed the efficacy and safety of a single occipital nerve block (ONB) in patients with episodic (eCH) and chronic CH (cCH).
Methods
In this prospective, observational study 101 CH were treated with a single ONB using triamcinolone 10 mg and bupivacaine. Attack frequency, pain intensity and side effects were assessed at days 1 and 7 after ONB and thereafter weekly for 60 days until recurrence of attacks.
Results
Baseline mean daily attack frequency was 2.9 ± 2.5 (eCH) and 3.3 ± 2.9 (cCH), which was reduced to 0.7 ± 1.2 (eCH) and 1.1 ± 1.4 (cCH) after one day (p = 0.08 for group difference) and to 1.1 ± 1.6 (eCH) and 1.9 ± 2.3 (cCH) after seven days (p = 0.01 for group difference). In patients with eCH the pain-free period lasted longer compared to cCH (p = 0.004). There was no association between the presence of local anesthesia and treatment response (p = 0.88). No serious adverse events occurred.
Conclusion
ONB is an easy, safe and effective transitional treatment option in case of insufficient response of CH to treatment both in patients with eCH and cCH. Patients with eCH have a better and more sustainable treatment response.
Introduction
Cluster headache (CH) is the most frequent trigeminal-autonomic cephalalgia. CH is characterized by severe unilateral headache and/or periorbital facial pain attacks lasting 15 to 180 minutes. These attacks recur up to eight times per day and are associated with ipsilateral trigeminal-autonomic signs and restlessness. Pain attacks typically show a circadian periodicity and a seasonal rhythm. Episodic (eCH) and a chronic (cCH) form of CH can be distinguished (1,2). About 85% of patients suffer from the episodic variant with pain-attack episodes for weeks or months interrupted by longer pain-free remission periods. The remaining 15% display the chronic form in which attacks occur for more than one year without remission, or with remission periods lasting less than one month.
Treatment options in CH are classified as either abortive, transitional or prophylactic strategies. Attack-abortive acute treatment includes inhalation of oxygen, sumatriptan nasal spray, zolmitriptan nasal spray, and subcutaneous sumatriptan as first-line therapy (2,3). Corticosteroids are used as transitional treatment. Prophylactic therapies include verapamil, lithium and topiramate (2,4,5). Despite these treatments not all patients reach a sufficient level of attack reduction. Beside electrical occipital nerve stimulation and stimulation of the sphenopalatine ganglion (6–8), transitional prophylaxis by blocking the occipital nerve using a perineural applied corticosteroid and local anesthetic might be a useful method to rapidly suppress pain attacks in a cluster bout in eCH or transitional in cCH patients presenting with frequent attacks. A section of the American Headache Society stated in their Expert Consensus Recommendation for the Performance of Peripheral Nerve Blocks for Headaches in 2013 that blockade of the greater occipital nerve can be recommended based on the results of two small, controlled, randomized trials (9–11). However, these two trials included only 13 (10) and 21 (11) patients receiving verum injections and thus do not allow for assessing differences in patients with eCH and cCH. Two other larger studies investigating occipital nerve blockade (ONB) in patients with CH included only patients with cCH (12) or had a retrospective design (13). We conducted a large, prospective, observational study to investigate differences in the short- and long-term efficacy and safety of a single-shot ipsilateral infiltration of both the greater and lesser occipital nerve in patients with eCH and cCH. Furthermore, we assessed whether local anesthesia after infiltration was predictive of treatment response.
Methods
Consecutive patients with a diagnosis of eCH or cCH according to the second edition of the International Classification of Headache Disorders (14) and without adequate control of attacks by standard abortive therapies (oxygen inhalation, triptans) and/or more than one attack per day despite usual prophylactic therapies (corticosteroids, verapamil, lithium, topiramate) were prospectively recruited from July 2010 to November 2011 in the tertiary headache center of the University Hospital Essen. ECH and cCH patients continued the prophylaxis they were taking before ONB. All patients gave written informed consent before inclusion in the study. The study was approved by the local ethics committee.
Injections were made ipsilateral to the side of the CH. A 27-gauge needle was inserted until contact to the periosteum 1 cm beneath the first one-third (greater occipital nerve) and two-thirds (lesser occipital nerve) of an imagined line between the occipital protuberance and the mastoid process, and then slightly withdrawn. Injections were made in four directions, upward, downward, 45 degrees left and right. Then in total 2 ml of a mixture of a long-acting corticosteroid (10 mg triamcinolone dissolved in 1 ml NaCl) and 1 ml of the anesthetic bupivacaine 0.5% was administered at each injection site by experienced neurologists (CG, HS, AT, RW) or anesthesiologist (KG).
Data were obtained using a standardized questionnaire developed by the authors. The questionnaire consisted of 42 items including demographics, headache characteristics (side and localization of headache, age at onset, headache intensity on the 0–10 numerical rating scale (NRS), concomitant underlying persistent pain, accompanying trigemino-autonomic symptoms, length, frequency and intensity of cluster attacks, pain-free days), adverse events, and numbness at the site of injection. The baseline interview before ONB was performed by one of the five neurologists/anesthesiologist. Follow-up interviews were performed at day 1 and 7 after ONB, and thereafter in face-to-face or telephone interview by a trained medical student (JR) weekly for a maximum of 60 days until recurrence of attacks. After that day, patients were called at longer intervals and asked if and when the attacks recurred. Complete treatment response was defined as absence of further attacks for more than 24 hours. Partial response was defined as reduction in attack frequency, duration and intensity of at least 50%. Both were first-time evaluated 24 hours after ONB.
Patients were also asked to rate their subjective satisfaction as a percentage seven days after ONB (0% = no improvement, 100% = complete resolution of pain).
Statistics
Descriptive statistics were used to report means and standard deviations as well as proportions. To evaluate effects of intervention over time in categorical variables, χ2 statistics and Cochran’s Q statistics were applied. To evaluate effects of intervention over time in continuous measures, data were entered into repeated-measures analyses of variance (ANOVA) with the within-subject factor time (baseline, day 1, day 7) and the between-subject factor group (cCH, eCH). Normal distribution of data was investigated using Kolmogorov-Smirnov tests. In case of non-normally distributed data, non-parametric tests were used for group comparisons. In case of sphericity violation in the repeated-measures ANOVA, Greenhouse-Geisser correction was applied. P values < 0.05 were considered statistically significant. All statistical analyses were performed with SPSS version 21.
Results
Baseline
Patient characteristics and status at baseline.

NRS: numerical rating scale; measurement of pain intensity range 0–10 (0 = pain free; 10 = maximum pain intensity). eCH: episodic cluster headache; cCH: chronic cluster headache.
Therapeutic response
In total, 84 (83.2%) of 101 patients had a complete or partial response to ONB. Sixty-one patients (60.4%) reported at least one pain-free day after ONB. The effect was maintained for a mean of 27.3 ± 26.2 days (median 14 days, range 1 to 60 days) in these 61 patients. Forty-one (67.2%) patients with eCH had at least one pain-free day compared to 20 (50%) patients with cCH (p = 0.08). In patients with eCH, the pain-free period lasted significantly longer than in patients with cCH (mean 33.6 ± 26.3 days vs. 14.3 ± 21.3 days; p < 0.001).
Twenty-three (22.8%, 12 with eCH and 11 with cCH) patients reported a partial response and 17 (16.8%, eight with eCH and nine with cCH) patients reported having no benefit at all.
For the dichotomous outcome variable “pain-free vs. not pain-free,” Cochran’s Q statistic showed a significant effect of the intervention over time (p < 0.001). Treatment effect was non-significantly higher in the eCH group compared to the cCH group one day after the injection (p = 0.08), while significantly more patients reported having CH attacks at seven days after the injection in the cCH group compared to the eCH group (p < 0.01). This effect remained significant at day 28 and day 60 (p < 0.01; Figure 1). A Kaplan-Meier survival analysis confirmed the difference between the groups (p < 0.001; Figure 2).
Percentage of CH patients reporting CH attacks at baseline (day 0) and at follow-up. Kaplan-Meier survival analysis.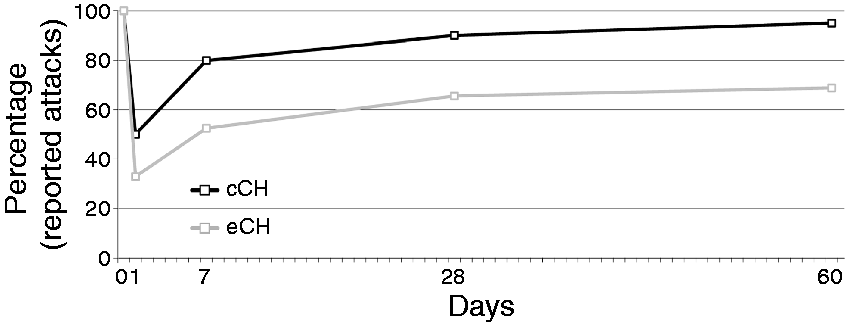

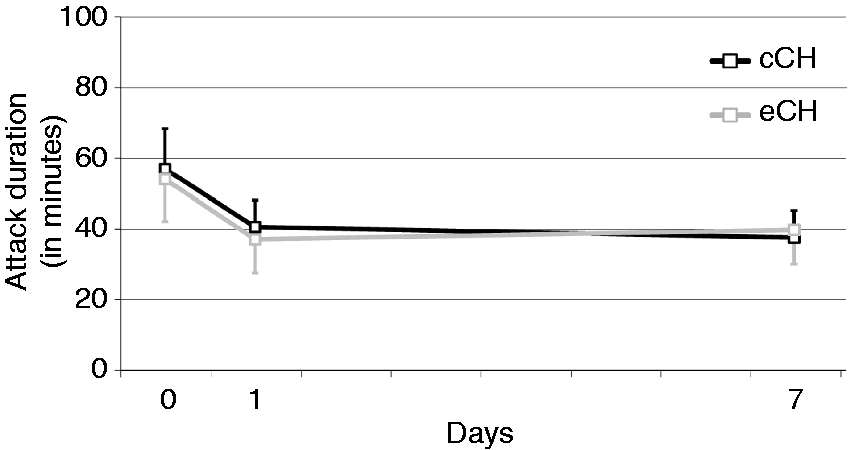
There was also a significant reduction of attack frequency after ONB in patients with both eCH and cCH over time (p < 0.001), while no significant effect of group or group × time interaction was observed (Figure 3). Pain intensity was significantly reduced over time (p < 0.001, Figure 4). A significant interaction (p = 0.001) indicated a larger decrease for eCH than for cCH patients, as can be seen by the group differences on day 1 and day 7 (p < 0.05). Attack duration was also significantly reduced over time (p = 0.04, Figure 5) both in eCH and cCH patients after ONB. Patients who were not free of attacks after ONB (20 in each group) showed a reduction in attack duration from 55.4 ( ±51.7) minutes before ONB to 38.7 ( ±38) minutes one day later, and to 38.5 ( ±38.8) minutes seven days after ONB. The effect of group and the interaction effect were not significant (p > 0.75).
Attack frequency per day (with standard error of the mean) in CH patients at baseline (day 0) and at follow-up. Attack intensity measured with the numeric rating scale (0 = pain free; 10 = maximum pain intensity; with standard error of the mean) in CH patients at baseline (day 0) and at follow-up. Attack duration (in minutes; with standard error of the mean) in CH patients who were not attack free both at baseline (day 0) and at follow-up.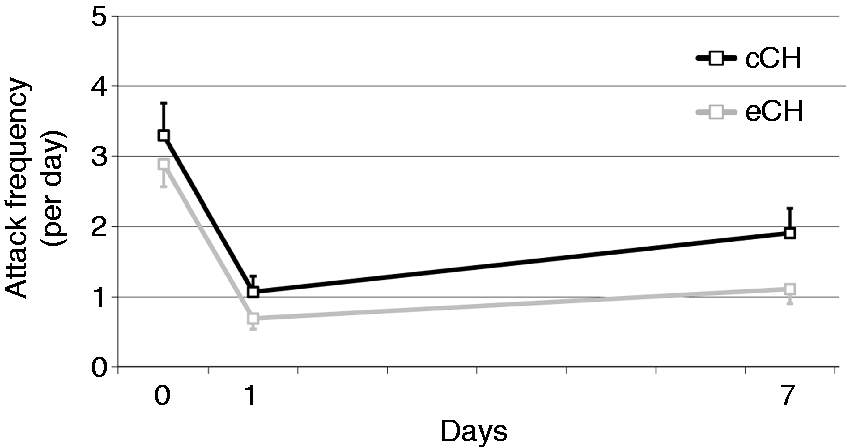

The frequency of continuous background pain significantly decreased over time (Cochran’s Q statistics, p = 0.007). In seven of the 20 patients with background pain (three with eCH and four with cCH), the background pain had completely disappeared on day 7 after ONB.
Seventy-seven (76.2%) of the 101 patients reported at least some subjective benefit. The mean subjective improvement from baseline was 61.9 ± 31.7% (median 70%, range 5% to 100%). Significantly more patients with eCH reported a subjective improvement than patients suffering from cCH (87% vs. 60%, p = 0.002); the subjective benefit was also rated significantly lower in patients with cCH (subjective satisfaction of 43% vs. 70%, p < 0.001).
Seventy (69.3%) patients reported numbness in the area of the occipital nerve the day of the ONB. The percentage was comparable in both groups (cCH: 70%, eCH: 69%; p = 0.90). Twenty-eight (27.7%) patients noted numbness restricted to the area of the greater and lesser occipital nerve, while 42 (41.6%) patients reported more extended numbness of the occipital region. Again, the two groups did not differ (p = 0.37). There was no association between the presence of numbness and treatment response on either day (p > 0.74).
In total, 83% of the patients stated that they would repeat ONB treatment, whereby the number for the eCH group (88.5%) was slightly higher than for the cCH group (75%, p = 0.08).
Adverse events
Adverse events were reported by 11 (10.9%) patients after ONB injection. None of the adverse events was classified as serious. The most frequent adverse events were non-CH (three patients) and tiredness (two patients). The following adverse events were reported by one patient each: continuous pain at the injection site, pressure at the injection point, nausea, tenseness in the occipital muscles, retrobulbar pressure or periorbital pain. None of the patients reported having more than one adverse event. At day 7, no patient reported a persistent adverse event of the treatment.
Discussion
Our large, prospective, observational study shows that a single nerve blockade of both the greater and lesser occipital nerve results in a complete or partial response in more than 80% of CH patients with ongoing daily attacks under standard acute and prophylactic treatment. More patients with eCH than with cCH had a complete or partial response and remissions lasted significantly longer in patients with eCH. No serious adverse events of ONB were observed in our study. In addition, the ONB was well accepted by patients and overall 83% would repeat the treatment.
Overview of studies published on ONB in cluster headache (in chronological order).

Patients receiving verum injection.
ONB: occipital nerve block; eCH: episodic cluster headache; cCH: chronic cluster headache.
Similar to the retrospective study by Gantenbein et al. (13), ONB resulted in a complete or partial response in more patients with eCH compared to cCH in our study. Gantenbein et al. reported that a single ONB resulted in a complete or partial response in 78.6% of the 31 eCH patients and 50% of the 29 cCH patients (13). Furthermore, treatment effect lasted longer in patients with eCH both in our study (mean of 33.6 ± 26.3 days in eCH vs. 14.3 ± 21.3 days in cCH) and the study by Gantenbein et al. (mean of 101.9 ± 152.6 days in eCH vs. 24.6 ± 27.8 days in cCH). These findings were in line with another recent prospective observational study that included only patients with cCH (12). Lambru et al. found that 42% of their 83 patients were pain free for at least seven days (complete response) with a median treatment effect of 21 days after the first injection (12). These consistent results support the use of ONB also in patients with cCH for whom other preventive treatment strategies have not resulted in sufficient treatment response. The longer-lasting treatment effects in patients with eCH might be biased by the natural end of the CH bout in patients with eCH.
The mechanism of action of ONB is not fully understood and it is still under debate whether the effect of ONB is based on systemic/central nervous and/or local processes (10,11). Experimental studies in rats and humans provided evidence for a functional connectivity between cervical afferents from the occipital nerve and the trigeminal nuclei in the brainstem (17–19). Similar to a small retrospective case series (16), we did not observe a correlation between the occurrence of local anesthesia in the territories of the infiltrated occipital nerves and the efficacy of the intervention in our study. It is therefore likely that the corticosteroids are responsible for the main treatment effect in ONB and not the local anesthetic. This finding is also supported by the positive study of Leroux et al., who did not use additional local anesthetics in their injections. It is not possible to determine which steroid dose is sufficient to treat patients with cCH, as direct comparisons of different doses are not available. Our results with a comparatively low steroid dose (equivalent to 1 mg cortivazol and to 2 mg betamethasone) may support the use of a rather low steroid dose. However, no relevant side effects of higher steroid doses were observed in the other studies.
Furthermore, it is not known whether single or serial, uni- or bilateral infiltrations of the occipital nerves are superior to each other. Serial injections were performed in the studies of Leroux et al. (11) and Gantenbein et al. (13). The latter noted a better treatment effect of serial and bilateral injections. This might be due to an enhanced placebo effect or an increasing cumulative steroid dose with systemic effects. However, the retrospective study design and the low treatment numbers in each treatment group prevent drawing a definite conclusion whether serial ONB is superior to a single injection. Only a randomized trial is able to answer this question. Recent studies about ultrasound-guided injections of the occipital nerve have been published (20,21). Whether this technique will result in better treatment responses in patients with CH is also not known.
One-fifth of our CH patients reported a continuous background pain, predominantly located in the area where the pain occurs in cluster attacks, which could be suppressed in a third of these patients after ONB. Further studies are needed to test whether ONB might be a treatment option in CH patients reporting background pain that is usually difficult to treat (22).
Similar to the other published ONB studies, there were no serious adverse events related to the injections in our study and only 10.9% of the patients noted side effects, which is comparable to the study by Gantenbein et al. (14.2%), and lower compared to the study by Leroux et al. (86%), in which patients were injected three times (11,13). Alopecia and cutaneous atrophy have been reported as rare complications after ONB with corticosteroids (23); however, we did not observe these in our study.
The major limitation of our study is lack of a control group to assess placebo effects, which were high in the randomized, controlled study by Leroux et al. (11), but not in the study by Ambrosini et al. (10). It is well known that the placebo response is high in studies with headache patients (both migraine and CH) and moreover in studies using invasive therapies (24–26). The major strength of our study is the high number of prospectively included patients, which allows better comparison of differences between eCH and cCH. Furthermore, we used a standardized questionnaire in prospectively and consecutively treated patients and were not dependent on medical records with missing information, which are used in retrospective studies.
In conclusion, our large prospective study shows again that a simple infiltration therapy of the occipital nerves is efficient and safe in patients with eCH or cCH who are not adequately controlled with standard acute and prophylactic therapies. A better complete or partial treatment response was again observed in patients with eCH.
Article highlights
Occipital nerve block is an easy, safe and effective treatment option in cluster headache attacks. Occipital nerve block is effective in episodic as well as in chronic cluster headache. However, patients with episodic cluster headache have a better and more sustainable treatment response. Side effects of occipital nerve block are mild and occur with low frequency.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Gaul has received honoraria from Allergan, Lilly, ElectroCore, St Jude Medical, Grünenthal, Desitin, Bayer, Boehringer Ingelheim, Autonomic Technologies and Hormosan. Dr Gaul has no ownership interests and does not own any pharmaceutical company stocks. J Roguski has no conflict of interest. T Dresler has no conflict of interest. H Abbas has no conflict of interest. A Totzeck has no conflict of interest. K Görlinger has no conflict of interest. H-C Diener has received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Addex Pharma, Alder, Allergan, Almirall, Amgen, Autonomic Technology, AstraZeneca, Bayer Vital, Berlin Chemie, Boehringer Ingelheim, Bristol-Myers Squibb, Chordate, Coherex, CoLucid, ElectroCore, GlaxoSmithKline, Grünenthal, Janssen-Cilag, Labrys Biologics, Lilly, La Roche, 3M Medica, Medtronic, Menerini, Minster, MSD, Neuroscore, Novartis, Johnson & Johnson, Pierre Fabre, Pfizer, Schaper and Brümmer, Sanofi, St Jude, Teva and Weber & Weber. H-C Diener has no ownership interest and does not own stocks of any pharmaceutical company. R Weber has no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.