
Abstract
Introduction
Headaches after concussion are highly prevalent, relatively persistent and are being treated like primary headaches, especially migraine.
Methods
We studied all new patients seen between August 2008 and December 2009 assessed by a civilian headache specialist at the TBI Center at Womack Army Medical Center, Fort Bragg, NC. We report sample demographics, injuries and headache characteristics, including time from injury to headache onset, detailed descriptions and International Classification of Headache Disorders second edition primary headache diagnosis type.
Results
A total of 95 soldiers reported 166 headaches. The most common injury cited was a blast (53.7%). Most subjects (76.8%) recalled the onset of any headache within 7 days of injury. The most commonly diagnosed headache was a continuous type with migraine features (n = 31 (18.7%)), followed by chronic migraine (type 1.5.1, n = 14 (8.4%)), migraine with aura (type 1.2.1, n = 10 (6.0%)), hemicrania continua (type 4.7, n = 12 (7.2%)), chronic cluster (type 3.1.2, n = 6 (3.6%)) and headaches not otherwise classifiable (type 14.1, n = 5 (3.0%)) also present. The most clinically important was a continuous headache with migraine features.
Conclusion
We present a series of patients seen in a military treatment facility for headache diagnosis after concussion in whom we found migraine, as well as uncommon primary headache types, at frequencies that were much higher than expected.
Introduction
The wars in Iraq and Afghanistan and the surge in interest in sports concussion have produced basic and clinical research opportunities as well as guidelines for return to military duty (1,2) and athletic play (3). Many of these recommendations are based upon findings from physical examinations and psychological testing instruments that are used to measure the short- and long-term impacts of concussions. Specific tests for cognitive function (4–6), balance (7), visual tracking (8) and personality and behavioral changes (9) have been used to document the natural history of mild traumatic brain injury (TBI) and to evaluate potential therapies (10). No specific scale or instrument has yet been created to track the course of headaches attributed to mild TBI. Some of this may be due to the reliance upon recall of events from the onset of headache to a clinical evaluation. Other challenges include concurrent non-cephalic injuries, the subjective nature of head pain, differing expressions and descriptive capabilities of individuals or groups and the level of knowledge of clinicians and investigators. Adding confusion to this is the use of terms such as “mild TBI” or “concussion”, which have been used in different papers and contexts without consistency. In this report, the term “concussion” will be used in accordance with the common language of the army (11) where mild TBI is used synonymously, although differences in outcome may associate with the different terms (12).
In the military (13) and all other environments, diagnosing post-traumatic headache (PTH) requires a well-executed history and physical examination, including accounting for differences in populations (14,15). Headaches after concussion are highly prevalent (16–18), relatively persistent (19) and are usually treated based upon primary headache nosology (20–22). Since the first publications describing military service-related headaches after concussion, the focus has been on prevalence (17,18), associations with other symptoms (22), relationships to post-traumatic stress disorder (PTSD) and other psychological complications (21,23) and treatment (24–26). Attempts to classify headaches have resulted in descriptive groupings (27) and categorical proposals (28–30) and have been hindered by the lack of a gold standard questionnaire. Ongoing research aims to clarify further the relationships between concussion and primary headache diagnosis, with the goal of determining whether extant therapies are adequate or new therapies need to be developed. Since migraine is the most prevalent type (15–17,27,31), usual therapies have been reported, but randomized controlled trials have not.
In a preliminary report on PTH in soldiers seen at the Womack Army Medical Center (WAMC) TBI Clinic, we described the headaches of 25 patients with a focus on phenomenology and diagnosis in which multiple headaches might be described by a single individual, and where diagnostic criteria according to the International Classification of Headache Disorders second edition (ICHD-II) were applied to all headaches (32). In that report, it was noted that the most common headache type was a non-standard, non-classifiable continuous headache with migraine features, meeting the criteria for migraine without aura on at least half of the days of the month prior to initial appointment. In addition, unusual and uncommon headache types were described. This present paper extends those findings to a larger group of 95 patients.
Methods
Subject sample and clinical evaluations
The study population consisted of all new patients referred for headache evaluation to a civilian headache specialist (AGF) and seen consecutively at the then-named TBI Center at WAMC, Fort Bragg, NC, between August 2008 and December 2009. The current name of that clinic is the Concussion Care Clinic. All subjects were active-duty military personnel at the time of initial evaluation. The design was retrospective and observational. All data were confirmed by reviewing medical records (the Armed Forces Health Longitudinal Technology Application or AHLTA) and recorded on a questionnaire-based template that was created for the previous study (31) in order to maximize consistency.
All subjects were clinically diagnosed with concussion, defined as head injury associated with either brief loss or alteration of consciousness, and confirmed by record review. Specific details differentiating complete from partial loss of sensorium were not included, since confirmation was often not possible. Clinical data included: demographics of age, gender, education and rank; causes of injury; and history of pre-injury concussions and headache symptoms. Mean values are reported with their standard deviations.
Injury
Injuries were defined as those to which the soldier attributed symptoms, including blast if an explosion occurred at the time of injury. All other head injuries were categorized as “non-blast”, including less common civilian types, such as parachute jumps.
Headache onset
Time from patient-reported signature concussion to first clinic visit was recorded. Patients were asked to identify the injury to which they attributed the onset or worsening of headache(s) and the time between that concussion and the onset of each headache type. The time of headache onset after attributed trauma was reported on a seven-point scale (immediate, less than 1 day, within 7 days, less than 30 days, 1–3 months, 3–6 months and greater than 6 months).
Headache characteristics
Headache descriptions were recorded in detail at the time of initial face-to-face evaluation and were entered into a template containing language and “keywords” derived from the ICHD-II. Soldiers were asked to list the number (up to three) and characteristics of each headache experienced in the last month prior to evaluation. Continuous headache was described as never having any time during waking hours without headache. If any time during a day was headache free, they were coded to “non-continuous”. Only one continuous headache was coded and up to two non-continuous headaches were recorded. Symptom-specific questions were repeated for each headache, including: the time of onset in relationship to head injury; the location and area of pain; the character, severity (none: 0, mild: 1, moderate: 2, severe: 3) and duration; modifiers, including triggers for episodic headaches; factors of worsening or relief, including those for continuous headaches; and associations, including photophobia, phonophobia, nausea/vomiting, neck pain and symptoms of the eye and/or nose. Patients were also asked about warning signs or symptoms for episodic headache or worsening of baseline headache using verbal and pictorial descriptions including, but not limited to, classical migraine aura, such as fortification spectra and scintillating scotoma.
Headache diagnosis
Headache characteristics were then codified for assigning criteria to the ICHD-II primary headache diagnosis “type” that were in use at the time of evaluation. Chronic PTH attributed to mild head injury (5.2.2) was not listed, as it was considered to be the primary clinical diagnosis. Secondary headaches were confirmed and coded. The most clinically important headaches were determined by the patient and the authors for the purposes of creating larger categories.
A false category, 2.3/1.x, was created for patients who described a headache type that was continuous which: (1) at baseline did not meet the criteria for tension-type headache because of an inclusive and regular migraine criterion; or (2) when worse, would attain other features and meet the criteria for migraine without aura. This category was created since this was the most commonly reported headache using verbal and visual cuing (e.g. a single headache that was continuous, but with migraine features, especially on more than 15 days in the previous month) (2.3/1.5.1), which we titled continuous headache chronic migraine (CHCM). (Note that the diagnosis of Hemicrania Continua (HC) was treated according to the International Classification of Headache Disorders – III (beta) (ICHD-III), which moved HC to the trigeminal autonomic cephalalgia (TAC).)
Diagnostic categories
All individual headaches were grouped according to the four major categories of primary headaches listed in the ICHD-II, and frequencies were recorded for each. We then grouped patients according to most clinically important headache regardless of total number of headaches described ad hoc by the clinician at the time of data recording and based upon the record review. This grouping of patients by the clinically most important of the reported headaches was confirmed independently and post hoc using an algorithm that was created for that purpose (Figure 1). The algorithm, accounting for migraine symptoms and reported headache severity, sequentially applied the following criteria:
Reported headache pain (severity): for this criterion, severity ratings obtained from the original scales (0–4) were utilized. Number of migraine symptoms reported (aura, nausea/vomiting, photo- or phono-sensitivity and neck pain). Patient activities during a severe headache, including maintenance of pre-headache activity, medication and forced rest. Monthly frequency of headache occurrence for non-continuous headache. Flowchart for determining the most important headache (HA) for each subject.

Cohen's k coefficient was utilized in order to assess the degree of agreement between these two methods of determining a categorical variable: the clinically most important headache. k estimates greater than 0.80 provide evidence of strong agreement (33).
Approval for this study was obtained from the Institutional Review Board of WAMC with timely renewals as required.
Results
Demographics
The sample of 95 soldiers consisted of 89 males (93.7%) and six females (6.3%) with a mean age of 31.3 ± 7.4 years (median: 30.0; minimum, maximum: 20, 49). Sixty-seven (70.5%) had some college or graduated, and the majority (71/95; 74.7%) were junior enlisted or non-commissioned officers. Thirteen (13.7%) patients reported a prior history of recurrent headache, all with unknown or no diagnosis. A total of 36/91 (39.6%; data missing for four soldiers) reported a history of concussion prior to military service. A total of 24/85 (28.2%) reported a family history of headache.
Injury characteristics
The most common injury cited by the soldiers as causative was blast (53.7%), followed by parachute jump (23.2%) and motor vehicle accidents (10.5%). The mean time from injury to the initial consultation was 27.6 ± 26.6 months (median: 20; minimum, maximum: 1, 132).
Headache characteristics
Headache characteristics (sample n = 95).

Statistics are counts (percentages in parentheses), except where indicated.
IQR: interquartile range.
Headache onset
Most (76.8%) subjects recalled the onset of any headache within 7 days of injury. The 22 subjects who did not report headache onset within 7 days of injury were divided into three sets (Supplemental Table 2). The first set (n = 13) reported a specific time of headache onset: seven (53.8%) reported more than 7 days but less than 30 days from injury; two (15.4%) reported between 1 and 3 months; one (7.7%) reported between 3 and 6 months; and three (23.1%) reported greater than 6 months. A second set (n = 7) had unknown times of headache onset, based upon patient response or inability to confirm time of onset from chart reviews. Only one had a continuous headache (CHCM). In a third set (n = 2), multiple concussions were sustained and subjects could not identify a signature or approximate date. Of the patients who did not report headache onset within 7 days of injury, 4/22 had more than one headache type (<30 days: two patients; multiple concussions: two patients).
Headache diagnosis
International Classification of Headache Disorders second edition diagnoses of all headaches within major categories a .
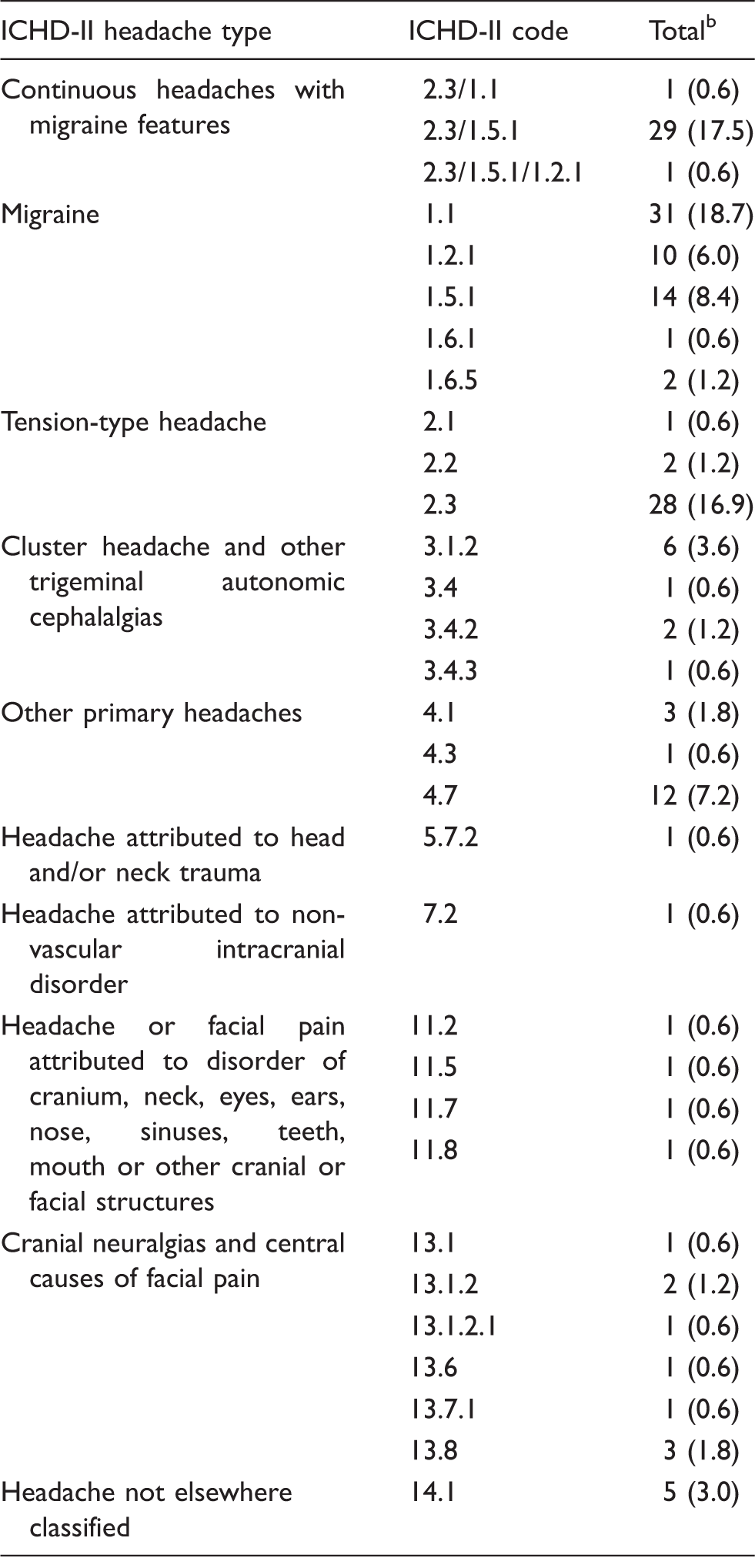
This table summarizes all headaches observed (n = 166); some individuals were diagnosed with multiple headaches – see text.
Percentages do not sum to 100 due to rounding; values are counts (percentages in parentheses).
ICHD-II: International Classification of Headache Disorders second edition.
Highlighted amongst patients (n = 95), chronic migraine type (1.5.1) occurred in 14 (14.7%), migraine with aura type (1.2.1) occurred in ten (10.5%) and HC type occurred in 12 (12.6%), including two who had daily but non-continuous pain. Chronic cluster type was diagnosed in six patients (6.3%), as were other primary headaches, including primary stabbing type and primary exertional headache in three each (3.2%). Nummular headache was diagnosed in one patient, with six (6.3%) secondary headache types and ten (10.4%) with cranial neuralgias and central causes of facial pain (ICHD-II 13.x). Five soldiers had headaches not otherwise classifiable (Supplemental Table 1 displays the individual patients and all diagnoses).
Headache profiles
There were 53 individual combinations or “profiles” for patients (Supplemental Table 3), and 40 (75.5%) of these profiles contained more than one headache. The top seven profiles described 43.2% of subjects (n = 41); only five of these patients did not have a continuous headache.
Most clinically important
Final categories by major classification for most clinically important headache identified a .
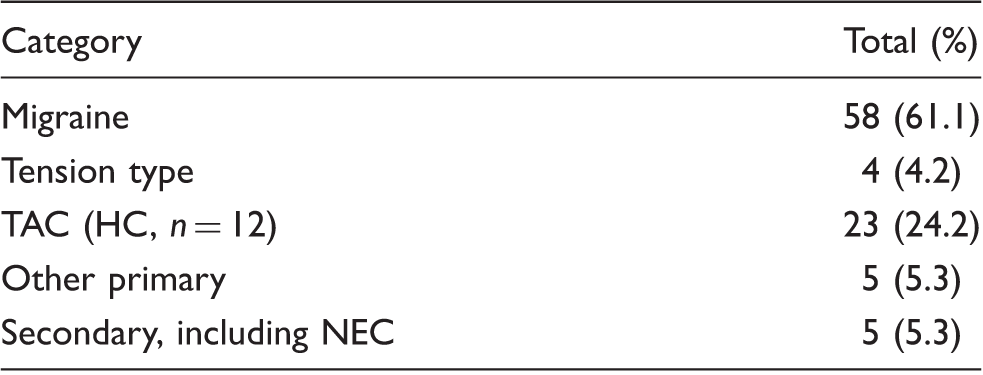
Continuous headache chronic migraine is included as migraine. HC was included in the TAC category following the International Classification of Headache Disorders third edition.
HC: hemicrania continua; NEC: not elsewhere classified; International Classification of Headache Disorders second edition code 14.1; TAC: trigeminal autonomic cephalalgia.
Discussion
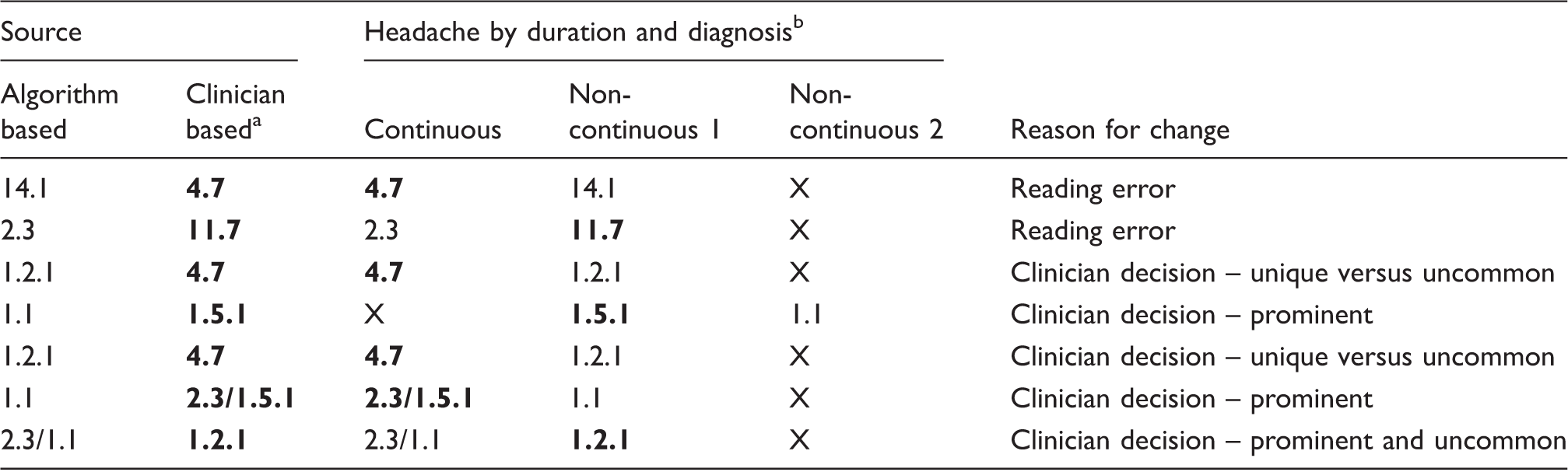
The classification of headaches after concussive or non-concussive injury to the head, neck or face depends on many factors. Originally classified as “concussion reactions” under Category VI.B, non-migraine vascular headaches, of the American Academy of Neurology Ad Hoc Committee on Classification of Headache, PTH was included with, amongst others, carbon monoxide poisoning, caffeine “circulatory insufficiency in the brain” and “hangover reactions” (Supplemental Figure 1) (34). The International Headache Society Classification of Headache (first edition) (35) describes chronic PTH according to “significant” or “minor” head trauma (Supplemental Figure 2) where: “Headache occurs less than 14 days after injury, Headache continues more than 8 weeks after injury and there is International Classification of Headache Disorders (second edition) (2004) (35). International Classification of Headache Disorders (third edition, beta) (36). Discordances between post hoc algorithm and clinician diagnosis of most clinically important in individual subjects. Most clinically important are displayed in bold. “X” indicates that no headache was reported.
Our group of active-duty service members presented with a multitude of headache descriptions at an average of more than 2 years from their reported signature injury. We used direct interview and medical record review to confirm concussion or “symptoms and/or signs diagnostic of concussion” (37) and diagnosed each headache according to the extant classification in use at the time. The most common diagnosis was a mixed CHCM type, with the next most common types being migraine without aura and chronic tension type, either continuous or non-continuous. Overall, the largest category of described headaches was migraine, and we noted that continuous headaches could occur across diagnostic categories. There were non-continuous headaches of the less common type, including TAC and other primary headaches.
We describe a variety of onset dates, including a group of headaches that were reported to begin later than 14 days (35) or 7 days (36,37) from the time of injury. All patients had headaches that were persistent for more than 3 months after head trauma, including those few who were seen within fewer than 3 months after their concussion. The time from injury to evaluation was variable, but on average, we found that many still had headaches at 2 years after concussion.
We did not attempt to apply statistical formulae or to ascribe any possible relationships to demographics or injury type or the outcomes that we observed (not reported here). The primary goal of this study was to demonstrate that close assessment of patients in this population can yield diagnosis types other than migraine type.
Why does this matter? In our clinical observation of a population of mostly male soldiers, there are more than just migraine features with which to deal. In a recent epidemiologic sampling at 1 year post-injury of mixed severity, migraine and probable migraine types were most prevalent (54%), followed by tension type (21%), cervicogenic (4%) and unclassifiable (21%), with those with only mild TBI having similar rates of migraine/probable migraine (49%), tension type (32%), cervicogenic (4%) and unclassifiable headaches (17%) (38). Our finding of other headache types may suggest that prescription of medications with efficacy in other diagnoses should be considered; for example, verapamil in cluster type, indomethacin in short duration or hemicrania types, etc. These subtleties may not be apparent in larger epidemiologic studies or clinic trials using survey or questionnaire data to determine control drug trials (e.g. we found that chronic migraine type may have better outcomes than continuous type when treated with onabotulinum toxin A, and in that study, the time from injury to treatment may have improved the efficacy) (39). In addition, the anecdotally high failure rate of the standard of care for PTH of the migraine type may relate to the presence of changes expressed as a second and perhaps more unique headache diagnosis types.
In developing guidelines and standard operating procedures, the gold standard is always going to be clear delineation of diagnosis and the application of evidence- or consensus-based treatments. Our findings may have implications for primary care or general neurology in the military setting, where stratification of medication or procedural management is important, but Continuation on Active Duty and deployment readiness are paramount. Finally, the factors that lead to persistence may be different for more non-specific headache types, such as tension type or tension type with migraine features (the largest group combined), and in our future reports, we will address the question of such associations.
The shortcomings of a phenomenological study of individuals with subjective complaints are obvious. Reliance upon patient report always presumes some difficulties in addition to the recall of injury and symptom progression over time. These may also be based upon education, prior experience, ability to express symptoms consistently and possible motive or intent on the part of the individual to gain attention or secondary advantages. We did not address any of these issues, relying upon a historical classification system in current use at the time of the patient's initial evaluation. We were able to show that the criteria were applicable in the vast majority of cases.
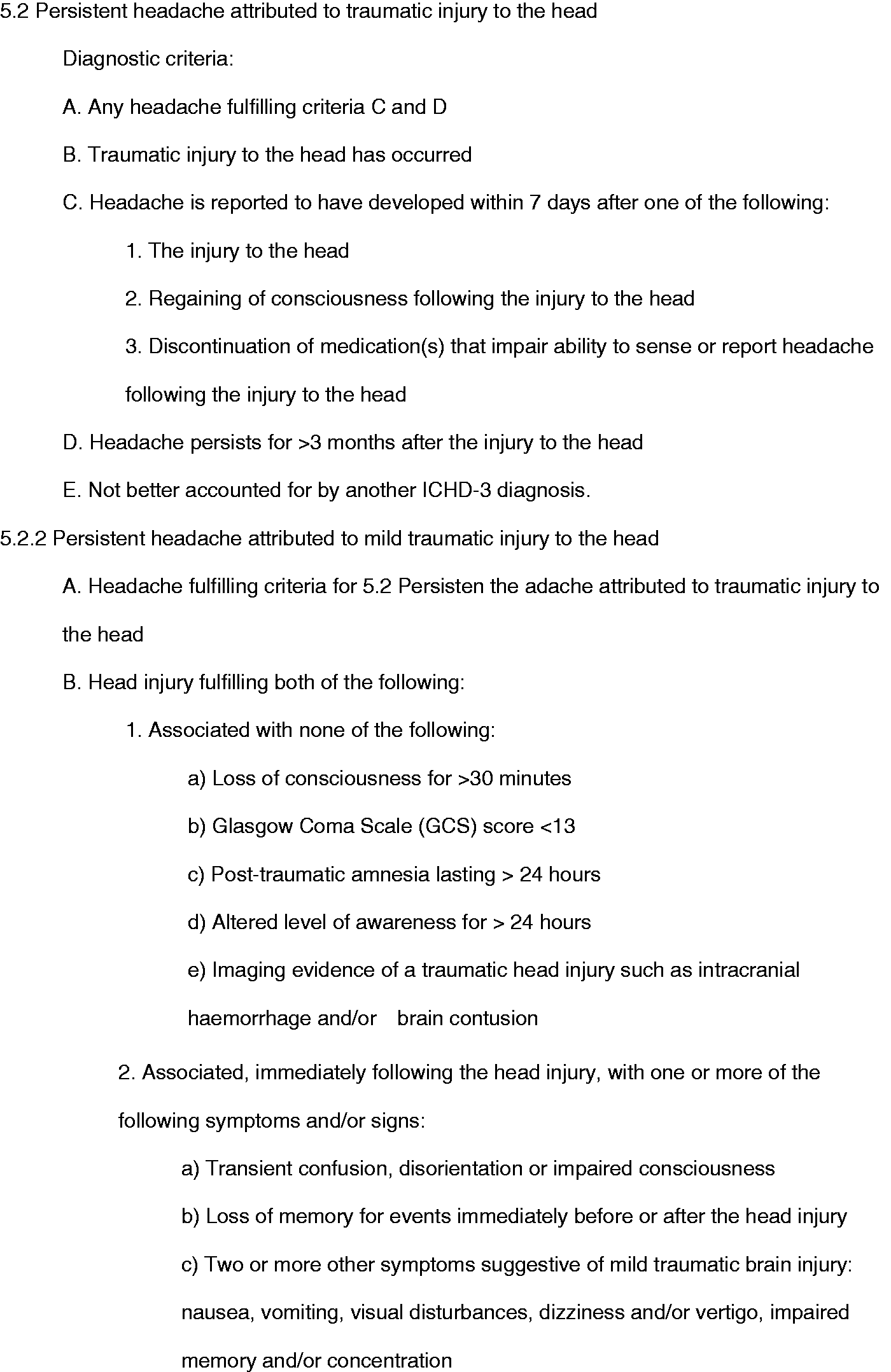
Additional criticism of the work could include what might be called “shoe-horning” symptoms into diagnosis typing. The utility to applying criteria to individual headaches in specific patients is the cornerstone of headache medicine. Changes to the criteria for PTH and chronic PTH (Figures 2 and 3; Supplemental Figures 1 and 2) through time may have introduced more specific terms, with the most recent ICHD-III beta recognizing that “any headache” that could be attributed differs substantially from “no typical characteristics”. Application of this criterion may need to be tested in field trials. Those same authors also allow for onset after 7 days post-injury.
Using these ideas, we proposed that clinically diagnosed and retrospectively reviewed medical records could yield criteria that were positive diagnoses for individual headaches and individuals with PTHs. These were based upon best clinical judgement at the point of contact and on the analysis of granular details collected retrospectively. Best attempts to match criteria exactly were made, and choices between diagnoses, where unclear, aimed to best match existing primary headache classification.
Another prominent concern must be that study participants may be biased to report a close temporal association between the impugned injury and the timing of headache onset (i.e. < 7 days post-injury). Historically, assumptions have been that highly selected responders may have negative motivational factors related to monetary awards (e.g. disability benefits) (40), comorbidities (41) or distress related to the context of injury (e.g. directly attributable to concussion, such as PTSD) (24).
In light of these and possibly other legitimate arguments, our highly selected cohort that was referred for definitive evaluation to a headache specialist at an average of 2 years after headache onset demonstrated a surprisingly high prevalence of cluster and other TAC-type headaches, leading some to be legitimately skeptical of our reporting. The literature has very few cases of these types of headaches attributed to mild head trauma. Those arguing thus could further suggest that the absence of contemporaneous medical records describing headache phenomenology and symptomatology from the moment of concussion to the immediate period afterwards led us to rely upon a retrospectively determined timing of headache based upon a forced choice of fixed time periods for headache onset. Acknowledging this during our review, we strictly adhered to criteria, including those with “probable” TAC type, all having only one missing criterion. Whether this occurrence relates to patient variables or transition in central and peripheral structures implicated in TAC-type headaches or problems of symptom interpretation, etc., cannot be known. We note that a possible association with changes in hypothalamic–pituitary function has been proposed in concussion (42,43). Speculating on the onset of a more complex headache disorder such as these TAC types, it is worth noting that three out of ten of our subjects had onset either unknown onset, onset at >7 but < 30 days post-injury or onset after multiple injuries. Whether this should be interpreted as a change in anatomy or physiology (44–46) is an open question, including whether the entire discussion is moot (e.g. headache is not a post-concussive complication) (30). Opposing this argument, imaging results in mild TBI have shown both functional and anatomical changes (47,48).
In an attempt to confirm the clinical impression using this approach based on objective criteria, one of us (JSK) created an algorithm to test whether control of severity, migraine criteria and headache-associated disability could replicate the clinician-determined diagnoses of the most clinically important headaches. Use of the clinician's sense of uniqueness to stratify headaches in patients with more than one type of headache, as well as determination of the most clinically important headache, was largely (although not completely) replicated. In patients with more than one type of headache, we found concordance in all but a few comparisons (>90%). Replication also included the relatively high prevalence of TACs observed. Though some clinician-detected nuances were not accounted for by this algorithm, this type of approach may offer future opportunities to create methods for sub-classifying secondary headaches of no known characteristics.
Lastly, few statistics were applied to the data we present. This leaves unanswered questions such as: are there predictors of diagnoses or types that could be easily used to help clinicians at all levels to treat or prognosticate? Do patients with certain headache types have different injuries? Do headache types in combination with medical histories and demographics predict outcomes?
In conclusion, we present a series of patients seen in a military treatment facility for headache diagnosis after concussion. Prior publications in non-traumatic headaches have attempted to view diagnosis through a microscopic (49–53) or phenomenological lens (54,55) for the purposes of clarifying the heterogeneous nature of even the most common headaches. To that end, where there has been reliance upon field trials for validations (56–60), including PTH (61), there have also been refutations of the claims for classification as being truly representative of the phenomenology and thus epidemiology of individual headache diagnoses (62).
We did find that the prevalence of migraine is high, but we also included headache types that met specific criteria for other primary headaches. We were able to group patients and headaches by creating “profiles” and, lastly, by identifying the most clinically important headache. We found only five soldiers each (5.3%) in which tension type, other primary or secondary headache were most important. A review of the last 10 years of publications (search terms “post traumatic headache”) (63) showed that 26% (121/458) were under the categorical heading that included cervicogenic. On the other hand, we found essentially no cases in which cervicogenic was either the only headache type or the most important type. However, migraine type was most prevalent, but, interestingly, TAC type was the second most prevalent, raising the possibility that more focal, severe and episodic headaches may suggest a relationship with the mechanism of injury. In an historical footnote, those papers relating cluster headache patients to head injury or violence suggest that the pugnacious nature of males with cluster headaches, including the authors' noting of alcohol seeking, may be a part of the reason for some of this association (64–67). The relevance of this to service members is not implied, but war, by definition, involves fighting. In this same vein, the generalizability of all of the diagnostic findings reported here may be limited to specific populations and/or injuries.
This disparity may suggest that intensive diagnostic interview in combination with stringent applications of classification can help the clinician determine upon which of the possibly multiple headache types to focus evaluation and treatment. Lastly, the results of a directed diagnostic process may help to determine clinical outcomes or surrogates in lieu of reliable biomarkers. Future prospective and longitudinal studies are indicated.
Article highlights
Ninety-five soldiers injured during the wars in Afghanistan and Iraq were seen consecutively by a certified headache specialist for diagnosis. The most common diagnosis was a continuous headache with migraine features. Twenty-two subjects did not report the onset of headache within the 7 days stipulated by the International Classification of Headache Disorders. Of these, seven had unknown onset and seven had onset between 7 and 30 days. Uncommon headaches, including cluster headaches, were seen in higher prevalence than would be expected, raising the possibility of central nervous system and hypothalamic–pituitary changes. An innovative approach using an algorithm based upon most severe headache characteristics was employed, showing a high level of correlation with clinically determined diagnosis.
Footnotes
Disclosure
The views expressed herein are those of the authors and do not reflect the official policy of the Department of the Army, Department of Defense, the Uniformed Services University or the US Government.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: One of the authors (AGF) received salary support from the Defense and Veterans Brain Injury Center and General Dynamics Information Technology for work associated with this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding was received from the Defense and Veterans Brain Injury Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.