
Abstract
Background
Calcitonin gene-related peptide provokes migraine attacks in 65% of patients with migraine without aura. Whether aggregation of migraine in first-degree relatives (family load) or a high number of risk-conferring single nucleotide polymorphisms contributes to migraine susceptibility to calcitonin gene-related peptide infusion in migraine patients is unknown. We hypothesized that genetic enrichment plays a role in triggering of migraine and, therefore, migraine without aura patients with high family load would report more migraine attacks after calcitonin gene-related peptide infusion than patients with low family load.
Methods
We allocated 40 previously genotyped migraine without aura patients to receive intravenous infusion of 1.5 µg/min calcitonin gene-related peptide and recorded migraine attacks including headache characteristics and associated symptoms. Information of familial aggregation was obtained by telephone interview of first-degree relatives using a validated semi-structured questionnaire.
Results
Calcitonin gene-related peptide infusion induced a migraine-like attack in 75% (12 out of 16) of patients with high family load compared to 52% (12 out of 23) with low family load (P = 0.150). In addition, we found that the migraine response after calcitonin gene-related peptide was not associated with specific or a high number of risk-conferring single nucleotide polymorphisms of migraine without aura.
Conclusion
We found no statistical association between familial aggregation of migraine and hypersensitivity to calcitonin gene-related peptide infusion in migraine without aura patients. We also demonstrated that the currently known single nucleotide polymorphisms conferring risk of migraine without aura have no additive effect on calcitonin gene-related peptide induced migraine-like attacks.
Keywords
Introduction
Migraine is a very prevalent neurological disorder with a strong genetic basis (1,2). The genetic make-up in the most prevalent type of migraine, migraine without aura (MO), is complex, with many loci determining disease susceptibility (3,4). Aggregation of migraine in first-degree relatives of proband with migraine is a reasonable indicator of having a high genetic load (5,6). Moreover, a large genome-wide association study's meta-analysis has identified 12 single nucleotide polymorphisms (SNPs) conferring risk of MO (7). These SNPs may play a role in migraine pathophysiology, but their exact biological actions are unknown (7).
Pharmacological migraine provocation may be a novel approach to explore the contribution of genetics to migraine susceptibility (8). A previous study indicated that susceptibility of migraine-like headache to pharmacological provocation is associated with familial aggregation of migraine (9). In this study, provocation experiments were conducted in healthy volunteers and the International Headache Society (IHS) criteria for migraine were not used. Calcitonin gene-related peptide (CGRP) is one of the key molecules involved in migraine (10,11) and it induces migraine attacks in 60–65% of MO patients (12) but not in normal subjects (13). Whether this hypersensitivity to CGRP experienced by two-thirds of MO patients may be explained by genetic load, i.e. having aggregation of migraine in first-degree relatives (family load) or having a high number of risk-conferring SNPs (SNP load) is unknown.
In the present study, we hypothesized that MO patients with high family load would report more migraine attacks after intravenous infusion of human αCGRP than patients with low family load. We therefore conducted a randomized, balanced and double-blinded study in 40 genotyped patients with MO and obtained the migraine history of their first-degree relatives. In addition, we investigated whether specific or a high number of risk conferring SNPs could explain the sensitivity to CGRP.
Materials and methods
The patients were recruited from a cohort of 1010 unrelated MO patients from the Danish Headache Center, who were genotyped for the 12 identified SNPs associated with migraine (7). Our strategy was to recruit two groups of patients with the most difference in SNP load. Subsequently, we conducted a thorough telephone interview with first-degree relatives of the patients who completed the study. This approach allowed us to stratify patients into two groups based on family and SNP load.
As the SNPs are bi-allelic, each patient has zero, one or two risk alleles for each SNP; hence, the total numbers of at-risk alleles can theoretically range from none to 24. The lowest number of risk alleles was six and the highest number was 19. From our cohort, we recruited the 20 patients with the highest and lowest number of risk alleles, respectively. High and low SNP load definition was based on the number of risk alleles of the patients we ultimately included in the two groups. Thus, we ensured the most possible difference between the groups. One of our recent studies used the same method for definition of SNP load and found a difference in triptan response in migraine patients (14). In the present study, high SNP load was defined as patients identified with ≥ 14 risk alleles, whereas low SNP load was defined as patients identified with ≤ 9 risk alleles. For more information about the study population, phenotyping and genotyping of risk alleles, see supplementary material.
The history of migraine of the patient's first-degree relatives (parents, siblings and children) was obtained via a telephone interview based on a validated semi-structured questionnaire (15,16). Migraine (MO or with aura) were diagnosed according to the 3rd edition of the International Classification of Headache Disorders (17). Patients identified with ≥ 2 first-degree relatives with migraine were defined as having a high family load, whereas patients identified with ≤ 1 first-degree relatives with migraine were defined as having a low family load. Because migraine affects roughly 15% of people (18,19), having one first-degree relative with migraine is very likely due to chance. Trained research fellows who conducted the interviews were blinded in regard to the CGRP response and SNP load of the proband.
Design
We conducted a randomized, balanced and double-blinded study. Participants and research fellows, who performed all recordings, were blinded in respect of the genetic load. All subjects received a continuous intravenous infusion of 1.5 µg/min human α-CGRP (Calbiochem, Merck4Biosciences, Darmstadt, Germany) over 20 min as in our previous provocation studies (13,20,21).
Females were requested to be on sufficient contraception. Exclusion criteria were any other type of headache (except episodic tension-type headache ≤ 8 days per month); intake of any preventive medication (including migraine preventives); serious somatic or psychiatric diseases. A full medical examination and electrocardiography were performed on the day of the study. The patients were informed that CGRP might induce headache in some individuals, but the timing or the characteristics of headache was not discussed.
All participants gave written informed consent to participate in the study, which was approved by the Ethics Committee of Copenhagen (H-2-2011-141) and the Danish Data Protection Agency and conducted in accordance with the Helsinki II declaration of 1964, as revised in 2008. The study was registered at ClinicalTrials.gov (NCT01924052).
Experimental protocol
All participants arrived non-fasting at the clinic between 09:00 and 11:00 hours. They had to be without any kind of headache or intake of painkillers (including triptans) 48 h before the study day. A pregnancy test was performed at the beginning of each study day in all female patients. A venous catheter (Venflon®) was inserted into an antecubital vein for the administration of CGRP. The patients were kept in the supine position in quiet surroundings. After 15 min of rest, we measured the baseline (at 10 min before start of infusion (T−10) and at the time of infusion start (T0)) headache intensity and vital signs and started the infusion using an infusion pump (Braun Perfusor, Melsungen, Germany).
Headache intensity and questionnaire
Headache intensity was recorded at T−10 and then every 10 min up to 120 min after the start of infusion on a verbal rating scale (VRS) from 0 to 10 (22): 0 is no headache; 1 represented a very mild headache (including a sensation of pressing or throbbing or otherwise altered sensation in the head not associated with pain); 5 is headache of moderate intensity; 10 is the worst headache imaginable (23). Headache localization, characteristics and associated symptoms were also recorded. After discharge from the hospital, the patients were carefully instructed to continue recording their headache by a self-administered questionnaire every hour until 12 h after the start of infusion or until they went to bed. The questionnaire recorded headache characteristics and associated symptoms according to the IHS criteria (17) but also included questions concerning adverse events, premonitory symptoms (fatigue, yawning, stiff neck, mood swings) and if the reported headache mimicked the spontaneous migraine attacks. The patients were allowed to take their usual acute migraine medication at any time, but were instructed to take the medication when the head pain and associated symptoms mimicked their usual migraine attacks.
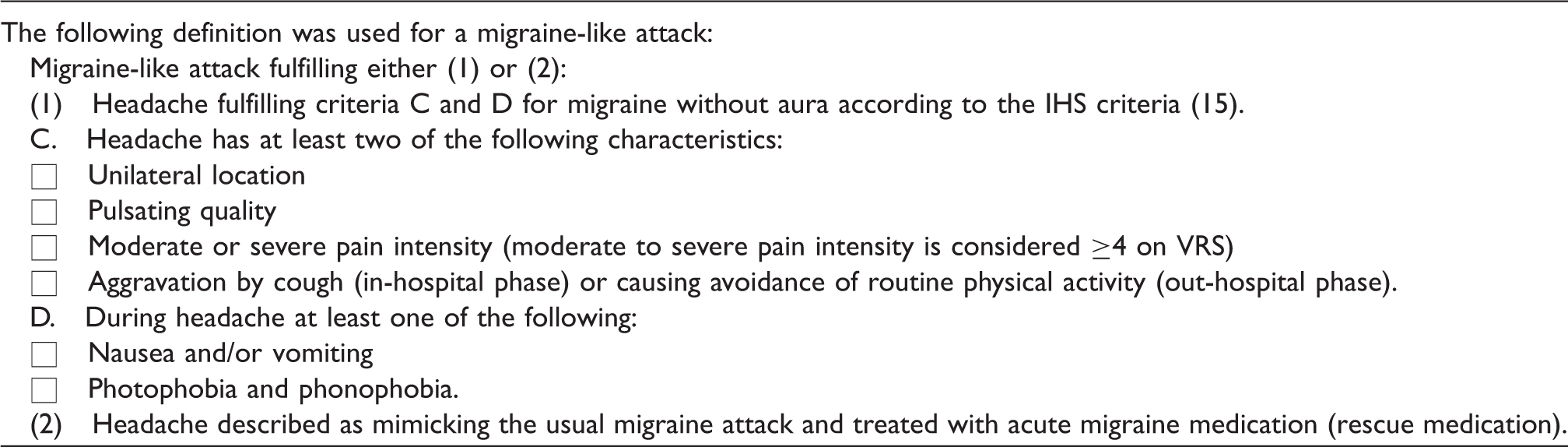
Migraine-like attack criteria
The following facts are important in defining criteria for an induced migraine-like attack. The majority of patients report them as attacks that mimic spontaneous migraine attacks (12,24). Second, it is well known that many spontaneous migraine attacks develop in a matter of hours and in the early stage phenomenologically only fulfil the criteria for tension-type headache before the headache gets worse, becomes unilateral and has the associated symptoms required for migraine. Third, most patients can predict the development of migraine in the early stage of the attack (25,26) and in a research study they cannot be denied treatment. Accordingly, the induced migraine attacks are often treated before all migraine criteria are fulfilled.
Vital signs
Heart rate (HR) and mean arterial blood pressure (MAP) were measured at baseline (T−10 and T0) and then every 10 min until 120 min after the start of infusion using an auto-inflatable cuff (Omega 1400, Orlando, FL, USA).
Statistical analysis
Headache intensity scores, peak headache intensity and median time to onset of migraine-like attacks after CGRP infusion were presented as median (range). HR and MAP data were presented as mean values ± SD.
Calculation of sample size was based on the difference between two groups reporting CGRP-induced migraine-like attacks after CGRP infusion (0–12 h), at 5% significance with 80% power. We assumed that CGRP would induce migraine-like attacks in at least 80% of patients with high genetic load as reported previously in common types of migraine (12) and migraine-like attacks in less than 20% of patients with low genetic load. We estimated that inclusion of at least 15 subjects in each group would be sufficient (http://biomath.info/power/ based on J.L. Fleiss, et al., Statistical Methods for Rates and Proportions).
The primary end-points were the difference in incidence of migraine-like attacks and the difference in area under the curve (AUC) for headache intensity scores (0–2 h and 2–12 h) between two groups. Secondary end-points were differences in incidence of any head pain, in AUC for MAP and HR during the in-hospital phase (0–2 h). We calculated AUC according to the trapezium rule (27) to obtain a summary measure to analyse the differences in response between the two groups of patients.
The incidence of migraine-like attacks, head pain, associated symptoms, premonitory symptoms and adverse events were analysed as categorical data with chi-square test except when the cell count was less than five then Fisher's exact test was applied. Difference in AUC for headache intensity scores were tested using the non-parametric Mann–Whitney U-test, while differences in AUC for HR and MAP values were tested with two-tailed unpaired Student's t-test.
Logistic regression analyses were performed with incidence of migraine-like attacks as the outcome variable and number of risk alleles as predictor variable. The incidence of migraine-like attacks and SNP load were analysed as categorical data by the chi-square test. Univariate logistic regression analyses were performed with migraine incidence as outcome and each SNP as predictor variable. We conducted an explorative analysis of the FHL5 variant and incidence of migraine-like attacks using the chi-square test. Association between family load and SNP load was analysed as paired categorical data with McNemar's test.
The P-values were not adjusted for multiple testing, age or sex because of insufficient sample size. All analyses were performed with SPSS Statistics version 19 for Windows (Chicago, IL, USA). P < 0.05 was considered the level of significance.
Results
Description of the two groups of patients with high or low family load who completed the study.

P-value: Fisher's exact test.
P-value: unpaired t-test.
P-value: Mann–Whitney U-test.
P-value: chi-square test.
The one subject without known relatives was excluded in the analysis for family load. Two patients with high family load and three patients with low family load had missing values in their headache intensity scores, because they went to bed or tried to sleep through the attack. Data at these time points were excluded from the statistical analysis and an extrapolation was done.
Migraine-like attacks and headache
Clinical characteristics and associated symptoms of the spontaneous (Spontan.) and provoked migraine attacks in the 12 migraine patients with high family load who developed migraine-like attacks.

NS: not stated.
Headache characteristics: Localization/intensity/quality (throb: throbbing; pres: pressing)/aggravation (by cough during in-hospital phase and by movement during out-hospital phase).
Associated symptoms: Nausea/photophobia/phonophobia.
Migraine-like attacks are defined according to criteria, described in Methods.
Treatment effect: Pain freedom or pain relief (≥50% decrease of intensity) within 2 h.
Clinical characteristics and associated symptoms of the spontaneous (Spontan.) and provoked migraine attacks in the 12 migraine patients with low family load who developed migraine-like attacks.

NS: not stated.
Headache characteristics: Localization/intensity/quality (throb: throbbing; pres: pressing)/aggravation (by cough during in-hospital phase and by movement during out-hospital phase).
Associated symptoms: Nausea/photophobia/phonophobia.
Migraine-like attacks are defined according to criteria, described in Methods.
Treatment effect: Pain freedom or pain relief (≥50% decrease of intensity) within 2 h.
CGRP infusion induced a migraine-like attack in 75% (12 out of 16) (95% confidence intervals (CI) 48–93%) of patients with high family load compared to 52% (12 out of 23) (95% CI 31–73%) with low family load (P = 0.150) (Figure 1). The incidence of migraine-like attacks and headache for all patients is described in Table 4. Median time to onset of migraine-like attacks in patients with high family load was 1.92 h (range 0.33–12 h) and in patients with low family load was 3.5 h (range 0.16–9 h)(P = 0.977).
Family load of the participating migraine patients (n = 39) and whether they got a migraine-like attack or not after CGRP infusion. High family was defined as ≥2 first-degree relatives with migraine, whereas no low family load was defined as ≤1 first-degree relatives with migraine. There was no significant difference in number of CGRP induced migraine-like attacks between MO patients with high and low family load (75% vs. 52%) (P = 0.150). Data are shown as % (n). Incidence of migraine–like attacks or headache after CGRP infusion among patients with high and low family load and number of patients who took rescue medication. Data are shown as % (n): number of patients. P-value: chi-square test. P-value: Fisher's exact test.
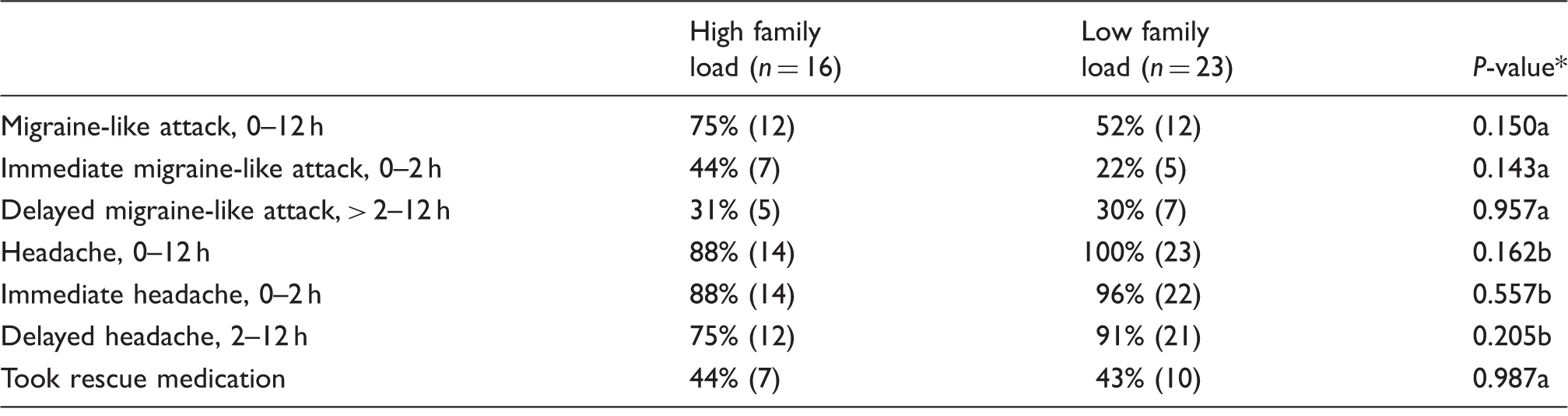
Median time to onset of immediate migraine-like attacks (0–2 h) was 30 min (range 20–120 min) for high load (n = 7) and 40 min (range 10–60 min) for low load (n = 5). Median time to onset of delayed migraine-like attacks (>2–12 h) was 8 h (range 8–12 h) for high load (n = 5) and 5 h (range 3–9 h) for low load (n = 7).
Median duration of migraine attacks for high load patients was 1 h (range 0.33–6.66 h), while median duration for low load was also 1 h (range 0.33–5.66 h). Seven out of 16 (44%) patients with high load took rescue medication compared to 10 out of 23 (43%) with low load (P = 0.751) (Table 4). Both high load and low load patients responded well to their rescue medication and had a significant reduction in headache intensity 2 h after treatment compared to baseline (P = 0.021 and P = 0.022). Median time of rescue medication intake for high load patients was 6 h (range 0.50–12 h) and 4.5 h (range 0.66–9 h) for low load patients.
Headache characteristics and associated symptoms 0–12 h after administration of CGRP.

Data are shown as % (n): number of patients.
P-value: chi-square test.
P-value: Fisher's exact test.
Flushing (100%), warm sensations (95%), palpitation (53%) and dizziness (33%) were the only adverse events reported and showed no difference between the two groups.
There was no statistical difference between the two groups in the incidence of any head pain or in the AUC for headache intensity over the 12 h observation period (Table 4 and Figure 2).
Median (thick line) and individual (thin lines) headache intensity on a 0–10 VRS for 16 migraine patients without aura with high family load (a) and 23 patients with low family load (b). Median peak headache score after CGRP was 4 (range 0–7) in patients with high family load and 5 (range 1–9) in patients with low family load. There was no difference in the AUC between high and low family load (AUC0-12 h: P = 0.120, AUC0-2 h: P = 0.520, AUC2-12 h: P = 0.100).
Subanalyses of SNPs
Among the 40 MO patients, 20 had a high SNP load and 20 had a low SNP load. Thirteen patients (65%) with high SNP load developed a migraine-like attack after CGRP compared to 12 patients (60%) with low load (P = 1.000). The median number of risk alleles (range) in patients with high SNP load was 14 (14–19) compared to 8 (6–9) in patients with low SNP load. We found no difference between the two groups in the AUC for headache intensity over the 12 h observation period (P = 0.947).
Logistic regression analyses showed no association between number of risk alleles and incidence of migraine-like attacks (P > 0.05). We also conducted analysis by categorizing number of risk alleles into two groups with high and low SNP load and found no difference. Moreover, we found no association between family load and SNP load (P = 0.677).
Incidence of migraine-like attacks showed no association with any particular SNP (P > 0.05). One of the 12 SNPs is the FHL5 variant (rs13208321), which encodes a transcription factor that regulates the cAMP response element-binding protein and cAMP-responsive element modulator (28). We hypothesized that this specific variant may affect CGRP sensitivity as CGRP activates the cAMP-dependent pathway (11). Twenty patients in our study were carriers of the FHL5 variant, but we found no association between the FHL5 variant and the development of migraine-like attacks after CGRP infusion (P = 0.752).
HR and MAP
We found no difference in HR and MAP between patients with high and low family load (HR AUC0-2 h, P = 0.658 and MAP AUC0-2 h, P = 0.787).
Discussion
We found that CGRP infusion statistically did not induce more migraine-like attacks among MO patients with high family load than in patients with low family load (75% vs. 52%). Patients with familial aggregation of migraine were more likely to develop nausea after CGRP infusion compared to patients with no family history of migraine and we found a trend toward higher incidence of throbbing headache in patients with high family load. However, we did not adjust for multiple testing. In addition, we found that a high number of the currently known SNPs or specific SNPs (i.e. the FHL5 variant) could not explain the hypersensitivity to CGRP infusion in MO patients.
Glyceryl trinitrate (GTN) is a nitric oxide donor and like CGRP is a known trigger of delayed migraine attacks (24). Sicuteri et al. (9) investigated 50 healthy volunteers and reported that induction of delayed migraine-like headache after intake of sublingual GTN was associated with familial predisposition of migraine. The authors demonstrated that participants with no family history of migraine did not develop delayed headache after provocation with GTN, whereas 29% (eight out of 28) of volunteers who had one or both parents suffering from migraine developed a delayed migraine-like headache. The migraine diagnosis of the parents was obtained by direct interviews with the parents according to the Ad Hoc Committee for Classification of Headache (29), but detailed information on headache characteristics and associated symptoms were not reported. These data suggest that the susceptibility of migraine attacks to pharmacological provocation might be explained at least partially by familial aggregation of migraine. In the present study, we found a nominally higher incidence of migraine attacks in patients with high family load compared to low family load, but it was not statistically significant. Our study may have insufficient power to detect small (25%) difference between groups. However, provocation studies are quite challenging (due to resources and practical reasons) and therefore we calculated sample size based on maximal (60%) clinically relevant difference.
Our definition of high family load was partly based on studies of other diseases showing that two first-degree relatives significantly increased the risk of disorder (30,31). Therefore, we think that two first-degree relatives may indicate genetic enrichment. However, it is important to acknowledge a potential limitation of the present study that we could not obtain contact with all first-degree relatives. Consequently, migraine diagnosis in 12 (out of 55) relatives was therefore based on reports from the proband or parents. Furthermore, we did not account for the number of siblings in our calculation of high and low family load. In addition, the clinical contribution of SNPs is difficult to assess because they explain only a tiny fraction of the genetic risk of migraine or only a small fraction of relevant risk variants has been discovered. Our negative findings may therefore not be very surprising as the effect sizes of the currently known SNPs are small and the interactions are complex. We do not know the exact mechanisms by which the 12 SNPs increase the risk of MO, as some of them are located within genes and some outside of genes. Nonetheless, it is a very interesting and novel way to investigate the additive effects of the SNPs. It would be plausible to investigate the relationship between SNPs and migraine response by looking at polygenic risk scores in a larger sample size, when further migraine-associated SNPs are discovered.
Our study strengths include use of direct telephone interview based on a validated semi-structured questionnaire to diagnose first-degree relatives (15,16) according to the latest IHS criteria (17). Direct interviews with each relative are required to obtain accurate information on migraine in families, because proband report is not sufficiently sensitive (32,33).
CGRP and migraine genetics
We have previously used the same CGRP model to investigate the functional consequences of migraine genetics showing that the monogenic familial hemiplegic migraine (FHM) is not hypersensitive to CGRP as seen in MO patients (21). The dominant genes causing FHM all affect ion-channels and glutamatergic neurotransmission (8,34). CGRP is thus unlikely to cause migraine via such mechanisms.
The clinical heterogeneity of migraine and the heterogenic response to CGRP infusion are caused by genetic, epigenetic or environmental factors. α-CGRP is encoded by the CALCA gene and the CGRP receptor consists of three separate subunits: calcitonin-like receptor, RAMP1, and receptor component protein (35,36). Given that CGRP and its receptor play crucial roles in migraine pathophysiology, it would be plausible to suggest an association between SNPs in the genes coding for CGRP or its receptor components and migraine. However, two recent studies showed no association between SNPs in the CALCA gene or the RAMP1 gene and migraine (37,38).
Conclusion
This is the first functional study of a relation between genetics of MO and migraine provocation. We found no association between familial aggregation of migraine and hypersensitivity to CGRP infusion in MO-patients. In addition, we demonstrated that the currently known SNPs associated with MO have no additive effect on CGRP-induced migraine response. With increasing knowledge of the genetic background to MO, this type of study may shed light on the phenotype-genotype relations of migraine in the future.
Article highlights
This is the first functional study of a relation between genetics of MO and migraine provocation Family history of migraine cannot explain the hypersensitivity of MO patients to CGRP infusion. SNPs cannot explain the hypersensitivity of MO patients to CGRP infusion.
Footnotes
Acknowledgements
The authors thank all participating patients, Ann-Louise Esserlind for scientific input and lab technicians Lene Elkjær, Winnie Grønning, medical student Christina Strand-Holm Manniche and Ditte Georgina Zhang for expert assistance. Further thanks to Lundbeck Foundation Center for Neurovascular Signaling (LUCENS), Novo Nordisk Foundation and Independent Research-Medical Sciences (FSS) and FP7-EUROHEADPAIN-no.602633.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jes Olesen has received grants and/or research support from, has been a consultant and/or scientific adviser for, and has been in the speakers' bureau of Allergan Inc, AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Janssen Pharmaceutical Products, Lundbeck, Merck, Amgen, Alder and Pfizer. Messoud Ashina is a consultant and/or scientific adviser/speaker for the ATI, Allergan, Amgen, Alder and Eli Lilly. Song Guo has received a travel grant from the ATI.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grants from Novo Nordisk Foundation (NNF11OC1014333), Independent Research-Medical Sciences (FSS) (DFF – 1331-00210A), and Lundbeck Foundation (R155-2014-171). The research leading to these results has received funding from the European Union's Seventh Framework programme (2007-2013) under grant agreement no. 602633.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.