
Abstract
Background: Measuring quality of life (QOL) is an important means of assessing the impact of headache. The currently used QOL questionnaires are usually geared toward migraine and focus on a limited number of factors, thus they are not necessarily informative in other headache types. We report the psychometric properties of a new questionnaire, the Comprehensive Headache-related Quality of life Questionnaire (CHQQ) that may be more sensitive to the burden of headache.
Patients and methods: A total of 202 patients suffering from migraine (n = 168) or tension-type headache (TTH) (n = 34) completed the CHQQ and SF-36, a generic QOL questionnaire. We assessed the reliability and validity of the CHQQ and its physical, mental and social dimensions.
Results: The questionnaire was easy to administer. Reliability was excellent with Cronbach’s alpha being 0.913 for the whole instrument (0.814–0.832 for its dimensions). The dimensions and total score showed significant correlations with the patients’ headache characteristics (criterion validity), and were also significantly correlated with the SF-36 domains (convergent validity). The total score and dimensions were significantly (p < 0.005) lower in the migraine group than in the TTH group (discriminative validity).
Conclusion: In this study the new headache-specific QOL instrument showed adequate psychometric properties.
Keywords
Introduction
Primary headaches constitute a public health problem, affecting 46% of the adult population globally, causing a significant amount of disability (1) and poor health-related quality of life (QOL) (2). Health-related QOL reflects the patient’s perspective of the way medical conditions and their treatment influence their position in life. Measuring QOL can give a unique insight into the patient’s condition as the doctor’s evaluation of the effect of illness can be markedly different from the patient’s perspective (3). Along with other patient-reported outcomes that measure disability, illness intrusiveness or other consequences of health problems, measuring QOL has become an important means of assessing the burden of disease and the efficacy of therapeutic interventions (4).
QOL is measured by generic or disease-specific questionnaires. Generic ones include questions that represent those aspects of health that are important for the majority of people. Thus, these instruments allow broad comparisons of distinct conditions, can measure the effect of various healthcare interventions and therefore can be useful, among others, in analysing cost-efficiency or planning resource allocation in health economics studies. Generic instruments may, however, be unresponsive to changes in specific conditions (5). There are numerous generic QOL instruments in use, the most widely used being the Short Form Health Survey (SF-36) (6). Disease-specific QOL instruments focus on problems associated with single disease states, allow comparisons of illnesses which share the leading symptoms, and can be helpful in selecting the most appropriate therapy for the patient and monitoring its efficiency. Moreover, they may better reflect the particular impact of a selected condition.
QOL instruments study more domains of QOL. A domain refers to a specific area of behaviour or experience, such as work performance, social functioning, sleep, leisure activities, etc. The domains usually cover the three main dimensions of health-related QOL: physical, mental and social (5), which have their roots in the World Health Organization’s definition of health (7).
Since the 1990s several headache-specific QOL instruments have been developed. These include the MSQ2.1 (Migraine-specific Quality of Life Questionnaire) (8), the MSQOL (Migraine-Specific Quality of Life measure) (9), the 24-hour MQoLQ (24-hour Migraine Quality of Life Questionnaire) (10), and the French QVM (Qualité de Vie et Migraine) (11). In 2003 the 6-item Headache Impact Test (HIT-6) was introduced. HIT-6 is an instrument designed to measure headache impact, a concept that is strongly related to QOL (12). We briefly review these instruments here.
The MSQ2.1 is the current 14-item version of the former 16-item Migraine Specific Questionnaire. It measures three dimensions of headache impact: role-restrictive, role-preventive and emotional function. MSQ2.1 was found to be a reliable and valid means of assessing QOL in migraine and has been formally validated for patients undergoing prophylactic migraine treatment (13). It has also been used in cluster headache (14). Recently, MSQ2.1 was validated for clinical use in episodic and chronic migraine (15) and was found to demonstrate significant differences between these, with chronic migraine sufferers having lower values in all dimensions.
The MSQOL is a 25-item instrument that was found to be a valid and reliable measure for cross-sectional comparisons that encompass a migraine patient’s subjective well-being (9). Further testing of the instrument revealed three dimensions (avoidance, relationships and feelings) and provided evidence for the calculation of a total score (16). Interestingly, another group described a different structure of the MSQOL with four dimensions (physical, psychical, social and life rhythms) in a study of patients with migraine or tension-type headache (TTH) (17) The MSQOL has been successfully used as an outcome measure in prophylactic drug trials for migraine (18).
The MQoLQ was developed to measure the acute changes in QOL in migraineurs during a migraine attack. The questionnaire has 15 items grouped in five domains: work functioning, social functioning, energy, feelings/concerns, and migraine symptoms. In the validation study the domains showed good internal consistency and construct and discriminant validity, and responsiveness to acute migraine attacks. It detected significant changes of QOL during the acute migraine attack. Moderate to strong negative correlations were found between QOL and headache severity, limitations of activity, number of migraine symptoms, and headache duration (10). The MQoLQ was validated and primarily used among migraineurs, but also as an endpoint in drug trials (19), and it was found to be useful in the long-term follow-up of chronic headache patients (20).
QVM is a French migraine-specific QOL instrument, with four domains: psychological, somatic, social repercussion and disturbance generated by the treatment. In the validation study, the reliability assessed by test–retest reproducibility was good (r ≥ 0.70–0.80). In a later study on a nationwide sample, frequency, severity and treatment resistance of headaches, as well as headache-related disability, were significantly correlated with QVM’s total score and subscales; correlation coefficients were not reported (21). QVM was used in many French studies, including acute drug trials in migraine (22) and also in patients with chronic daily headache (21) and TTH (23).
The HIT-6 covers six content categories represented in widely used surveys of headache impact, including social and role functioning, vitality, cognitive functioning and psychological distress. It was developed using an existing item pool of 54 items and from 35 items suggested by clinicians, using advanced methods of item response theory. In a large study, HIT-6 was found to be efficient, reliable and valid for the screening and monitoring of patients with headache (12). Subsequently, it has been extensively used in clinical practice, and applied in studies measuring headache impact and also in drug trials in migraineurs. The HIT-6 has been validated in episodic and chronic migraine using ID-migraine and a headache diary for diagnostic purposes (24). It has also been used in chronic daily headache (25) and TTH (26).
Owing to the availability of these instruments, there is a significant amount of scientific evidence about the negative effect of episodic and chronic migraine, cluster headache (2,14,27), TTH (28) and chronic daily headache (29) on generic and headache-specific QOL. The effects of acute (19,22) and prophylactic (13,18,30) migraine treatment on QOL have also been documented. There are, however, some observations that raise the possibility that currently available instruments do not fully capture patients’ perceptions. Despite the obvious differences in the clinical picture and the patients’ complaints, there were only a few differences between the generic QOL profiles of migraine, cluster headache and TTH (31). The SF-36 profiles of migraine and cluster headache were also very similar, and in the same study, MSQ2.1 did not show any difference between the QOL profiles of cluster headache patients and migraineurs (14). Moreover, a clinically effective therapy is not necessarily reflected by an improvement of the QOL scores of migraineurs (32). Patients may also feel that the instruments do not capture some important areas of their QOL, as was the case of our patients (suffering from cluster headache or migraine) during the above-mentioned trial (14).
Besides these observations there is a methodological caveat when using headache-specific QOL instruments: all the above-described instruments were developed to assess the QOL in migraine. Based on PubMed and Scopus searches, only MSQ2.1 and HIT-6 have been psychometrically validated for chronic migraine, and none have been validated in other headache types.
Taken together, these limitations suggest that an instrument probing several important facets of life and validated in different headache types may provide patients and healthcare providers with more precise information about QOL in headache. In order to test this hypothesis, we have decided to develop a comprehensive headache-specific questionnaire, assessing several aspects of QOL. A preliminary study in migraineurs found that the psychometric properties of this questionnaire were adequate for further testing (33). Three dimensions (physical, mental and social) were constructed based on item content. Exploratory factor analysis with varimax rotation found that a single factor accounted for 47% of the total variance, while a second factor was responsible for 3.7%, and further factors accounted for even smaller amounts of variance: this was interpreted as the basis of calculating a total score (34).
Objective
The aim of the present study was to assess the psychometric properties of the headache-specific questionnaire on a large group of headache patients suffering from migraine and TTH. The main hypotheses were the following:
The questionnaire’s internal consistency will be adequate (Cronbach’s alpha >0.7) in the total sample and both headache types. The individual’s QOL, as indicated by the items, domains and total score, will be negatively correlated with clinical characteristics of their headache. The new questionnaire’s items, domains and total score will be positively correlated with the relevant domains and total score of the SF-36 measure. Patients with TTH will have a better QOL (higher scores on the instrument) than patients suffering from migraine.
Patients and methods
Patients
Consecutive outpatients visiting the headache centre of the Department of Neurology, Semmelweis University, in 2008–2010, who fulfilled the International Headache Society (IHS) criteria (35) for migraine with and without aura (episodic type; ICHD-II codes 1.1 and 1.2) or TTH (either episodic or chronic; ICHD-II codes 2.1–2.3) took part in the study. We excluded patients suffering from the rare adult migraine subtypes (hemiplegic migraine, basilar-type migraine, retinal migraine and complications of migraine (ICHD-II codes 1.2.4–1.2.6, 1.3–1.5). According to the IHS criteria, patients meeting one of the sets of criteria for probable TTH (2.4) may also meet the criteria for one of the subforms of probable migraine (1.6), therefore we also excluded patients with the diagnosis of probable migraine and probable TTH in order to minimize the chance of misdiagnosing the patients. Patients whose analgesic consumption reached the criteria of analgesic abuse (36) were also excluded, as were patients who also had concomitant chronic pain syndromes, untreated hypertension, and untreated or severe kidney or liver disease. Other concomitant treated disorders were not excluding criteria, but their possible effect on QOL was not taken into account in the statistical analysis. All patients had headache as the main complaint at the time of the study.
Methods
Development of the new questionnaire
The development of the questionnaire consisted of three major steps: relevant item identification, formation and psychometric testing of a draft version, and the development of the final version. First one of the authors (CE) conducted open interviews with 25 persons suffering from the most important primary headache types (10 migraine (M), 10 TTH and 5 cluster headache (CH) patients). The questions for these interviews were based on the experience of five clinicians and literature reviews of QOL in headaches and other pain conditions. A question was considered a potential item if at least two clinicians and two patients from each diagnostic group felt the respective issue was important. Twelve of the 37 original questions were found redundant or insignificant and therefore removed, resulting in a 25-item draft version.
In a second step, 11 migraineurs from a larger group studied for the effect of migraine (37) were asked to complete the draft version and were then interviewed about it. These interviews were used to determine whether each individual understood the items, felt them meaningful and whether they felt the answer categories were sufficient. Minor changes of content and format were applied accordingly.
Third, the 25-item questionnaire was tested in a group of 117 migraineurs (33) and quality criteria for item selection (9) applied. There was no ceiling effect in the sample. One item asking about the influence of headache on parental responsibilities (‘How much do your headaches interfere with your role as a parent?’) had by far the biggest proportion of missing answers (31% of the sample; mostly patients with grown-up children or no children) and therefore was not included in the final version. An item about prophylactic medication use (‘How often have you used prophylactic treatment for your headaches?’) had a very low (0.214) item-total correlation: analysis of the clinical data revealed that beside those who regularly took a prophylactic medicine, a significant part of the study population considered the early administration of acute medications as ‘prophylactic’ treatment. This item was also problematic because taking a migraine prophylactic is the joint decision of the patient and the physician and therefore it is less likely to reflect the patient’s QOL. Therefore this item was also omitted from the final version of the questionnaire. The reliability and validity assessments confirmed that the resulting 23-item questionnaire was adequate for further testing.
Description of the instruments used in the study
The 23-item QOL questionnaire, hereafter referred to as the Comprehensive Headache-related QOL Questionnaire (CHQQ), examines the impact of headache on QOL in detail. The questions cover the 2 weeks before the data recording. All questions have five possible answers (5-point Likert scale), ranging from the absolute absence of restriction to maximal restriction. After scoring, the values are transformed to a 0–100 point scale, the absence of restriction being equal to 100 points and the full restriction to 0 points (6). Total score and the three dimensions (physical, mental and social) are calculated; they are the mean values of the relevant transformed item scores (the item scores are not weighted).
Generic QOL was measured with the validated Hungarian version of the SF-36 questionnaire (38). The SF-36 is one of the most frequently used generic QOL instruments. It examines eight QOL domains: four domains represent physical (physical functioning, role-physical, bodily pain, general health) and four mental health concepts (vitality, social functioning, role-emotional, mental health) (6). Widely accepted as it is, the SF-36 is far from examining all notable aspects of QOL. Among other aspects, the SF-36 does not collect data about sleep and its quality, cognitive features, leisure activities, sexual life, self-confidence, worries, and the quality of interpersonal communication.
Data recording
The patients all completed the validated Hungarian version of the SF-36 and the CHQQ in the Headache Unit, after their outpatient visit; the questionnaires were administered by the headache specialist seeing outpatients on the given day. The questionnaires were filled in on the spot and given back to the staff. Missing data were not complemented. The patient’s headache characteristics and other clinical data were recorded during their clinical interview. Headache severity was assessed by the patient (visual analogue scale (VAS); 0–100 mm) and also by the specialist during the clinical interview (IHS rating scale, 0 = pain free, 1 = mild, 2 = moderate, 3 = severe). Headache diagnoses were made by the same headache specialists during the outpatient visit, using the IHS criteria. Depression was not formally tested during the visit. As this was a validation study, the data were not used in the evaluation of the patient’s functional status, disease severity or therapeutic needs.
Statistical methods
The validation of a questionnaire requires testing its reliability and validity. Reliability is the degree to which a test consistently measures what it aims to measure. The methods of assessing reliability include the test–retest method, the use of two alternative questionnaires (the equivalence of which requires prior statistical evaluation) or measuring the internal consistency of the instrument by calculating the split-half reliability, or Cronbach’s alpha. To assess the reliability of our questionnaire, we calculated the Cronbach’s alpha for the whole instrument and its dimensions.
Validity refers to the degree to which an instrument can accurately assess the specific concept that the research is attempting to measure (5). We used several methods to assess the validity of the instrument. First we examined the correlation of the patient’s headache characteristics with the questionnaire’s items, dimensions and total score (criterion validity). We then examined the correlation of the individual items, the three dimensions and the total score with the domains of the SF-36 measure, a means of assessing convergent validity. In these analyses the degree of correlation was measured by calculating Spearman’s rank correlation coefficient. We also assessed discriminative (known groups) validity, by comparing the results of the instrument in the two diagnostic groups, M and TTH, using Mann–Whitney tests.
In the preliminary validation study items were grouped in the three classical dimensions of QOL instruments (physical, mental and social) according to their content. In order to assess the structure of the instrument we performed an analysis of item-dimension correlations using Spearman’s rank correlation coefficients.
Statistics were calculated using Statistica 8.0 software. The level of significance was set to p < 0.05.
The study was approved by the Regional and Institutional Committee of Science and Research Ethics of Semmelweis University.
Results
Observations about completing the questionnaire
The questionnaires were administered to a total of 217 patients. On average, it took less than 20 minutes to complete both of the questionnaires. Filling in the questionnaire did not present any difficulty, as reported by the patients. The majority of the patients answered all questions. Of CHQQ’s 23 questions, 13 had no missing answers. Fifteen participants did not answer the question about the influence of their headaches on their sex life. For the remaining nine questions, the rate of missing answers was very low (1 to 3 per question). All questions were completely answered by 202 patients (93% of the 217 patients). As Statistica excludes subjects with missing data from reliability and validity analyses, these were calculated taking the 202 patients into account.
Patient characteristics
Among the 202 patients we studied 169 were females and 33 were male. The mean age was 35.1 years, (SD 11.53; range 18–68). All patients were Caucasian. One hundred and forty-one patients were in paid employment (70%), 20 were students (10%), 10 were on maternity leave (5%), 9 were retired (4.5%) and 3 unemployed (1.5%); 19 preferred not to answer the question about employment status.
One hundred and sixty-eight patients (83.2%) were migraineurs and 34 patients (16.8%) had TTH (11 episodic and 23 chronic). Patients with chronic TTH had a significantly higher attack frequency (mean 33.5, SD 13.5 vs. mean 6.5, SD 4.0, p < 0.001) and more headache days (mean 27.7, SD 5.07 vs. mean 7.61, SD 4.33, p < 0.001) but smaller minimum (mean 1.97, SD 1.56 vs. mean 4.91, SD 6.19 hours, p = 0.027) and maximum (mean 9.4, SD 6.67 vs. mean 33.71, SD 24.0 hours, p < 0.001) lengths of treated attack than patients with episodic TTH. Other headache characteristics were not significantly different in the chronic and episodic TTH groups. The male:female ratio was non-significantly higher in the chronic group (10 males and 13 females vs. 2 males and 9 females, p = 0.252, Fisher’s exact test).
Patient characteristics.

Data are presented as mean ± SD. All: all patients; M: migraine group; TTH: tension-type headache group; IHS: International Headache Society; VAS: visual analogue scale.
Reliability
The reliability of the questionnaire and its main dimensions: Cronbach’s alpha values.

TTH: tension-type headache.
Validity
Criterion validity
Criterion validity: the correlations between the items, dimensions and total score of the instrument with the clinical characteristics. For the sake of brevity only the whole group’s results are presented about the correlation of the individual items and headache characteristics.


All: all patients; M: migraine subgroup; T: tension-type headache subgroup; marked correlations (bold and italic) are significant (p < 0.05).
In the whole sample, the physical dimension of the instrument was significantly correlated with all clinical characteristics. The mental dimension was significantly correlated with six of the nine clinical characteristics (the exceptions being attack frequency, headache days per month and maximum length of attacks). The social dimension was correlated with eight of the nine clinical characteristics; age did not show a significant correlation with this dimension.
In the migraine subgroup most correlations were also significant. Neither dimension was correlated with the number of headache days per month, the mental dimension was not correlated with attack frequency and the maximum length of attacks, and the social dimension was not correlated with age. In the TTH group the questionnaire’s physical and social dimensions were negatively correlated with headache severity, whereas the mental dimension showed no significant correlation with the clinical characteristics.
In the whole sample the total score of the instrument correlated significantly with seven of the nine headache characteristics; there was no significant correlation with age and the number of headache days per month. In the subgroup of migraineurs the total score also showed significant correlations with most (7/9) clinical data, the exceptions being attack frequency and days with headache in the last month. There were no significant correlations between the clinical data and the total score in the subgroup of patients with TTH.
Convergent validity
Convergent validity: The correlation of the questionnaire’s individual items, dimensions and total score with the SF-36 instrument. Marked correlations (bold and italic) are statistically significant (p < 0.05). For the sake of brevity only the whole group’s results are presented about the correlation of the individual items and SF-36 domains.
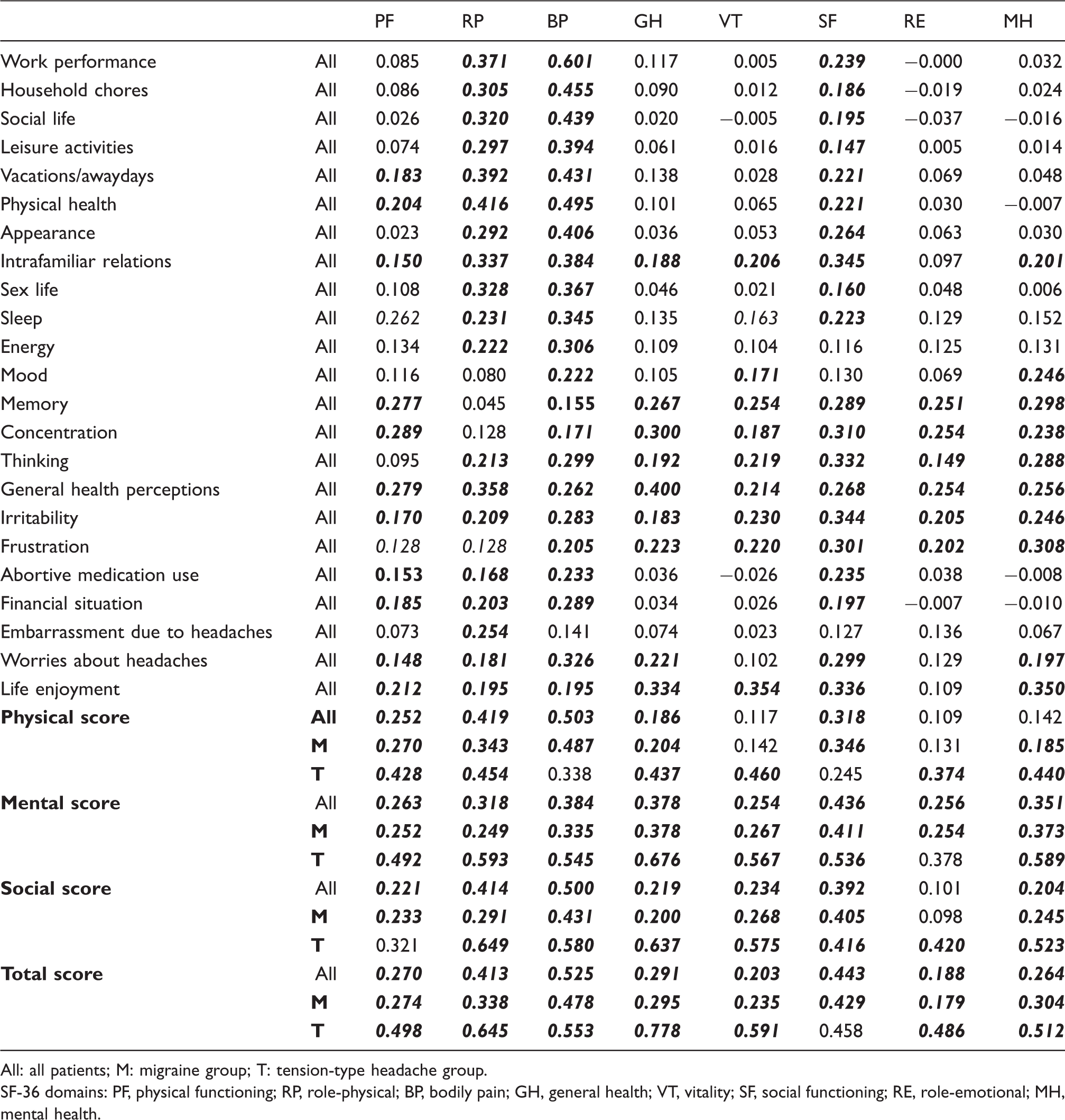
All: all patients; M: migraine group; T: tension-type headache group.
SF-36 domains: PF, physical functioning; RP, role-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role-emotional; MH, mental health.
The physical dimension of the new instrument showed significant correlations with all ‘physical’ domains of the SF-36 in the total sample and also in the M and TTH groups, except for the correlation with SF-36’s bodily pain domain in the TTH group. The mental dimension had significant correlations with all SF-36 domains, with the exception of the correlation with the role-emotional domain in TTH patients. The social dimension had significant correlations with the majority of SF-36 domains, except for the role-emotional SF-36 domain, which was significantly correlated with it only in the TTH group, and the physical functioning SF-36 domain, which was not significantly correlated with the social dimension in TTH sufferers.
The total score of the instrument correlated significantly with all SF-36 domains in the whole sample and in the migraine group; the total scores in the TTH group did not correlate with the social functioning domain of SF-36, but showed significant correlations with all other SF-36 domains.
Discriminative validity
Discriminative validity: item, dimension and total scores (mean ± SD) of the migraine group versus the tension-type headache group.

Marked differences (bold and italic) are significant (p < 0.05, Mann–Whitney tests). Higher scores reflect a better QOL. M: migraine group; TTH: tension-type headache group.
Within the TTH group, there was no significant difference in the CHQQ scores (items, dimensions and total score) of episodic and chronic patients, apart from work performance (p = 0.014) and physical health (p = 0.016), which were more severely affected in chronic TTH.
Dimension structure of the questionnaire
In order to examine whether the individual items were mathematically related to the hypothesized dimensions of the instrument, we performed an analysis of item–dimension correlations on the sample. Spearman’s rank order correlations were significant for all items and all dimensions. With the exception of the Energy item (which showed the highest correlation with the Physical dimension), all the items showed the highest correlation with their intended dimensions (these data are not shown in the tables).
Observations of the SF-36 measure
In order to compare the performance of the new questionnaire and the SF-36, we calculated the correlations between the SF-36 domains and the clinical characteristics. In general, significant correlations were rare and of low to moderate strength. In the whole sample attack frequency was negatively correlated with role-physical, vitality, role-emotional and mental health domains, and headache severity was negatively correlated with the role-physical and bodily pain domains. In the migraine group attack frequency was not correlated with any SF-36 domain, and headache severity was negatively correlated with the role-physical and bodily pain domains. In the TTH group attack frequency was negatively correlated with the role-physical and bodily pain domains, and headache severity with the bodily pain domain (these data are not shown in the tables).
Discriminative validity of the SF-36 questionnaire. SF-36 scores of the migraine and TTH groups (mean ± SD)

M: migraine group; TTH: tension-type headache group.
SF-36 domains: PF, physical functioning; RP, role-physical; BP, bodily pain; GH, general health; VT, vitality; SF, social functioning; RE, role-emotional; MH, mental health.
Discussion
We evaluated the psychometric properties of the Comprehensive Headache-related QOL Questionnaire (CHQQ), a new headache-specific QOL instrument in patients suffering from migraine or TTH headache. The questionnaire was easy to administer. The internal consistency of the questionnaire was excellent in the whole sample and also in the diagnostic subgroups. Tests of criterion and convergent validity were also adequate. The questionnaire was able to detect significant differences between the impact of migraine and TTH. The dimension structure of the instrument was confirmed. Thus, CHQQ seems to be a reliable and valid means of measuring the impact of headache on the individual’s QOL.
The study population consisted of patients with episodic migraine and TTH. Patients with episodic and chronic TTH had very similar clinical characteristics (apart from attack frequency and number of days with headache) and similar QOL profiles (no significant differences were found in 21/23 items, 3/3 dimensions and the total score), and therefore were treated as a single group. The reason for this similarity may be the fact that patients were recruited at a tertiary centre and patients with infrequent TTH or those whose headache did not cause a certain amount of impairment were not referred to this centre for evaluation.
The study population may have been larger if patients with probable migraine and probable TTH had been included. We decided not to include these patients to avoid diagnostic errors, as the IHS classification foresees a diagnostic overlap between these two headache types. We also aimed to define clearly distinguishable diagnostic groups because we felt that the assessment of discriminative validity could have been compromised by including the respective ‘probable’ cases. On the other hand, as the present study confirmed the questionnaire’s ability to discriminate the effect of migraine and TTH, it would be interesting to investigate whether there is any meaningful difference between the QOL profiles of patients with ‘probable’ and ‘definitive’ migraine or other forms of headache.
The length and ease of use of a questionnaire are important aspects of its usability (39) and questionnaire length can have a threshold effect on response rate (40). In our study the questionnaire did not present any difficulty for the patients and 93% filled in all questions. The question about the effect of headache on sex life was the most frequently unanswered one (7% of the patients), much lower than the 17% missing answers for a similar question in a French QOL study (21). The other questions were answered by more than 98% of the participants; equally high answer rates had been observed in previous studies of QOL in headache (9,21). The high response rate indicates that the length of this questionnaire will probably not be a significant limiting aspect of its clinical use. While shorter QOL instruments can clearly have an important role in everyday practice (41), longer instruments such as the CHQQ may present a more detailed QOL profile, which could be especially useful in the areas of clinical and pharmacoeconomic research and/or healthcare planning.
In assessing the reliability of a questionnaire, the repeated application of the same questionnaire (test–retest analysis) is an alternative to measuring internal consistency. Test–retest analysis usually requires a 4-week period between the two test sessions in order to avoid recall bias. During this period the patient’s therapy should be unchanged. As the majority of our patients clearly needed a change in their acute medications (and a significant portion also needed prophylactic therapy), this method would have been ethically incorrect and so was not applied in this study. Internal consistency is generally considered adequate if Cronbach’s alpha exceeds 0.7, and considered excellent with values in excess of 0.9; if an instrument is to be used in the clinical setting, rather than for the comparison of groups only, an alpha exceeding 0.9 is the minimum requirement (42). In this respect CHQQ seems to be adequate for use as a follow-up tool in individual patients, but we underline that formal clinical testing should precede its use for this purpose. On the other hand, CHQQ’s reliability is comparable to that of MSQ2.1 and quite noticeably better than the reliability of the MSQ, the dimensions of which had internal consistency values between 0.70 and 0.85 (8).
A high-quality QOL instrument is required to demonstrate content validity, criterion and construct validity (43). Content validity expresses the degree to which the underlying construct (QOL) is comprehensively sampled by the instrument’s items (5). Unlike other forms of validity, content validity cannot be formally tested, but is assured by (and can be judged by) the methods followed at the instrument’s development process. We followed the recommendations outlined in (5) and (43) during the development phase of CHQQ. Consequentially, the items included in the final version were the ones that were meaningful both for the patients and the clinicians involved. The small number of missing responses may also reflect that the patients felt the questions covered important aspects of their condition – another aspect of content validity. It is therefore reasonable to suggest that the instrument’s content validity is adequate.
The instrument’s validity was formally assessed by measuring its criterion, convergent and discriminative validity. Criterion validity is usually defined as the extent to which scores of an instrument are related to a criterion measure, i.e. a measure of the target construct that is widely accepted as a valid representative of that construct (44). The criterion measure can be a previously validated instrument measuring a similar construct, or a clinical variable that is conceptually related to the construct that the new instrument purports to measure. In headache research, the clinical characteristics of the individual’s headaches are frequently used as criterion measures. In line with the present study, most QOL instruments had low to moderate correlations with the clinical data. During the validation of the MSQ2.1 measure, self-reported frequency and severity of headaches, duration of the attacks, and the time since the last severe headache were used to test for criterion validity (8). These showed significant but moderate correlations with the MSQ2.1 dimensions and total score. The validation study of the MQoLQ-24 (10), an instrument designed for assessing the acute changes in QOL during a migraine attack, found that most correlations between the instrument’s domains and clinical data were moderate: the strongest correlations were between the work domain of the instrument and limitation of activity (r = −0.30 to −0.51); the weakest correlations were seen with the concerns/feeling domain, but even there, the strongest correlation was with activity limitation (r = −0.19 to −0.41). In the validation study of the French QVM instrument, the frequency, severity, and treatment resistance of headaches, as well as headache-related disability, were significantly correlated with QVM’s total score and subscales; correlation coefficients were not reported (21). During the validation study of the MSQOL correlations with clinical variables were not calculated; instead, groups were created according to the severity of clinical symptoms and ANOVAs of MSQOL scores calculated: increased disease severity was associated with worse QOL (9).
In the present study more severe external measures of headache were related to a worse QOL. The strength of the correlations we observed (weak to moderate) was comparable to those found in the above-mentioned studies. The strength of correlations, and the fact that the items, dimensions and total score of the instrument did not correlate significantly with all clinical data, are not surprising: the symptoms of a disease do not invariably correlate with QOL scores (45). This is partly explained by the fact that the items in a QOL instrument can be divided into two main types: causal indicators and effect indicators. Studies of the relationship between symptoms and QOL indicate that while some symptoms, such as obstipation, vomiting or hemiparesis, are almost always evident before, and have a direct influence on the deterioration of QOL (causal indicators), other symptoms including pain, anxiety or depression probably have a bidirectional relationship with QOL (effect indicators) (46). It is also important to note that different symptoms or aspects of their conditions can have differing importance for primary headache patients. This is exemplified by studies of the determinants of patient satisfaction with migraine treatment, with fast and complete headache relief being described by most migraineurs as their main preference, and freedom from associated symptoms being important for a smaller number of patients (47). The difference in the frequency of accompanying symptoms within the study populations (48) may also influence the correlations between clinical data and QOL scores. Finally, it must be borne in mind that, theoretically, symptom scores and QOL instruments measure two fundamentally different constructs, and the correlations we found support this notion.
While the CHQQ scores of migraineurs showed significant correlations with most clinical data, the scores of TTH patients were not significantly correlated with the clinical characteristics, apart from moderate correlations of headache severity and the physical and social dimensions. This may be explained in part by the fact that this group consisted of a fewer number of patients, and was itself heterogeneous as regards the headache frequency of the individuals. On the other hand, areas conceptually related to QOL, such as the ability to study, had been found to be more severely affected by migraine than by TTH, even after correction for pain intensity (49). Moreover, in the present study significant correlations between the TTH group’s clinical characteristics and SF-36 domains were also very rare: previous studies about QOL in TTH had similar results. In a sample of 25 chronic TTH patients, only four (bodily pain, vitality, social functioning and mental health) of the eight SF-36 domains were significantly correlated with headache frequency, and only one (social functioning) with headache intensity (50). In a German study, the SF-36 physical composite score (PCS) of TTH sufferers was significantly correlated with days with disability and days with analgesic use, but not with headache days/hours, days with severe headache and headache score. In the same study the PCS of migraineurs was significantly correlated with all clinical variables. Interestingly, the mental health composite score was not correlated with the clinical characteristics in either of the diagnostic groups (51). These studies and our results seem to indicate that the perceived effect of TTH on QOL is largely independent of the clinical characteristics of headache.
Convergent validity was assessed by calculating the correlations between CHQQ and the SF-36 generic QOL instrument. The total score of our instrument correlated significantly with all SF-36 dimensions in the whole sample and the diagnostic subgroups, with the exception of the total score in TTH that was not correlated with SF-36’s social functioning domain. CHQQ’s three dimensions had significant correlations with the majority of SF-36’s domains. Most correlations were of moderate strength (0.3 to 0.5) in the whole sample and migraine group, while there was a high number of strong (>0.5) correlations between CHQQ scores and SF-36 domains in the TTH group. Correlation coefficients were higher in the TTH group (0.374–0.778) than in the migraine group (0.179–0.487). The strength of correlations was again similar to those found in previous validation studies. In the MSQOL validation study convergent validity was measured by calculating the correlations of MSQOL with the SF-36 domains: mostly moderate correlations were found with the exception of a strong (0.53) correlation with the mental health domain (9). The validation study of the MSQ2.1 reported low-to-modest correlations between MSQ dimensions and the two component scores of the SF-36 (52).
The fact that most correlations were moderate may be explained by three factors. First, SF-36 gathers data about the 4 preceding weeks, while the CHQQ asks questions about the last 2 weeks. Second, there are important differences between the items in the two instruments. The CHQQ asks questions about sleep, intrafamiliar relations, sex life and leisure activities, while these are not included in the SF-36. Furthermore, it is important to stress that the CHQQ explicitly asks about the way headaches influence the various areas, so limitations caused by other conditions were probably not taken into account by the patients, whereas SF-36, as a generic QOL measure, gathers information about the effect of one’s health in general (including the headaches) on QOL. The same three factors may also explain the lack of significant correlation between SF-36’s social functioning domain and CHQQ’s total score in TTH patients.
Confronting the diagnostic subgroups’ headache-specific QOL (discriminative or known group validity) lent further support to the validity of the instrument. It is important to stress that, as we had expected, migraine patients had numerically lower scores (worse QOL) for all items, dimensions and the total score, and that the difference was significant in most (with the exception of seven items). It therefore seems that the CHQQ is able to disclose the differential effect of headache types on QOL. In this regard it is worth noting that in the present study the SF-36 questionnaire found a significantly different QOL between migraine and TTH only in four of its eight dimensions, and in two of them TTH sufferers had worse QOL, which is not consistent with the widespread notion of migraine being a more severe condition.
Convergent and discriminative validity are two subcategories of construct validity. Construct validity refers to an agreement between a theoretical concept (‘construct’) and the instrument designed for measuring it. The necessity of examining the construct validity of the instruments stems from the fact that an instrument can only examine the observable aspects of the construct. As the new instrument demonstrated adequate convergent and discriminative validity, we can assume that it is in agreement with the construct, i.e. QOL.
We started developing the CHQQ with the intention of producing an instrument that examines the QOL of headache patients in detail. We therefore tried to include a set of items covering several aspects of life. It was expected that the underlying factor structure would be complex. In the preliminary study we grouped the items according to the classical dimension structure used in QOL research (physical, mental and social), relying on the content of the items. This is considered a valid approach. Clinically useful scales are sometimes organized into subscales according to rational (rather than mathematical) principles and the two do not necessarily coincide. An example is the Headache Disability Inventory (HDI) (53), where the authors rationally organized items into emotional and functional subscales; in a later study by Holroyd et al. the factor analysis of HDI items revealed that all items loaded on a single factor (54). Different studies may find a different underlying structure within the same instrument, as exemplified by the MSQOL, which was found to have three dimensions (avoidance, relationships and feelings) in an American study (16), and four dimensions (affective, social, energetic and life rhythms) in a Hungarian one (17).
In the present study the analysis of the item–dimension correlations confirmed the hypothesized structure of the instrument.
An obvious issue with our study is the method of patient selection. As patients presenting at a tertiary centre were involved in this study, patients suffering from more severe headaches may have been over-represented in the sample. In fact, patients with more severe limitations may be more motivated to seek medical help in a specialized headache centre. An indirect proof of this possibility may be the fact that migraineurs outnumbered TTH sufferers in this study, in spite of TTH being much more prevalent in the general population.
A further limitation of our study is that most of the patients had migraine. This was due to the fact that we had chosen to enrol all consecutive outpatients who fulfilled the diagnostic criteria of migraine or TTH. Although the TTH group was much smaller, the reliability and validity measurements in this subgroup also showed that the psychometric properties of the instrument were adequate. This was further underscored by the fact that the instrument showed significant differences between the migraine and TTH groups, with TTH patients having better QOL. In this respect it is also worth noting that there were significant differences in the clinical characteristics of headache in the two groups, with migraineurs reporting higher values of disease duration, length of attacks (average, minimum and maximum), and severity of the attacks. Intriguingly, those clinical characteristics that were higher in the TTH group (signifying bigger disease load), i.e. attack frequency and number of days with headache, were the ones that showed fewer correlations with CHQQ’s items, dimensions and total score. A more precise assessment of the instrument’s usability requires samples drawn from the general population.
Comparing the new instrument with previously developed headache-specific measures could have added further evidence about the validity of the instrument and may have yielded important data about its usability. However, due to a lack of validated Hungarian translations of headache-specific QOL instruments, this approach was not possible (the validation study of the Hungarian version of the MSQOL was only published in 2011 (17)). Although the HIT-6 has been validated in Hungarian (55), due to the small sample size (only 35 Hungarian migraineurs diagnosed by their primary care physician were studied) and to the fact that, in a strict sense, HIT-6 is not a QOL instrument, we decided not to use it.
Regardless of these limitations, the present study provides sufficient evidence that the new QOL scale is a reliable and valid instrument to measure QOL in episodic migraine and TTH. Although previous headache-specific instruments are used in headaches other than migraine, only HIT6 and MQoLQ have been formally validated in chronic migraine, and, apart from our new questionnaire, we do not know of any instrument having been validated for TTH. The present study paves the way for using the new instrument in these headache types. We hypothesize that it may be useful in measuring QOL in headaches other than migraine, and may offer a more detailed view of the patient’s QOL, thereby making our understanding of the burden of headache more complete. It might also be useful in the more detailed evaluation of headache treatment (acute or prophylactic), and, assessing its correlations with instruments measuring patient satisfaction, might offer insights about the aspects of headache-related QOL that are meaningful for patients. Further evaluation of the instrument in migraine and TTH, as well as validation studies in chronic migraine, cluster headache and medication overuse headache, are needed to confirm these hypotheses.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.