
Abstract
Background
Burning mouth syndrome (BMS) is a chronic medical condition characterised by hot, painful sensations in the lips, oral mucosa, and/or tongue mucosa. On examination, these appear healthy, and organic causes for the pain cannot be found. Several studies have yielded scant evidence of the involvement of psychological and/or psychopathological factors, and several have outlined a model for the classification of BMS.
Aim
This review aims to provide a systematic review of research examining the psychological, psychiatric, and/or personality factors linked to BMS.
Findings
Fourteen controlled studies conducted between 2000 and the present were selected based on stringent inclusion/exclusion criteria. All studies but one reported at least some evidence for the involvement of psychological factors in BMS. Anxiety and depression were the most common and the most frequently studied psychopathological disorders among BMS patients.
Discussion and conclusion
Anxiety and depression play critical roles in this condition. Evidence on the role of personality characteristics of BMS patients has also been produced by a few studies. Further studies on the role of specific psychological factors in BMS are warranted, but the importance of a multidisciplinary approach (medical and psychological) to BMS is no matter of discussion.
Introduction
Diagnostic criteria for burning mouth syndrome (International Classification of Headache Disorders, 3rd edition beta (ICHD-3) version).

The diagnosis of BMS is often made by exclusion, and the diagnostic process should include an interview to analyse the quality and the quantity of pain; a clinical examination, including an analysis of the mucous membranes and possible local and systemic causes; measurement of salivary flow and the taste function; microbiological swabs to confirm suspicions of bacterial (or viral or fungal) involvement; a patch test for allergens; a gastric reflux study; blood tests to assess nutritional status; hormone tests; and examinations to rule out autoimmune disease (4). Epidemiological data on BMS are generally poor, due in part to a lack of strict adherence to diagnostic criteria (5), and prevalence estimates range from 0.6% to 15% (4,6).
BMS affects more women than men, with a ratio of 7:2.5; it is more common in menopausal women, and its prevalence increases with age (7,8). A recent study on the general population found a mean age at diagnosis of 59.4 years (range: 25–90 years), with the highest prevalence in women aged 70–79 years (9).
The aetiology of BMS remains unknown, but a variety of hypotheses have been proposed (10,11). Its treatment is also a focus of debate, and there is scant research to provide guidance to those treating patients with this condition (12). BMS has a negative impact on health-related quality of life (13,14). Indeed, a recent study (3) found a worsening in the quality of sleep and life in patients with BMS compared to controls, probably because of pain. Few patients (approximately 3%) experience a complete and spontaneous remission of symptoms (15).
The role of psychological factors in BMS has been the focus of several studies and indirectly suggested by different proposals of classification of BMS.
Scala et al. (15) classified BMS into two forms: primary (essential/idiopathic), which is characterised by an unknown local or systemic cause and the involvement of central and peripheral neuropathic pathways; and secondary, which is caused by local systemic or psychological factors.
Lamey (16) identified three types of BMS: type I, which is characterised by a burning sensation in the mouth and tongue during the day and is not linked to psychiatric disorders; type II, which is characterised by constant pain during the day and is linked to psychiatric disorders, particularly chronic anxiety; and type III, which is characterised by intermittent pain with atypical localisation, such as in the area of the cheek mucous membrane or tongue root, associated contact stomatitis, reactions to food additives, and the involvement of unspecified psychiatric disorders.
Cocolescu et al. (8) proposed five categories of possible causative factors for BMS: local, systemic, psychological, neurological and idiopathic.
During the last 15 years, at least one review per year has been published on various aspects of BMS, but only one examined the psychological characteristics of patients with BMS (18). To the best of our knowledge, no systematic review has been performed on psychological contributors to BMS. Yet it is imperative to clarify the role of psychological factors in BMS given the impact of and the poor outcomes associated with this condition as well as the potential psychological sequelae of receiving a diagnosis sine causa. Patients with BMS suffer from a rare and painful condition that is often difficult to explain to others and from which it is often difficult to find relief. Rarity and lack of awareness of this condition among health care professionals may also contribute to psychological impact. Indeed, BMS is characterised by chronic pain and thus presents the well-known challenges related to aetiopathogenesis and treatment that accompany efforts to understand and ameliorate the multiplicity of factors that contribute to such pain.
The primary aim of this systematic review was to calculate the pooled estimates of the odds ratios (ORs) for the associations of psychological disorders with the presence (cases) vs the absence (controls) of BMS. We tested the null hypothesis that there would no difference between cases and controls with regard to the frequency of psychological disorders.
Methods
Search strategy
To include the broadest range of relevant literature, we performed an electronic literature search of three major databases in the field of medical and psychological sciences: PsychInfo, PubMed and Scopus. The electronic bibliographic search was conducted in May 2015.
Flow diagram of literature search and selection of publications.
The search was limited to English-language journal articles and was adapted for each database as necessary. We limited our search to the period from 2000 to the present to focus on more contemporary psychological models, theories and assessments. The keywords were ‘burning mouth syndrome’ OR ‘stomatopyrosis’ OR ‘stomatodynia’ OR ‘glossalgia’ OR ‘glossopyrosis’ AND ‘psychological’ OR ‘psychiatric’ OR ‘cognition’ OR ‘anxiety’ OR ‘depression’ OR ‘mood disorder’ OR ‘somatoform’ OR ‘somatisation’ OR ‘psychogenic’ OR ‘temperament’ OR ‘psychometric’ OR ‘personality’. Moreover, we performed an additional analysis of each reference list in each selected paper to ensure that all significant papers were included in the review (Figure 1).
Selection criteria and data extraction
The following inclusion criteria were employed:
The use of an analytical study design as defined by Grimes and Schulz (19) (i.e. an observational study with a comparison or control group); Diagnosis of BMS based on current criteria; The use of standardised and validated instruments to assess psychological factors; Written in the English language. Case reports, reviews and studies reported in letters to the editor; Studies with intra-group controls (e.g. premenopausal or postmenopausal BMS); Studies with a single control group enrolled in a clinical population (e.g. only atypical facial pain control group); Studies with controls drawn from research on the validation of psychometric test(s); Studies that did not specify the selection criteria for the control group(s).
The following kinds of research were excluded:
Data extraction
Study selection was performed by two independent reviewers (FG and EV) who assessed the relevance of the studies’ questions and objectives. This first round of selection was based on the title, abstract and keywords of each study. If the reviewers did not reach a consensus or the abstracts did not contain sufficient information, the full text was reviewed.
In the second phase of the selection process, which relied on the full-text reports, we tested whether the studies met the inclusion criteria. Discrepancies between reviewers were resolved by a process of discussion/consensus-building moderated by a third reviewer (GL) (20). When the full text was not retrievable, the study was excluded.
A standardised data extraction form was prepared, and data were independently extracted by two of the authors (FG and EV) and inserted in a study database. The form included the following information: title, year of publication, numbers of patients and healthy controls, gender ratio, criteria used to classify BMS, study design, tools used in the psychometric assessment, significant and non-significant findings, and notes and/or comments on the study findings and/or design.
Risk of bias
To assess the risk of bias of the included studies, we adopted a method previously employed in systematic reviews of observational studies (21,22). In brief, two reviewers (GL and FG) independently extracted relevant information and data from all eligible reports that met the inclusion criteria, and the following quality criteria were adopted to assess risk of bias:
Cohort studies
1) Appropriateness of the control group: with the exception of BMS status, participants in the control group must not differ significantly from those in the study group (matched for gender and age, individuals in the control group must have been selected from the study base); 2) a follow-up period of at least five years; and 3) a prospective design (i.e. data and samples must have been collected specifically for the study).
Case-control and cross-sectional studies
1) Characteristics of the study group: consecutive, unselected patients with BMS; 2) appropriateness of the control group: with the exception of BMS status, participants in the control group must not differ significantly from those in the study group (matched for gender and age, individuals in the control group must have been selected from the study base); and 3) prospective design (i.e. data and samples must have been collected specifically for the study).
Each criterion was rated ‘met’, ‘unmet’ or ‘unclear’. Then we summarised the risk of bias of the studies using these three categories:
Low risk of bias: all criteria met; Moderate risk of bias: one or two criteria unclear; High risk of bias: at least one criterion unmet or three criteria unclear.
Statistical analysis
The data were analysed using Review Manager 5 (www.cochrane-net.org/revman). The primary analysis involved differences in the distributions of psychological factors between cases and controls. Dichotomous outcomes (e.g. presence/absence of anxiety or depression) were expressed as estimates of association, for which we used the OR and the 95% confidence interval (CI). Continuous outcomes (e.g. results of numerical scales) that relied on the same scale were expressed as the mean values and standard deviations (SDs) reported in the studies, yielding the estimate of effect as the mean difference (MD) with a 95% CI. Statistical heterogeneity was assessed with the I2, which has been conventionally adopted to indicate low, moderate and high heterogeneity values of 25%, 50% and 75%, respectively (23). As heterogeneity among studies was expected on the basis of large variability in the assessment of psychological factors across different studies, a random-effects model was used to calculate the summary estimate using the Mantel-Haenszel method for dichotomous outcomes and the inverse variance method for continuous outcomes (24,25). A sensitivity analysis was used to exclude studies with a high risk of bias. To investigate potential publication bias, the funnel plot of the results of the included studies was checked for asymmetry (26).
Results
Eligible studies
Overview of included studies.

BDI: Beck Depression Inventory; HADS: Hospital Anxiety and Depression Scale; ICHD: International Classification of Headache Disorders; GHQ: General Health Questionnaire; VAS: visual analogue scale; MMPI-II: Minnesota Multiphasic Personality Inventory-2; SCID-II: Structured Clinical Interview for DSM-IV Axis II Personality Disorders; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, fourth edition; MINI-PLUS: Mini International Neuropsychiatric Interview-PLUS; TAS: Toronto Alexithymia Scale; TCI: Temperament and Character Inventory; HAM-D/A: Hamilton Rating Scale for Depression/Anxiety; STAI: State-Trait Anxiety Inventory; SCL-90-R: Symptom Checklist-90-Revised.
Data on gender (138 females) was reported on the whole sample (N = 157).
Risk of bias.

BMS diagnosis
Only five studies (20,27–30) adopted the diagnostic criteria issued by the ICHD (1,31). The remainder of the studies diagnosed BMS based on ‘criteria included in the literature’ without specifying a time period or based on ‘exclusion criteria’.
Psychiatric and psychological factors
Most studies (Table 2) have examined psychiatric disorders, with a principal focus on anxiety and/or depression (12/14), using several different instruments: three studies used the Hospital Anxiety and Depression Scale (HADS) (3,31,33), three used the State-Trait Anxiety Inventory (STAI) (2,28,34), two used the Hamilton Rating Scale for Depression (HAM-D) (28,34), two used the Beck Depression Inventory (BDI) (28,29), one used the Beck Anxiety Inventory (BAI) (35), one used the Hamilton Anxiety Rating Test (HAM-A) (30) and the Montgomery-Asberg Depression Rating Scale (30), and another the Cattell’s Anxiety Test (36). Three studies examined broad psychopathological profiles: Two used the Mini International Neuropsychiatric Interview-PLUS (MINI-PLUS) (27,28), and one used the Symptom-Checklist-90-R (SCL-90-R) (34).
Five studies investigated the personality characteristics of BMS patients: One used mean scores on the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) Axis II Personality Disorders (SCID-II) (37), one used the NEO Personality Inventory (NEO PI-R) (38), one used the Minnesota Multiphasic Personality Inventory-2 (MMPI-2) (39), one used the Big Five Inventory (BFI) (27), and one used the Temperament and Character Inventory (TCI) (29). One study adopted the Toronto Alexithymia Scale-20 (TAS-20) (30), and one analysed current and historical life events with a qualitative interview (32).
Anxiety and depression
Most studies found evidence of an association between anxiety and depression and BMS. Only one study reported no evidence (according to mean of STAI scores) for the involvement of psychological factors in BMS (39), although this study focussed primarily on neurophysiological factors. The STAI and the HADS were the most commonly used tests (three studies each): trait and state anxiety was more prevalent in those with BMS than in healthy controls in two studies (28,34), and BMS patients met the criteria for pathological anxiety and depression (30,32,33) in all of the reviewed studies. Another study found that state and trait anxiety was associated with BMS according to mean scores on the Cattell’s Anxiety Test (40).
Anxiety
According to the three studies adopting the HADS (15,32) and BAI (35), anxiety was more common among those with BMS compared to controls. The pooled OR across the three studies was 2.64 (95% CI: 1.63–4.28), reflecting a significantly increased risk of anxiety among cases compared to controls (Figure 2). No heterogeneity was detected among such studies (I2 0%). Anxiety was measured in five studies using different diagnostic tools, including the HADS (23,28), Cattel’s Anxiety Scale (5), and STAI (state) (28,34). All studies found significantly higher levels of anxiety among those with BMS than controls. The pooled MD across studies remained statistically significant for the HADS, 3.38 (95% CI: 2.43–4.33), but not for the STAI (state), 10.53 (95% CI: −2.27 to 23.33), probably because of the significant heterogeneity between the two studies included (I2 92%) (Figure 3).
Forest plot of anxiety prevalence in BMS patients and controls. Forest plot of anxiety in BMS patients and controls.

Depression
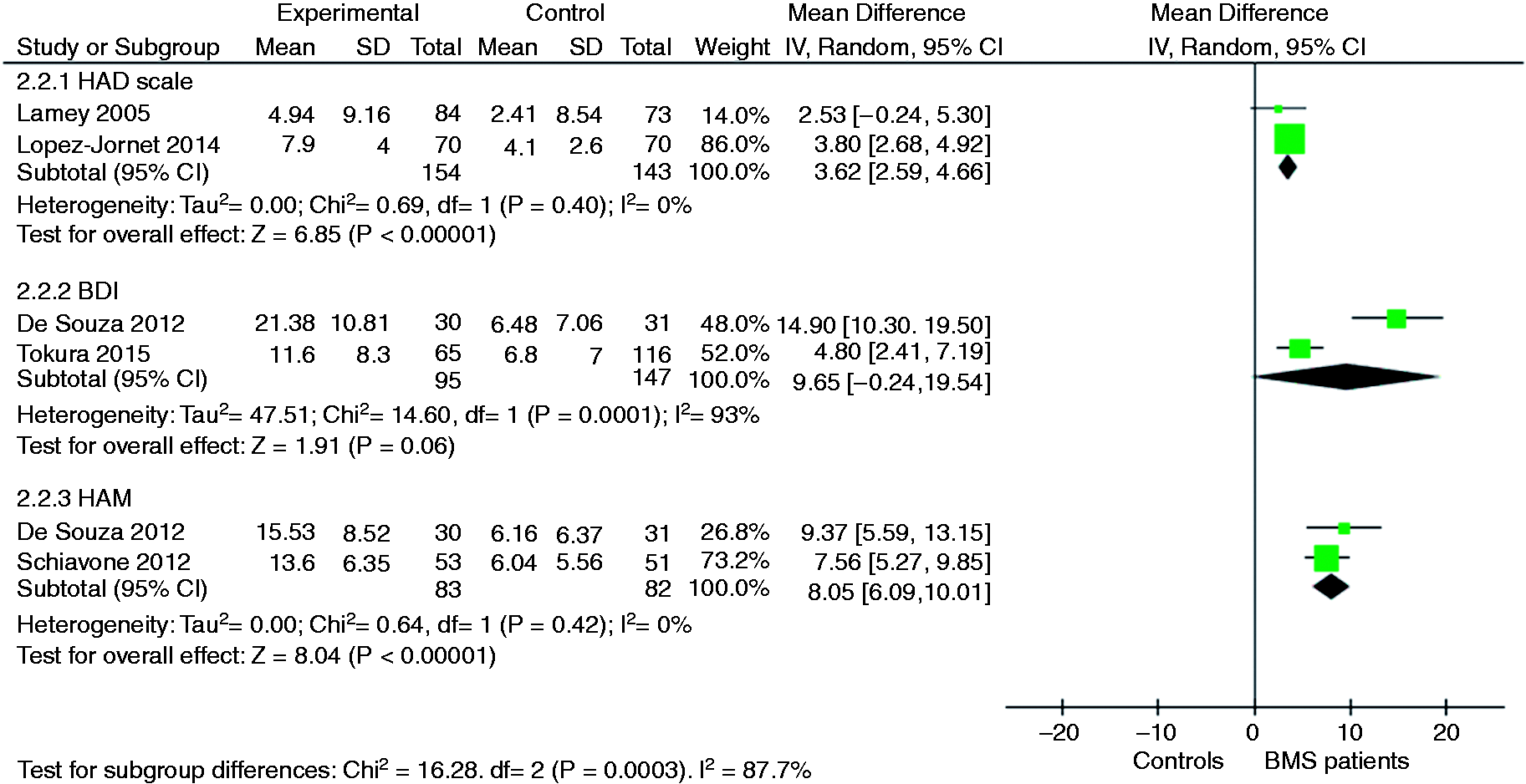
Two studies measured the prevalence of depression using the HADS (3,32). Their pooled OR was 3.18 (95% CI: 1.75–5.76), indicating a significantly increased risk of depression among cases compared to controls. No heterogeneity was detected among these studies (I2 0%) (Figure 4). Depression was measured by six studies using different diagnostic tools, including the HADS (23,28), BDI (28,29), and HAM-D (28,34). All studies found that depression was significantly more prevalent among those with BMS than among controls. The pooled MD across the studies remained statistically significant for the HADS, 3.62 (95% CI: 2.59–4.66), and the HAM-D, 8.05 (95% CI: 6.09–10.01), but not for the BDI, 9.65 (95% CI: −0.24 to 19.54), probably because of the significant heterogeneity between the two studies included (I2 93%) (Figure 5).
Forest plot of depression prevalence in BMS patients and controls. Forest plot of depression in BMS patients and controls.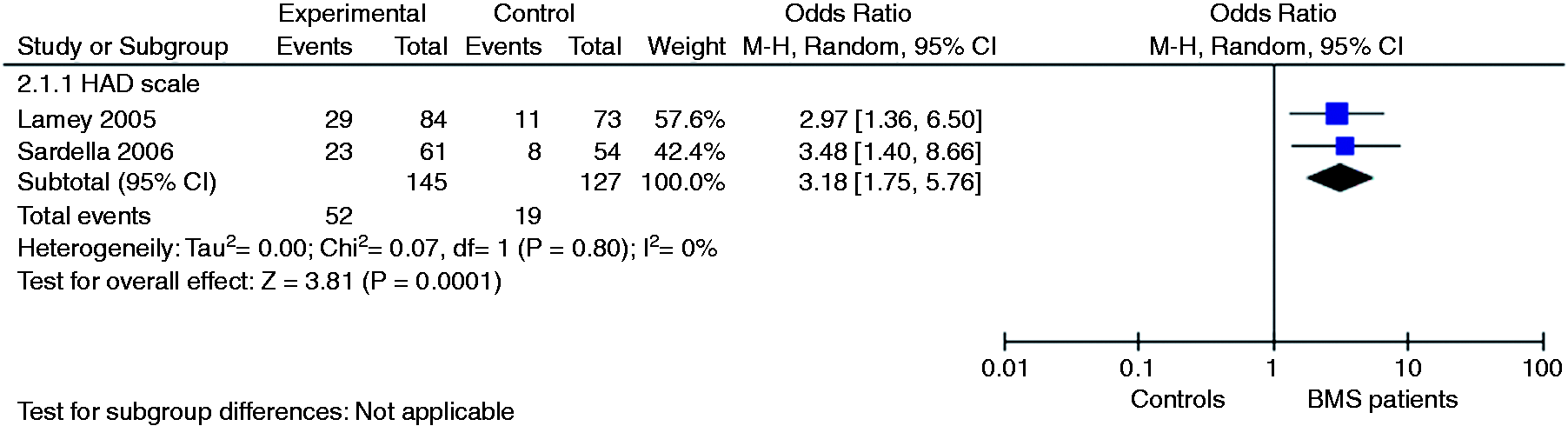
Other psychological factors
In terms of personality, we reviewed five studies using five different instruments (NEO Personality Inventory-Revised, SCID-II, MMPI-2, BFI, TCI) to assess personality: One did not find any differences between those with BMS and healthy controls (39), and the other four found higher levels of neuroticism (38,27) and harm-avoidance (11), lower levels of novelty seeking and self-directedness, and a greater prevalence of personality disorders (particularly obsessive-compulsive and schizotypal) in patients with BMS than in controls (37).
Two studies reported the presence of cancerophobia in BMS patients with contrasting findings (33,28).
Life events have been studied in the context of medical interviews and reported by one study (32).
Discussion
BMS is a clinically relevant form of chronic orofacial pain characterised by the absence of any detectable organic cause, and most likely, a complex aetiology. In this review, we present an overview of the role of psychological factors in this condition.
All reviewed studies but three found that psychological and/or psychiatric factors played a role in BMS. The psychopathological symptoms of patients with BMS have been the focus of more research than the personality or cognitive characteristics of this population.
Anxiety and depression (as measured by the STAI and HADS) seem to be the most common comorbid disorders among patients with BMS. The HADS is a self-report instrument for assessing anxiety and depression, but such variables are measured and quantified for the week ‘before the hospitalisation’. This meta-analysis further supports the role of anxiety and depression in BMS, but we need studies assessing psychological variables with instruments other than self-report measures that work well as screening measures, but are not diagnostic. However, the presence of mood and anxiety disorders has also been supported by few studies that adopted DSM-IV criteria and administered internationally validated structured clinical interviews, such as the MINI-plus (27,28). It is noteworthy that the few studies (41,42) that compared BMS patients with patients with other kinds of chronic pain (atypical facial pain and atypical odontalgia) did not clarify the specific aetiology of BMS, as they reported no differences between the prevalence of anxiety and depression between those with this condition and those with other conditions. Moreover, a study (43) that divided the sample into those with acute BMS, chronic BMS, or trigeminal neuralgia found a higher prevalence of depression (and somatisation) scores among those with the chronic form of BMS than in those with trigeminal neuralgia despite the fact that pain was rated as more severe by those with trigeminal neuralgia than by those with BMS. Anxiety and depression are common in patients affected by functional chronic pain disorders, such as irritable bowel syndrome, recurrent headache, fibromyalgia, chronic back pain, and chronic fatigue syndrome (44). The nature of the mechanism underpinning different kinds of chronic pain disorder is an intriguing matter of debate, and several hypotheses proposing different roles for genetic and epigenetic factors have been advanced (36). Like many other pain disorders, BMS involves chronic pain with a late age of onset (usually postmenopausal) and a clear prevalence in females, both of which contribute to the debate regarding the aetiology of BMS because they imply the involvement of hormonal factors. However, one interesting study (45) that compared premenopausal women, postmenopausal women, and men found inter-group differences in the clinical characteristics of BMS but not with regard to anxiety and depression. The question of whether anxiety and depression are causes or effects of BMS remains unanswered, but some evidence suggests that the former precede the latter. Where most studies assessed current symptoms (which probably biased the response towards concerns, anxiety, and demoralisation related to coping with new but chronic pain), others examined the history of psychopathological symptoms (27,28) and found that the onset of major depression, generalised anxiety disorder, and painful conditions other than orofacial disorders preceded the onset of BMS in almost 80% of cases (41). We propose that BMS is a kind of somatoform disorder that manifests in the elderly female population due to specific biological and/or psychological factors. Few studies (with contrasting findings) have analysed the occurrence of significant life events in BMS patients (32); however, such research might clarify the aetiology of BMS.
Only one study included in the present review analysed the role of alexithymia in BMS, and it found that 79.3% of BMS patients suffered from this condition. Alexithymia is a personality trait involving a dysregulation of negative affect (46) and is characterised by impaired symbolic thought, a restricted fantasy life, an externally oriented cognitive style, difficulty distinguishing feelings from bodily sensations, and impaired intuition and empathy (47). Alexithymia tends to be more prevalent in individuals with chronic pain (48), suggesting another element likely shared by BMS and other kinds of chronic pain.
Additional studies are warranted including epidemiological studies with prospective designs, to elucidate temporal patterns and causal relationships between psychological factors and BMS. A subset of psychological symptoms (other than anxiety and depression) may contribute importantly to the development and/or severity of BMS. We do not have studies linking psychological data to the severity of BMS.
Most studies regarding personality included in this review found a role for specific personality dimensions that may be related to BMS. As was the case for psychopathological assessments, many different instruments designed to detect different psychological constructs were adopted by the research included in this meta-analysis, rendering us unable to conclude anything other than that personality characteristics (e.g. neuroticism) play some role in BMS. As with anxiety and depression, several features of the personality of patients with BMS are shared by patients with other kinds of chronic pain. In particular, one study (11) found lower levels of self-directness and higher levels of harm avoidance in BMS patients than in controls; this is consistent with the results for those with other kinds of chronic pain (49) (e.g. fibromyalgia, migraine, tension-type headaches, nonspecific musculoskeletal disorders), but depression seems to play a specific role in BMS.
Further studies on BMS are needed to support and clarify the role of psychological factors other than anxiety and depression, address the interplay of specific cognitive and personality dimensions, and assess the possible contribution of life events. We stress the importance of a multidisciplinary approach to BMS; such an approach should involve a collaborative process between dentists or oral surgeons and clinical psychologists or psychiatrists from diagnosis to treatment. Patients with BMS suffer from pain and frequently frustration because of the unavailability of effective medications and the lack of understanding from friends and relatives. This condition requires appropriate attention and support because it may reflect psychological or psychiatric difficulties and/or have a serious impact on daily life.
Key findings
No systematic reviews and meta-analysis has been published on the role of psychological factors in burning mouth syndrome. The role of psychological factors is primary in burning mouth syndrome, but the mechanisms explaining it need to be addressed by further studies. Most studies evidenced a role for anxiety and depression, but personality and cognitive factors require more attention.
Footnotes
Acknowledgements
We are grateful to Dr Marco Margiotta for the preliminary assistance in data entry.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.