
Abstract
Background
Haemodialysis arteriovenous fistulas have common local and regional complications, but are rarely associated with neurological symptoms.
Case report
A 43-year-old woman presented with short acute episodes of unilateral, non-throbbing, severe headache, vertigo and left lateropulsion. She had undergone renal transplantation and had a still-functioning left brachial arteriovenous fistula. No abnormality was detected on neurological examination or on brain parenchymal imaging. Colour Doppler ultrasonography showed a subclavian steal syndrome of the left vertebral artery and reversed flow in the left internal jugular vein. Ligation of the arteriovenous fistula had to be delayed as a result of renal graft dysfunction. Six months later she developed a headache attributed to intracranial hypertension. All symptoms subsided after ligation of the arteriovenous fistula.
Literature review
We identified 16 case reports of central neurological complications attributed to haemodialysis brachial fistulas. Headache descriptions were scarce and were not fully detailed.
Conclusions
The case of our patient suggests that unilateral, episodic, non-throbbing, non-postural headache with transient neurological symptoms can be caused by combined arterial and venous flow abnormalities secondary to a high-flow arteriovenous brachial fistula. In this setting, this pattern of headache may precede overt signs of intracranial hypertension and may be used as a warning sign of cerebral venous congestion.
Keywords
Introduction
Arteriovenous fistulas (AVFs) are regarded as the best type of haemodialysis access and are usually constructed using vessels in the upper limbs. The most common complications are local thrombosis and stenosis, arm steal syndrome, central vein stenosis and cardiac failure (1). Neurological complications are seldom reported and those caused by flow disturbances are rare and poorly characterized. The headache characteristics of these patients have been mostly neglected in case reports.
Central neurological symptoms in these patients have been attributed to two mechanisms: subclavian steal syndrome (2) and cerebral venous congestion (3). These mechanisms usually operate separately and have not been described in the same patient.
We report the case of a patient presenting with a distinctive headache and neurological symptoms with both arterial and venous flow disturbances. The published literature on the headache characteristics of neurological complications secondary to haemodialysis vascular access is reviewed.
Case report
We present the case of a 43-year-old woman with chronic kidney disease who had undergone renal transplantation in 2014 after seven years of haemodialysis. Her haemodialysis vascular access was a high-flow brachiocephalic AVF on her left arm. She had previously experienced stenosis of the left innominate vein, which had been treated by angioplasty on multiple occasions with recurring residual stenosis.
In March 2015 she presented with episodes of sudden unilateral headache on the left side with ipsilateral cervical irradiation, pressing/non-throbbing in quality and of severe intensity from the start. This headache was different from any previous headache she had experienced and was accompanied by rotational vertigo with a tendency to fall to her left side. The attacks were unprovoked, lasted for five minutes and resolved spontaneously while in the supine position, which did not worsen the headache. The frequency of the episodes ranged from one per week to three in the same day. She had pain, oedema and engorged tortuous veins on her left arm and supraclavicular region during the three days preceding the first headache episode. There were no associated symptoms such as nausea, vomiting, photophobia or phonophobia. There were no cranial autonomic symptoms.
She had previously had episodic migraine with visual aura since adolescence, which was infrequent (less than one episode per month), unilateral but on alternating sides, of moderate to severe intensity. The pain resolved with simple analgesic drugs and lasted one to three hours. She had never experienced sensory, speech, motor or possible brainstem or retinal symptoms with the headaches. She had not reported any episode in the previous five years. Her other past medical history was relevant for hypertension, diabetes, pre-eclampsia and allergy to both iodinated radiological contrast media and gadolinium. She was treated with tacrolimus, mycophenolate mofetil, prednisolone, prophylactic sulfamethoxazole and trimethoprim, carvedilol, linagliptin and esomeprazole.
Examination in the inter-critical period did not reveal any abnormality. Funduscopic examination excluded optic disc oedema. On the same day, a brain computed tomography scan was normal, but colour Doppler ultrasonography showed biphasic flow in the left vertebral artery, which was rendered monophasic and anterograde by temporary occlusion of the AVF with an inflated cuff, and reversed flow in the left internal jugular vein (IJV) and vertebral vein (Figure 1).
Colour Doppler ultrasonography findings: (a) at the beginning of symptoms with subclavian steal syndrome on the left vertebral artery (LVA) and (b) turbulent retrograde flow on the left internal jugular vein (LIJV); (c) after transient improvement of headache with disappearance of vertigo and improvement of early systolic flow on the LVA and (d) reduction of flow turbulence and velocity on the LIJV; (e) when signs of intracranial hypertension settled, but still showing sustained improvement of subclavian steal syndrome on the LVA and (f) slow retrograde flow on the LIJV; and (g) after ligation of the arteriovenous fistula with normalization of flow on the LVA and (h) marked decrease of retrograde flow in the LIJV.
Magnetic resonance imaging (MRI) showed no acute parenchymal lesion and a normal flow void signal on both lateral sinuses (Figure 2). MRI also showed integrity of the brainstem structures (Figure 3). Three-dimensional time-of-flight (TOF) arterial intracranial magnetic resonance angiography (MRA) demonstrated the patency of all intracranial arteries, but also flow signs on the left transverse and sigmoid sinuses and IJV, normally not depicted on this sequence. Two-dimensional TOF venous intracranial MRA did not detect any flow in the left IJV. However, a normal flow signal was present in this vein on a three-dimensional TOF arterial neck MRA (Figure 2). These findings, combined with colour Doppler ultrasonography, suggested that flow on the left internal jugular vein was oriented cranially.
(a) Axial diffusion, (b) axial T2 Fast spin echo (FSE) and (c) coronal T1 FSE showing normal parenchymal appreciation and a normal flow void signal on both lateral sinuses. (d) Three-dimensional time-of-flight (TOF) arterial intracranial magnetic resonance angiography (MRA), axial maximum intensity projection (MIP) reconstruction, depicting lateral left sinus opacification. (e) Two-dimensional TOF venous intracranial MRA, coronal MIP reconstruction, showing absent left internal jugular vein. (f) Three-dimensional TOF arterial neck MRA, sagittal MIP reconstruction, documenting left internal jugular vein signal (arrow). (a–c) Axial T2 fast spin echo (FSE) and (d, e) axial T2 fluid attenuation inversion recovery (FLAIR) scans showing normal parenchymal appreciation of the lower pons (a, d), upper pons (b, e) and midbrain (c, f).

Ligation of the AVF was proposed, but had to be delayed due to a diagnosis of a new spontaneous AVF within the renal graft. Meanwhile the headache episodes temporarily became milder and less frequent, albeit with the same headache characteristics, but were devoid of focal neurological signs. At this time, reversed flow in the left IJV decreased and became less turbulent (Figure 1).
In September 2015 the patient reported a change in the characteristics of the headaches. These were now holocephalic, daily, constant, of moderate intensity, with an acute sensation of stabbing on the left side, which irradiated down the left cervical region. The headaches worsened during the night due to her lying position and were accompanied by nausea and vomiting in the morning. Relief from analgesic drugs was only partial and short-lasting. Her neurological examination remained normal and funduscopic examination did not reveal papilloedema. Lumbar puncture was performed and her cerebrospinal fluid (CSF) pressure was 270 mm CSF with normal CSF analysis.
Immediate ligation of the brachial AVF was proposed and performed three days later, with prompt relief from the headaches. A timeline of the main clinical events is presented in Figure 4.
Timeline of headache characteristics and severity in relation to reversed internal jugular vein flow. AVF: arteriovenous fistula; IJV: internal jugular vein; star symbol: transient rotational vertigo with left lateropulsion.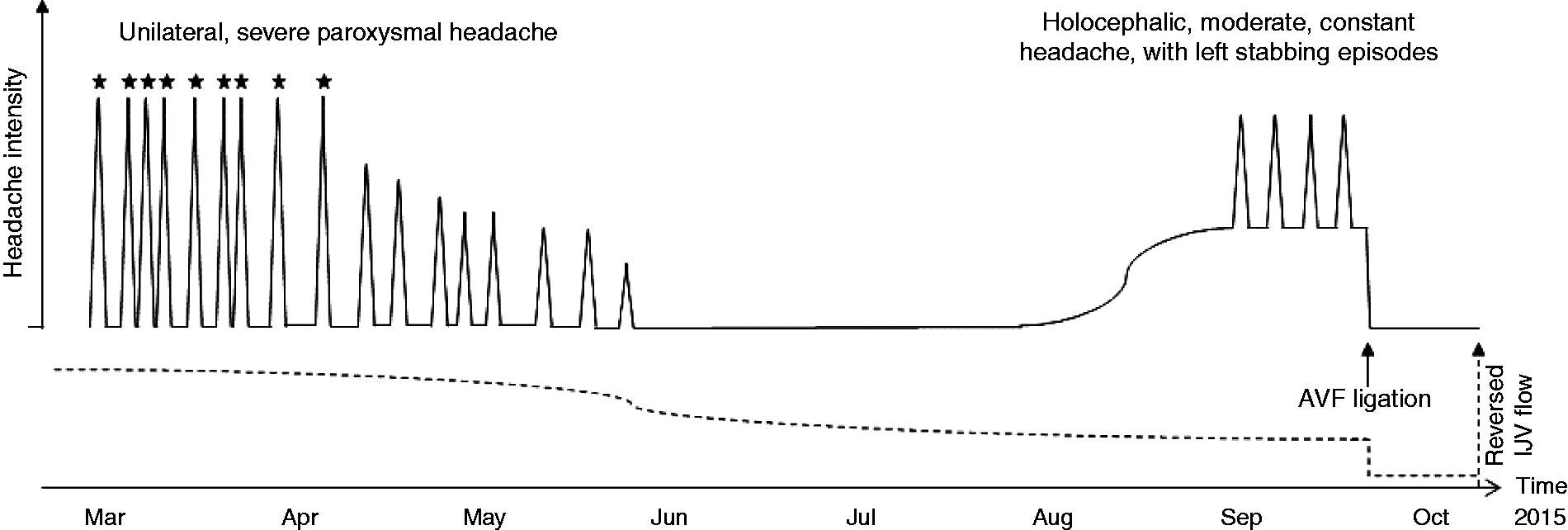
Literature review
Review of publications with central nervous system symptoms attributed to haemodialysis brachial fistulas.

CT: computed tomography; MRI: magnetic resonance imaging; SAH: subarachnoid haemorrhage.
We found 16 reported cases, 11 with retrograde venous flow on the IJV and five with vertebral artery retrograde flow. Only one of these case reports studied or reported both vertebral artery and jugular vein flows (4). Reports of headache in these patients were scarce and, when available, were not fully detailed (3–10) or described (6,11). Six case reports did not mention the presence of headache (2,8,12–15). Intracranial hypertension or hydrocephalus was reported in five of the 11 case reports with retrograde IJV flow (3,5,7,8,11).
Discussion
A new subtype of headache?
The case report presented here is, to the best of our knowledge, only the second published report of unilateral headache attributed to ipsilateral venous retrograde flow in the presence of upper limb AVF. However, the previous report was of a unilateral throbbing headache, possibly with another mechanism as its genesis because it did not occur in acute attacks, intracranial hypertension did not develop and it was ultimately related to a venous infarction (9). The headache reported here is noteworthy in terms of its characteristic features of being unilateral and side-locked, episodic, non-throbbing and not influenced by changes in position. It is also of special interest because it anticipated symptoms of overt intracranial hypertension, thereby serving as a potential warning sign.
We may be in the presence of a new headache eventually classifiable as attributed to cranial or cervical vascular disorder as described in the International Classification of Headache Disorders and fulfilling the general criteria for this headache type (16).
Our case report also featured typical characteristics of secondary headaches: a close temporal relation to the disorder (although we cannot relate the onset of the headache to increased AVF flow, the subsequent changes in headache frequency and intensity were synchronous with the AVF flow abnormalities) and the headache subsided after successful treatment of the causative disorder (17).
Pathophysiology
Previous reports have focused on the consequences of venous outflow impairment causing headache due to intracranial hypertension, brain oedema and venous infarction. We believe other mechanisms may better explain the headache in our patient.
The same-sidedness of the headache and the retrograde IJV flow allow us to postulate that they were both related, as the localization of the pain symptoms was congruent with the brain imaging findings of retrograde flow in the left transverse and sigmoid sinuses. The unilaterality of this headache may be conferred by the stimulation of pain receptors of the trigeminovascular system located in the wall of the venous sinuses (18) as a result of local flow inversion. Although this is the first time this aetiology has been proposed, we relied on previous knowledge of other disorders to make this assumption, such as intracranial dural AVF and arteriovenous malformations, where the headache and its putative mechanism are on the same side (16).
Later on the course of the disorder, before the closure of the AVF was possible, our patient’s symptoms shifted to a typical presentation of headache attributed to increased CSF pressure (16). As previously reported in patients with cerebral venous drainage obstruction, the augmented resistance in the venous outflow tracts generated an increase in cerebral venous back-pressure, causing impaired reabsorption of CSF across the arachnoid villi and leading to high CSF pressure (11). The continued impairment of cerebral drainage on the left side surpassed compensatory mechanisms in the brain and led to generalized intracranial hypertension. This later holocephalic headache with left stabbing episodic pain can result from continuous stimulation of the dural sinus caused by jugular venous flow impairment, with activation and sensitization of the trigeminovascular pathway (19) and intracranial hypertension. In this setting, our treatment option was immediate closure of the vascular access. Efficient decongestion of the cerebral venous system was shown by the reduction in flow velocities in the IJV and prompt relief of all symptoms of intracranial hypertension.
The colour Doppler ultrasonography findings of partial subclavian steal syndrome in the left vertebral artery are probably related to lower resistance in the left subclavian artery in the presence of the high-flow, low-resistance, brachial AVF (2). Retrograde vertebral artery flow with subclavian steal syndrome has been customarily associated with subclavian atherosclerotic stenosis, which was absent in our patient. Nevertheless, other infrequent aetiologies have also been reported, including high-flow brachial AVF steal, without relevant haemodynamic stenosis in the subclavian artery (20).
In this setting, we believe that the intermittent brainstem signs may have been related to vertebral artery insufficiency during episodes of higher demand. Headache during these episodes of vertigo and left lateropulsion may be caused by both arterial and venous mechanisms. The arterial contribution may be similar to that reported in connection with headache in posterior circulation acute stroke or transient ischaemic attack: dense perivascular innervation of the local intracranial vessels, ischaemia of the trigeminal nucleus leading to activation of the trigeminovascular system, dysfunction of the serotoninergic nuclei of the brainstem, or ischaemia of the dura partially supplied by the vertebral and basilar arteries (21). If we thought that these were the only mechanisms involved as a result of the simultaneous sudden onset of clinical symptoms of brainstem dysfunction, there should be no reason for the headache to continue after these symptoms had subsided. However, the patient continued to experience episodes of unilateral headache with the same features in the absence of neurological deficits. Thus we believe that venous mechanisms can better explain the continued episodes of headache.
Literature review
It is possible that similar disorders to that described here occurred in the previous case reports, but the focus on IJV abnormalities may have obscured concomitant vertebral artery abnormalities, which were probably under-reported. Of the two case reports with similar brainstem symptoms (3,12), only one reported vertebral artery flow changes (12). However, the paucity of these kinds of symptoms may indicate that, even if vertebral artery abnormalities are present, they are seldom symptomatic. On the other hand, when vertebral artery retrograde flow or occlusion was detected (2,4,10,12,13,15), only one study reported the flow direction in the IJV (4) and two reported the presence of headache, which in the first case may have been attributed to ischaemic stroke (4) and in the second case to intracranial hypertension (10). Therefore our patient’s symptoms reflect a combination of the two different pathophysiologies, which are infrequently described in the same patient.
Final remarks
Our patient’s headache proved to be secondary to cerebral venous outflow impairment in the presence of a high-flow AVF. Only the combination of subclavian steal syndrome and retrograde IJV flow can account for all the symptoms experienced by this patient. Contrary to other previously reported patients, the initial headache was not caused by intracranial hypertension. The unavoidable delay in closure of the AVF allowed us to follow the natural course of this disorder.
Clinical implications
Central venous stenosis is a common finding in patients undergoing haemodialysis and may be associated with retrograde IJV flow; subclavian steal syndrome can be caused by high-flow AVFs. It is rare for either disorder to present with neurological findings. Unilateral, episodic, non-throbbing, non-postural headache with transient focal neurological symptoms was caused by combined arterial and venous flow abnormalities secondary to a high-flow AVF. A specific pattern of headache may precede overt intracranial hypertension in haemodialysis patients with upper limb AVFs. With hundreds of thousands of patients receiving haemodialysis, this is useful as a warning sign of cerebral venous congestion before other signs of intracranial hypertension appear.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.