
Abstract
Introduction
Colloid cysts are histologically benign but can present with a broad spectrum of symptoms. A systematic review of the literature did not reveal any patient-centered data on the headache disability and quality of life (QoL) of these patients.
Methods
This is a retrospective cohort study of 187 colloid cyst patients from the Colloid Cyst Survival Group who completed a survey that included demographic data, clinical data, a modified QoL survey (SF36v2), and a headache disability inventory or index (HDI).
Results
Using multivariable linear regressions, we confirmed that the physical (PCS) and mental (MCS) components of SF-36 were significantly increased in the surgery group after adjustment for various baseline characteristics (p = 0.025; p = 0.006). Self-reported headache disability was significantly decreased with surgery when adjusted for the same baseline characteristics (p = 0.02). Finally, patients with an incidental diagnosis of colloid cyst reported similar benefits from surgery in PCS, MCS and HDI.
Conclusion
Our results suggest that colloid cyst patients who underwent a surgical resection self-report a better QoL and less headache disability compared with patients who did not undergo surgery. Future prospective studies with baseline measures of QoL are indicated to confirm our findings.
Introduction
Colloid cysts are rare, histologically benign, intracranial tumors located on the roof of the third ventricle in proximity to the foramen of Monro (Figure 1) (1,2). They make up 0.5% to 2% of all intracranial tumors (3,4) and are prone to a gradual or acute blockage of the ventricular system. Blockage can result in hydrocephalus and sudden death (Figure 1) (5–9). Furthermore, this patient population has been shown to have a large spectrum of symptoms such as headache and other neurological sequelae (2,10,11).
Imaging and intraoperative visualization of a colloid cyst case. (a) Sagittal T1-weighted magnetic resonance imaging in a colloid cyst patient with hydrocephalus two days preoperatively, and (b) one day postoperatively. Complete resection of the lesion was achieved. (c) Endoscopic visualization of a colloid cyst at the third ventricle that is protruding through the Foramen of Monro blocking the CSF flow and the anatomy at the lateral ventricle is distorted. This can be resected through a transforaminal approach. (d) Normal anatomy without tumor. The Foramen of Monro is accessible without obstruction of the CSF passage and all the structures can be clearly visualized. SV: septal vein; Fx: fornix; dCP: distorted choroid plexus; CP: normal choroid plexus; TSV: thalamostriate vein; CSF: cerebrospinal fluid.
The classic clinical vignette for a colloid cyst is a paroxysmal headache attack with changes in posture. However, with the advent of computed tomography (CT)/magnetic resonance imaging (MRI), such presentation is quite rare. Desai et al. (10) reported that only two out of 105 patients in their cohort had such a presentation. Chronic headache, however, was reported in 92% of their patients, and were described as generalized and intermittent in nature. Although many studies have reported chronic headache as being the most common symptom of colloid cyst patients, there are few data on how disabling such headaches can be. Furthermore, an extensive survey of the literature failed to reveal any data concerning the quality of life (QoL) of colloid cyst patients. The value of patient-centered data has become increasingly apparent. For instance, Harreld et al., have found that patient satisfaction correlates more with subjective than objective measures for patients undergoing shoulder arthroplasty (12). Desai et al. indicated that 92% of patients had headaches, 72% had papilledema, 26% had ataxia, and 9.5% had short-term memory deficits (10). Therefore, we hypothesized that the QoL of these patients is significantly affected by the sequelae of these cysts. It was our aim to assess both headache disability and QoL, in the colloid cyst population and across surgery vs. no surgery cohorts.
Methods
Patient population
The Colloid Cyst Survivor Group is an online support group that aims to provide an environment in which colloid cyst patients and their families can interact and exchange information that comes from a personal rather than medical viewpoint. Members of this group were solicited by one of the group administrators to complete an online questionnaire that included clinical and demographic information. All patients with a diagnosis of colloid cyst were eligible for this study. Surveys were collected from August 23, 2013 to October 22, 2013. The response rate was 31% (221/720). After excluding patients who did not fully complete the Short-Form Health Survey (SF-36) or Headache Disability Inventory (HDI) survey, there were 187 patients left. The Johns Hopkins Institutional Review Board (IRB) Committee approved this retrospective study.
Outcome measures
In order to assess QoL, we used a modified version of a well-validated, sensitive and reliable survey, the SF-36V2. This survey was modified only in the formulation of some questions, however, it does not differ from the original in its scoring of QoL parameters (13–15). The SF-36 survey is a multi-item scale that measures eight health concepts: physical functioning (PF), role limitations because of physical health (RP), bodily pain (BP), social functioning (SF), general mental health (MH), role limitations due to emotional problems (RE), vitality or energy/fatigue (VT), and general health perception (GH). These measures can be aggregated into a physical component (PCS) and a mental component (MCS) summary score. The higher the score, the better the QoL. Each of these scores has been normalized to the United States (US) population (mean = 50, standard deviation (SD) = 10), meaning that scores above and below 50 are considered above and below the mean, respectively, in the US general population. We also report an SF-6D score that was derived from MCS and PCS scores based on a conversion equation provided by Hanmer (16). SF-6D can be used to estimate quality-adjusted life years (QALYs). The Henry Ford Hospital HDI, a 25-item survey, is considered useful for assessing the impact of headache on daily living (17). Patients who self-report mild/moderate headaches have mean HDI scores of 32/33, whereas patients with severe headaches have mean HDI scores of 60 (17).
Statistical analysis
Continuous variables are presented as mean with SD if normally distributed and as median with interquartile range if not normally distributed. Categorical variables are presented as frequency with percentage. P values for categorical variables were computed using chi-square when cell size was greater than five and Fisher’s exact test otherwise. For continuous variables, normal distribution was assessed using the Shapiro-Wilk test. For not normally distributed variables, a Wilcoxon rank sum test was used. Comparison of means for variables with more than two categories was assessed using a one-way analysis of variance (ANOVA) with a Bonferroni correction when needed. P values less than 0.05 were considered significant. Multivariable linear regression models were used to assess the impact of surgery on SF-36 and HDI scores, adjusted for baseline characteristics including: age at diagnosis, age at survey, gender, country, family history, incidental diagnosis, size of the cyst at diagnosis, and headache at diagnosis. Finally, to assess whether our findings are applicable to patients with incidental findings of colloid cyst, we included an interaction term in each multivariable regression. The interaction term that we used is the product of “surgery” and “incidental diagnosis.” Statistical analysis was performed using STATA version 12.
Results
Patient demographics
Baseline characteristics in patients diagnosed with colloid cysts.

P values represent a statistical comparison of the no surgery cohort to the surgery cohort.
P values were computed using Fisher’s exact test.
USA: United States of America; UK: United Kingdom; pre-op: preoperative.
Reported symptoms
Patient reported symptoms in the interval between diagnosis (dx) and survey.

P values represent a statistical comparison of the no surgery cohort to the surgery cohort.
P values were computed using chi-square.
Surgery vs. no surgery cohort
Baseline characteristics (preoperative)
A total of 131 patients (70%) reported having a surgical resection of their colloid cyst. Patients who underwent surgery in general had larger colloid cyst size compared to those who did not undergo surgery (p < 0.001) (data collected as ordinal variable) (Table 1). There were no significant differences between the surgery and no surgery cohorts in age group, gender, country of origin, headache, family history, time since diagnosis, and incidental diagnosis (Table 1). Anxiety and panic between diagnosis and survey were more common in patients who did not undergo surgery as compared to those who did undergo surgery (62% vs. 40%, p = 0.006) (Table 2). Experiencing unbalanced feelings or ataxia between diagnosis and survey was also less commonly reported in the surgery cohort (p = 0.04 and p = 0.018, respectively).
Subjective QoL and headache disability (postoperative)
Self-reported quality of life (QoL) and headache disability (HDI).

P values represent a statistical comparison of the no surgery cohort to the surgery cohort.
SF-36 and HDI were not normally distributed in our patient population. P values were computed using non-parametric Wilcoxon rank sum test. SF-6D can be used to estimate quality-adjusted life years (QALYs). SF-6D values were derived from MCS and PCS scores.
HDI: Headache Disability Inventory; PCS: Physical Component Survey; MCS: Mental Component Survey; SF-36: Short-Form survey 36.
Multivariable linear regression of surgery on SF36 and HDI.

A multivariable linear regression model was used to assess the impact of surgery on SF36 and HDI adjusted for baseline characteristics (age at diagnosis, age at survey, gender, country of residence, family history, incidental diagnosis, size of the cyst at diagnosis and headache). In order to assess whether an incidental diagnosis modifies the impact of surgery on our primary outcomes, an interaction term was created using the product of surgery and incidental diagnosis, labeled “surgery ×incidental.”
Patients who did not report headache at baseline were excluded from the analysis of HDI.
HDI: Headache Disability Inventory; PCS: Physical Component Survey; MCS: Mental Component Survey; SF36: Short-Form survey 36; CI: confidence interval; coef: coefficient.
Incidental diagnosis
In all of these regression models, there was no significant association between incidental diagnosis and QoL or HDI. When adding an interaction term (product of “surgery” and “incidental diagnosis”) to all three models, incidental diagnosis did not modify the impact of surgery on MCS (interaction term: p = 0.67) and HDI (interaction term: p = 0.96) (Table 4). There was a marginal effect modification on surgery and PCS (interaction term: p = 0.065) (Table 4) with a coefficient of –7.5, which represents the difference between the slope comparing surgery to no surgery for patients with an incidental diagnosis and the slope comparing surgery to no surgery for patients without an incidental diagnosis. In other words, patients with an incidental diagnosis would gain fewer benefits from surgery in terms of the physical components of QoL compared to patients without an incidental diagnosis.
Predictors of surgical outcome
Indication for surgery: Hydrocephalus vs. no hydrocephalus
Predictors of surgical outcomes and patient-neurosurgeon (NS) relationship.
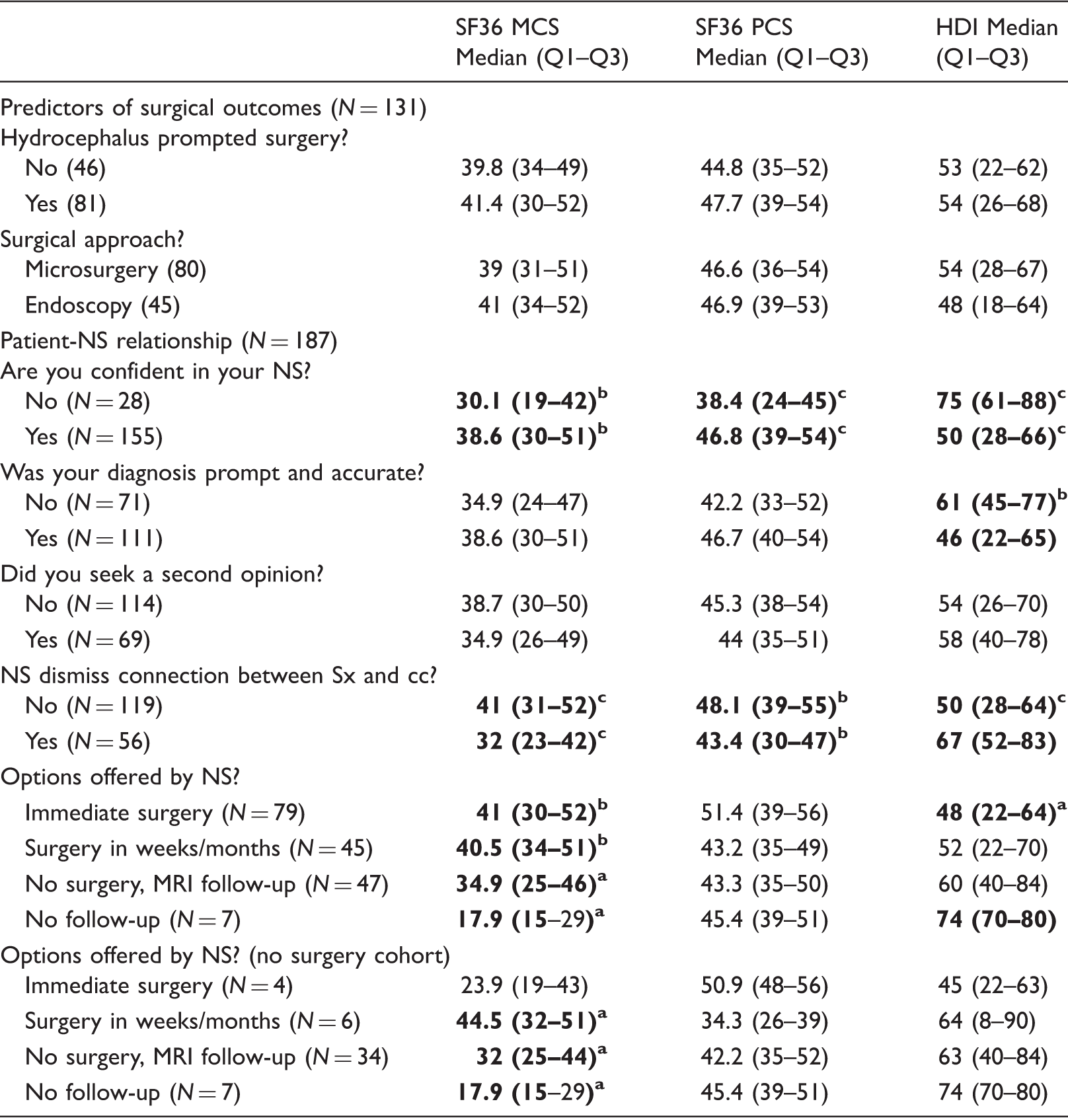
Four patients did not record hydrocephalus status on survey and six patients did not record surgical approach on survey. Comparison of means for binary variables was assessed using a Wilcoxon rank sum test. Comparison of means for variables with more than two categories was assessed using a one-way analysis of variance (ANOVA) with a Bonferroni adjustment. Sx: symptom; cc: colloid cyst; pt: patient; NS: neurosurgeon; MRI: magnetic resonance imaging. HDI: Headache Disability Inventory; PCS: Physical Component Survey; MCS: Mental Component Survey; SF36: Short-Form survey 36. p value: ap < 0.05; bp < 0.01; cp < 0.001.
Endoscopy vs. microsurgery
Ninety-five percent of patients, 125 out of 131, who had a surgical resection were able to report the type of surgical approach that was used. Forty-five patients reported an endoscopic approach (burr hole), while 80 patients reported a microsurgery approach (craniotomy). There were no significant differences between the endoscopic and microsurgery approaches in MCS (41 vs. 39; rank sum p = 0.71), PCS (46.9 vs. 44.6; p = 0.70), and HDI (48 vs. 54; p = 0.43) (Table 5).
Patient relationship with neurosurgeon
To identify components of the patient-neurosurgeon relationship that may predict subjective QoL and headache disability, patients were asked questions about their impression of their neurosurgeon. Eighty-five percent of patients (155/183) reported that they were “confident in their neurosurgeon’s ability to deal with their colloid cyst;” however, 25 patients reported that they were “not confident.” Patients who were not confident had significantly lower QoL and higher headache disability (MCS: p < 0.01; PCS: p < 0.001; HDI: p < 0.001) (Table 5). When asked if their diagnosis was prompt and accurate, 71 patients said “no” and 111 said “yes.” There was no significant difference in QoL between these two groups; however, there was an increase in headache disability score in those who replied that their diagnosis was not prompt and accurate (HDI: p < 0.01) (Table 5). There was no significant difference in QoL and headache disability between patients who asked for a second opinion and those who did not. There was a significant decrease in QoL and an increase in headache disability in patients who reported that their neurosurgeon “dismissed their symptoms as not being connected to their colloid cyst” (MCS: p < 0.001; PCS: p < 0.01; HDI: p < 0.001) (Table 5).
Finally, patients whose neurosurgeon suggested immediate surgery, surgery in a few weeks/months or follow-up with MRI reported to have much higher QoL and lower headache disability compared to patients whose neurosurgeon did not suggest surgery or follow-up (MCS: p < 0.001; PCS: p = 0.03; HDI: p = 0.003) (Table 5). Because the neurosurgeon’s recommendation is intrinsically linked with patients getting surgery or not, we confirmed that these associations remained significant within each surgery group. We found that in the no surgery group, MCS remained significantly lower when the neurosurgeon did not follow up compared to recommending an MRI follow-up or surgery in a few weeks/months (MCS: p < 0.03, one-way ANOVA) (Table 5). In the surgery group, all patients had a follow-up.
Discussion
Prior to designing this study, we recognized that there was a severe lack of patient-centered data for colloid cyst patients. We believe that these patients can provide us a wealth of information concerning their QoL, headaches, and experience with their illness. The first goal of this study was to assess the impact of surgery on QoL and headache disability. We then assessed whether an incidental diagnosis would modify the impact of surgery on QoL and HDI. We also looked at two predictors of surgical outcomes: hydrocephalus and surgical approach. Finally, we assessed the impact of the patient-neurosurgeon relationship on patient QoL and HDI.
Headache in colloid cyst patients
The prevalence of patients with headaches between diagnosis and survey was 90%, including the preoperative and postoperative periods. This is consistent with other reports on colloid cyst patients (2,10,11,18). Given such prevalence, we suspected that headache would contribute significantly to the QoL of these patients. We thought that this would be best captured by the HDI. Indeed, we found a prominent inverse correlation between HDI and the physical/mental components of SF36 (Pearson’s correlation = –0.58 and –0.42, respectively). This suggests that greater emphasis on headache management could have a great impact on the QoL of this patient population.
QoL in colloid cyst patients
To our knowledge, the QoL of the colloid cyst patient population has never been studied. One study reported levels of patient satisfaction with the surgery and recovery (19). Most studies have based their outcomes on physical/symptomatic components of health (3,20–23). However, our study indicates that the MCS are much more affected than the PCS when comparing this patient population to US norms (MCS: median = 37 vs. 50; PCS: median = 45 vs. 50) (Table 3). Parker et al. found that in men with a diagnosis of prostate cancer, anxiety was a strong predictor of MCS but not PCS (24). Furthermore, they found that illness uncertainty was a predictor both for MCS and PCS. In our study, anxiety was the most significant symptomatic difference between the surgery and the no surgery groups. It is also likely that the risk of sudden death in colloid cyst patients contributes significantly to illness uncertainty and anxiety. An alternative hypothesis is that the increased anxiety in the no surgery group is caused by the prospect of surgery.
Surgery vs. no surgery
When comparing baseline characteristics in patients who had surgery to those who did not, the size of the colloid cyst was the only variable that was significantly different (p < 0.001). This is not surprising, since the size of colloid cyst is considered a major indication for surgery (25). The main finding in this study is that the surgery cohort has a higher QoL, as measured by the SF-36 survey. When adjusting for various baseline characteristics with multivariable analysis, we found that both the MCS and PCS were increased in the surgery cohort (Table 4). Surprisingly, surgery seemed to increase the MCS more than the PCS of the SF-36. This suggests that some benefits of surgery may have been overlooked. Interestingly, Buhl et al. looked at seven patients with colloid cysts who underwent neuropsychological testing before and after surgery. They found significant memory and attention deficits in all colloid cyst patients. They also found that five out of seven colloid cyst patients had improved neuropsychological status postoperatively (26).
Incidental diagnosis
Some studies have suggested that an incidental finding of colloid cyst should not result in a resection but rather in observation with serial imaging (8,27) while others have been more in favor of a surgical approach (28,29). Margetis et al. compared surgical outcomes in 20 patients with incidental colloid cysts to 57 symptomatic patients with colloid cysts. They found that there were no significant differences in postoperative morbidity and mortality (28). However, a major question that remains unanswered is whether there are any significant differences in benefits from such a procedure for patients with an incidental diagnosis. Therefore, we decided to include an interaction term (product of “surgery” and “incidental diagnosis”) in our regression models to assess whether an “incidental diagnosis” modifies the impact of surgery on reported QoL. We found that there was no interaction for MCS and HDI. There was, however, a marginal effect modification on surgery and PCS with a negative coefficient. These results suggest that patients with an incidental diagnosis will have similar benefits from surgery in terms of the mental components of QoL and headache disability; however, they may have fewer benefits from surgery in terms of the physical components of QoL.
Hydrocephalus
Colloid cyst patients diagnosed with hydrocephalus are at a significantly higher risk of acute deterioration (8). As a result, there is great interest in assessing their QoL following surgery. We found that hydrocephalus and non-hydrocephalus patients reported comparable postoperative QoL. This finding is consistent with a study from Desai et al. that reports complete resolution of hydrocephalus following colloid cyst resection in all of their patients (10).
Endoscopy vs. microsurgery
Colloid cysts are currently resected via an endoscopic approach or via a microsurgery approach that entails a single-burr hole or a craniotomy, respectively. Recently, the endoscopic approach has drawn increased interest in the neurosurgical field because of decreased morbidity compared to the microsurgery approach (3,22,30–34). However, the endoscopic approach also has lower rates of complete resection and higher recurrence rates (3,18,34,35). In our study, there was no significant difference in reported QoL or headache disability between these two approaches.
Patient-Neurosurgeon relationship
We assessed the impact of the patient-neurosurgeon relationship on patient QoL and HDI. We first found that there is a strong correlation between patient confidence in his or her neurosurgeon and a higher QoL or lower HDI. When the neurosurgeon dismissed a connection between the patient’s symptoms and the colloid cyst, patient QoL and HDI were much worse. Within the no surgery group, if the neurosurgeon did not recommend any form of follow-up there was a significant decrease in MCS.
Limitations
The retrospective nature of our findings and potential recall bias are major limitations. We did not collect pre-operative QoL and HDI scores, which could have given greater insight into the longitudinal progression of these values over time. The response rate for this study was 31%, which could have resulted in a bias for patients who are more functional and with better outcomes. The nature of this study prevented us from retrieving data about non-respondent members of the Colloid Cyst Survival Group. As a result, we were unable to account for selection bias. Although we acknowledge that there is a low response rate, we consider that the population sample (187 patients) is significant given the low incidence of colloid cysts (3.2 colloid cysts per 1,000,000 people) (36). The previously reported literature on colloid cysts includes smaller cohorts ranging from case reports of one or two patients to case series of 39 to 162 patients (4,8,18,27,37). Our survey did not collect any information about the patient relationship with primary care doctors and neurologists, who are also involved in the diagnosis and long-term management of colloid cyst patients. Headaches can often be multifactorial and coexistent primary headache disorders like migraine and tension-type headaches were not explored in this study. We did not have access to the medical records to determine the differences in the recommendations for surgical intervention. Finally, health-related QoL scores were normalized to the US population, but 40% of our patients are from other countries. This, however, should not affect our ability to assess the impact of surgery on QoL. Furthermore, studies have suggested that US-weighted scores could be applied to all non-US data sets for purposes of simplicity and comparability (38). The international and multicenter nature of our study makes it geographically generalizable; however, our patients, being members of the Colloid Cyst Survivor Group, may receive more emotional support than other colloid cyst patients. Survey-based studies have significant limitations as mentioned above and future prospective studies with access to medical records will be needed. However, this study design enabled us to survey QoL and headache disability in a real-world/non-medical environment and in a very rare patient population.
Conclusion
This is the first and largest study on QoL and headache disability in patients with colloid cysts. Despite the limitations of the retrospective nature of this study and potential selection bias, our results suggest that colloid cyst patients who underwent a surgical resection have a better QoL and less headache disability compared with those who did not. We found that patients with an incidental diagnosis of colloid cyst are likely to enjoy similar benefits from surgery. Additionally, preoperative hydrocephalus status and operative approach did not correlate with postoperative QoL or headache disability. Finally, “lack of confidence in neurosurgeon,” “neurosurgeon dismissing symptoms,” and “neurosurgeon not recommending a follow-up” were all associated with worse QoL for colloid cyst patients. Further prospective studies with a larger cohort of patients and baseline QoL and HDI scores are indicated to confirm our findings.
Clinical implications
Surgical resection of a colloid cyst may result in significant improvements in patient headache disability and quality of life. Patients with an incidental diagnosis of colloid cyst may gain similar benefits from surgical resection in headache disability and quality of life. Although surgical approach has been shown to correlate with operative complications and recurrence rate, we did not find significant differences in headache disability or quality of life. A poor patient-surgeon relationship had a strong correlation with worsened headache disability and quality of life.
Footnotes
Acknowledgments
This study was approved by the Johns Hopkins Institutional Review Board Committee: # 36785. Author Jordina Rincon-Torroella is a grant holder of a “Fundació La Caixa” scholarship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.